Orthopedic Ob Trauma D Review | Dr Hutaif Trauma & Frac -...
Key Takeaway
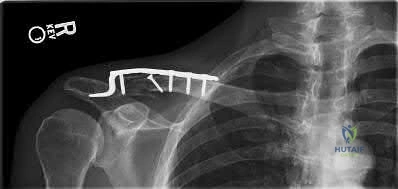
Discover the latest medical recommendations for ORTHOPEDIC MCQS ONLINE 20 OB TRAUMA 1D. A displaced midshaft clavicle fracture often presents with significant shortening and displacement, which a radiograph clearly shows an AP view of. These fractures are linked to decreased shoulder strength and high nonunion rates. Operative management, such as open reduction and internal fixation, significantly improves outcomes by reducing nonunion and enhancing functional recovery compared to non-operative care.
Orthopedic Ob Trauma D Review | Dr Hutaif Trauma & Frac -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 28-year-old male sustains a vertically oriented Pauwels type III femoral neck fracture after a high-energy fall. Which of the following fixation constructs provides the highest biomechanical stability to counteract shear forces for this specific fracture pattern?
Explanation

Question 2
A 45-year-old male is brought to the Emergency Department after a crush injury. He has an anteroposterior compression (APC-III) pelvic ring injury and is hemodynamically unstable. A pelvic binder is applied. Where must the pelvic binder be centered for maximal biomechanical effectiveness?
Explanation
Question 3
A 35-year-old male sustains a high-energy Schatzker VI tibial plateau fracture. On examination, he has tense swelling, and his compartment pressures in the anterior compartment measure 40 mmHg with a diastolic blood pressure of 65 mmHg. After performing emergent four-compartment fasciotomies, what is the most appropriate initial management of the fracture?
Explanation

Question 4
A 25-year-old male sustains a Hawkins type III talar neck fracture following an aviation accident. Which of the following accurately describes the displacement and the associated risk of avascular necrosis (AVN) for this specific injury pattern?
Explanation
Question 5
During open reduction and internal fixation of a distal femur fracture, a coronal plane fracture of the lateral femoral condyle (Hoffa fragment) is identified. To appropriately compress and fix this articular fragment, what is the ideal direction of the lag screws?
Explanation

Question 6
A 22-year-old male is involved in a high-speed motor vehicle collision. He presents with a closed midshaft femur fracture, bilateral pulmonary contusions, and a closed head injury (GCS 14). His initial BP is 90/60 mmHg, HR 120 bpm, lactate 4.5 mmol/L, and base deficit -8. After resuscitation with crystalloids and 2 units of packed RBCs, his lactate drops to 3.8 and base deficit to -6. What is the most appropriate management of his femur fracture?
Explanation
Question 7
A 40-year-old obese male presents to the Emergency Room after sustaining a low-velocity knee dislocation while playing basketball. The knee is currently reduced, and physical examination reveals a symmetric, palpable dorsalis pedis pulse. An ankle-brachial index (ABI) is performed, yielding a value of 0.85. What is the most appropriate next step in management?
Explanation

Question 8
A 65-year-old female sustains a displaced 3-part proximal humerus fracture. According to Hertel's criteria, which of the following fracture characteristics is the most critical predictor of subsequent avascular necrosis (AVN) of the humeral head?
Explanation

Question 9
A 32-year-old male sustains a closed transverse midshaft humerus fracture and presents with an immediate complete wrist drop. An initial attempt at closed reduction and functional bracing is performed. The radial nerve palsy persists immediately post-reduction. What is the most appropriate next step in the management of the radial nerve palsy?
Explanation
Question 10
A 42-year-old male requires open reduction and internal fixation of a highly displaced intra-articular calcaneus fracture via an extensile lateral approach. Which of the following neurological structures is most at risk during the creation of the full-thickness subperiosteal flap?
Explanation

Question 11
A 28-year-old motorcyclist sustains a Gustilo-Anderson Type IIIB open fracture of the middle third of the tibia. After thorough surgical debridement, a free tissue transfer will be required for coverage. According to established microsurgical trauma literature, what is the optimal timeframe for definitive soft tissue coverage to minimize infection rates and flap failure?
Explanation
Question 12
A 24-year-old football player presents with midfoot pain after an axial load force was applied to his plantar-flexed foot. Weight-bearing radiographs demonstrate a 3 mm diastasis between the base of the first and second metatarsals. What is the primary stabilizing structure disrupted in this classic Lisfranc injury?
Explanation

Question 13
A 7-year-old boy falls on an outstretched hand and sustains a Bado Type I Monteggia fracture-dislocation. Which of the following describes the correct anatomic configuration of a Bado Type I injury?
Explanation

Question 14
A 55-year-old female undergoes volar locking plate fixation for a comminuted distal radius fracture. Six months postoperatively, she presents to the clinic with an inability to actively flex the interphalangeal joint of her thumb. What is the most likely pathophysiological cause of her presentation?
Explanation

Question 15
A 30-year-old male sustains a posterior wall and posterior column acetabular fracture with a native hip dislocation following a dashboard injury. He requires surgical fixation. Which of the following surgical approaches is most appropriate for direct visualization and definitive fixation of these specific fracture components?
Explanation
Question 16
A 28-year-old male sustains an ankle fracture with a concomitant syndesmotic disruption. During operative fixation, a syndesmotic screw is planned. Which radiographic parameter on a perfect mortise view is considered the most reliable metric to intraoperatively assess the anatomic integrity of the syndesmosis?
Explanation

Question 17
A 24-year-old male presents with a closed, highly comminuted tibial shaft fracture. He complains of severe pain out of proportion to his injury. His clinical exam is equivocal due to his high anxiety. His blood pressure is 110/70 mmHg. Intracompartmental pressure testing is performed. Which of the following criteria provides the most accepted and specific threshold for performing a four-compartment fasciotomy?
Explanation

Question 18
A 45-year-old active smoker presents with persistent pain 9 months after intramedullary nailing of a closed tibial shaft fracture. Radiographs demonstrate a distinct fracture line with significant hypertrophic callus formation ('elephant foot' appearance) but lack bridging across the fracture site. What is the underlying cause of this specific type of nonunion?
Explanation

Question 19
A 38-year-old male sustains a severe APC-III pelvic fracture and arrives in hemorrhagic shock. Despite immediate pelvic binder application and massive transfusion protocol, he remains hypotensive and tachycardic. In the majority of pelvic ring injuries, what is the most common anatomic source of massive internal hemorrhage?
Explanation

Question 20
A 6-year-old girl falls from monkey bars and sustains a Gartland Type III extension-type supracondylar humerus fracture. On arrival, her hand is pink and warm, but she lacks a palpable radial pulse. Capillary refill is brisk (<2 seconds). Which of the following is the most appropriate initial management for this patient?
Explanation

Question 21
In the surgical management of a lateral Hoffa fracture (OTA/AO 33B3), which of the following statements regarding the biomechanics of fixation is most accurate?
Explanation
Question 22
A 45-year-old female presents after an MVC with a pelvic ring injury. Radiographs demonstrate a lateral compression injury.
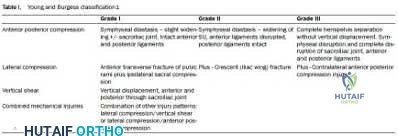
Which of the following specifically defines an LC-II injury according to the Young-Burgess classification?
Explanation
Question 23
A 32-year-old man sustains an acetabular fracture. CT scan reveals a fracture line separating the anterior half of the innominate bone from the intact posterior ilium, associated with a transverse fracture line through the posterior column. Which Letournel classification best fits this pattern?
Explanation
Question 24
In the evaluation of a complex tibial pilon fracture, the anterolateral fragment is frequently avulsed. What ligamentous structure attaches to this specific fragment?
Explanation
Question 25
A 28-year-old male sustains a displaced talar neck fracture with subluxation of the subtalar joint, while the tibiotalar and talonavicular joints remain congruous. According to the Hawkins classification, what is the type and approximate historical risk of avascular necrosis (AVN)?
Explanation
Question 26
A 42-year-old construction worker falls from a height and sustains a closed, displaced intra-articular calcaneus fracture. The Sanders classification is utilized for operative planning. Which specific anatomic structure is the primary landmark used to determine the Sanders classification?
Explanation
Question 27
A 24-year-old athlete sustains a hyperplantarflexion injury to the midfoot. Radiographs demonstrate subtle widening between the 1st and 2nd metatarsal bases and a "fleck sign."
The "fleck sign" typically represents an avulsion of the Lisfranc ligament from which structure?
Explanation
Question 28
In evaluating a displaced proximal humerus fracture, which of the following radiographic criteria (Hertel criteria) is the most reliable predictor of ensuing avascular necrosis (AVN) of the humeral head?
Explanation
Question 29
A 30-year-old male presents with a closed spiral fracture of the distal third of the humeral shaft resulting from a throwing injury. On examination, he is unable to extend his wrist or fingers. Which of the following is the most appropriate initial management?
Explanation
Question 30
A fracture involving the capitellum and the lateral half of the trochlea in a single piece, with associated posterior condylar comminution, is evaluated on a CT scan.
According to the Dubberley classification, this is classified as:
Explanation
Question 31
A 6-year-old child presents with a hyperpronation injury to the forearm. Radiographs reveal a fracture of the proximal ulna with an associated radial head dislocation. The radial head is dislocated laterally. According to the Bado classification, what type of Monteggia lesion is this?
Explanation
Question 32
A 40-year-old female presents after falling on an outstretched hand, sustaining a "terrible triad" injury of the elbow.
Which of the following accurately describes the typical sequence of surgical repair for this injury?
Explanation
Question 33
A 35-year-old male is struck by a motor vehicle and sustains a closed pelvic ring injury. Examination reveals a large, fluctuant area over the greater trochanter with overlying skin hypermobility and bruising. An MRI confirms a hemolymphatic fluid collection between the subcutaneous fat and the underlying fascia. What is the most appropriate initial management of this soft tissue injury to prevent deep infection prior to definitive internal fixation?
Explanation
Question 34
In the evaluation of a patient with a severe tibial shaft fracture, acute compartment syndrome is suspected. Intracompartmental pressure measurements are obtained. Which of the following parameters is considered the most reliable indicator for performing a fasciotomy?
Explanation
Question 35
A 25-year-old male sustains a gunshot wound to the thigh with a fractured femoral shaft. The weapon was a high-velocity military rifle. Which of the following principles best guides the management of the soft tissues in this injury?
Explanation
Question 36
A 38-year-old man sustains an open fracture of the tibia. There is a 12 cm laceration with extensive muscle stripping and a segmental fracture pattern. Pulses are non-palpable distally, and an angiogram demonstrates a complete transection of the popliteal artery requiring a saphenous vein graft repair. According to the Gustilo-Anderson classification, what is the grade of this open fracture?
Explanation
Question 37
In the polytraumatized patient, the concept of "Damage Control Orthopedics" (DCO) is often employed to minimize the "second hit" phenomenon. Which of the following physiologic parameters would most strongly indicate the need for DCO rather than Early Total Care (ETC) for a femoral shaft fracture?
Explanation
Question 38
An 82-year-old female sustains a non-displaced femoral neck fracture. To minimize mortality and morbidity, national guidelines recommend that surgical intervention should ideally be performed within what timeframe from admission?
Explanation
Question 39
A 25-year-old male sustains a femoral neck fracture.
The fracture line is oriented 75 degrees relative to the horizontal. According to the Pauwels classification, this is a Type III fracture. Which of the following statements best describes the biomechanical forces and optimal fixation strategy for this fracture?
Explanation
Question 40
A 45-year-old male presents with a high-energy medial tibial plateau fracture (Schatzker IV). This fracture pattern is frequently a result of a high-energy varus/axial load. Which of the following injuries is most strongly associated with this specific fracture pattern, requiring careful clinical assessment?
Explanation
Question 41
Proximal third tibial shaft fractures treated with intramedullary nailing in extension are classically associated with which of the following malalignments?
Explanation
Question 42
A 35-year-old polytrauma patient with bilateral femur fractures presents with a lactate of 4.5 mmol/L, pH 7.2, and base excess of -8. According to Damage Control Orthopedics (DCO) principles, what is the most appropriate initial management of the femur fractures?
Explanation
Question 43
During the surgical approach for a terrible triad injury of the elbow, what is the generally recommended sequence of reconstruction to restore elbow stability?
Explanation
Question 44
A 40-year-old male sustains a Type IIIB open tibial shaft fracture. Following initial debridement and external fixation, when is the optimal time for definitive soft tissue coverage to minimize infection risk?
Explanation
Question 45
In the management of a displaced Hoffa fracture (coronal shear fracture of the femoral condyle), what is the optimal direction of lag screw placement for maximum biomechanical stability against physiological forces?
Explanation
Question 46
A patient with a displaced posterior wall acetabular fracture presents with a foot drop preoperatively. Which nerve division is most commonly injured in this scenario?
Explanation
Question 47
Which ligament is considered the strongest and most critical for maintaining the structural stability of the Lisfranc complex?
Explanation
Question 48
Eight weeks following open reduction and internal fixation of a Hawkins Type II talar neck fracture, an AP radiograph demonstrates a subchondral radiolucent band in the talar dome. What does this finding indicate?
Explanation
Question 49
When utilizing an extensile lateral approach for a displaced intra-articular calcaneus fracture, the surgical flap relies primarily on which of the following vessels for its blood supply?
Explanation
Question 50
In a patient with recurrent anterior shoulder instability, advanced 3D imaging reveals 25% anterior glenoid bone loss. Which of the following is the most appropriate definitive surgical intervention?
Explanation
Question 51
A patient undergoes volar plating for a distal radius fracture. Postoperatively, the patient develops an attrition rupture of the flexor pollicis longus (FPL) tendon. This complication is most commonly associated with plate placement distal to which anatomical landmark?
Explanation
Question 52
A patient presents with severe leg pain following a closed tibial shaft fracture. Which of the following findings is the most reliable early clinical indicator of acute compartment syndrome?
Explanation
Question 53
A patient sustains a high-energy pelvic ring injury. During surgical exploration via an ilioinguinal approach, massive hemorrhage occurs near the superior pubic ramus. Which vascular structure is most likely injured?
Explanation
Question 54
According to the Denis classification of sacral fractures, fractures occurring in Zone 3 are most commonly associated with which of the following complications?
Explanation
Question 55
A young adult sustains an isolated transverse fracture of the scaphoid waist. What is the primary anatomical reason this fracture pattern carries a high risk for avascular necrosis of the proximal pole?
Explanation
Question 56
A 25-year-old male sustains a traumatic knee dislocation. Following closed reduction, the patient has palpable pedal pulses but an Ankle-Brachial Index (ABI) of 0.8. What is the most appropriate next step in management?
Explanation
Question 57
A 65-year-old female sustains a subtrochanteric femur fracture. Biomechanically, what is the primary deforming force causing flexion and external rotation of the proximal fracture fragment?
Explanation
Question 58
A 30-year-old patient with an open Type IIIA diaphyseal femur fracture undergoes immediate intramedullary nailing. What is the current consensus regarding the optimal duration of prophylactic antibiotic therapy after definitive wound closure?
Explanation
Question 59
A 22-year-old male presents with a gunshot wound to the right knee. Radiographs reveal a retained bullet directly within the intra-articular space, with a minimally displaced osteochondral fracture. What is the recommended management?
Explanation
Question 60
In a patient with a suspected syndesmotic injury following an ankle fracture, intraoperative fluoroscopy is used to perform a "Cotton test." Which maneuver accurately describes this test?
Explanation
Question 61
A 32-year-old male presents with a Hawkins type III talar neck fracture following a motor vehicle collision. Which of the following best describes the specific vascular disruption that places him at an 80-100% risk for avascular necrosis?
Explanation
Question 62
During open reduction and internal fixation of a comminuted posterior wall acetabular fracture, an area of marginal impaction is identified. What is the most appropriate management of this articular fragment?
Explanation
Question 63
A 40-year-old female sustains a distal femur fracture. CT imaging reveals a coronal plane fracture of the lateral femoral condyle (Hoffa fracture). Which of the following fixation strategies provides the most biomechanically stable construct for this specific fragment?
Explanation
Question 64
A 25-year-old male polytrauma patient with bilateral femoral shaft fractures and a severe pulmonary contusion has a serum lactate of 4.5 mmol/L and a base deficit of -8. According to damage control orthopedics (DCO) principles, what is the most appropriate initial skeletal management?
Explanation
Question 65
When treating a proximal third extra-articular tibia fracture with an intramedullary nail, the fracture is at highest risk for which of the following post-operative malalignments?
Explanation
Question 66
A 50-year-old male sustains a subtrochanteric femur fracture. During closed reduction, the proximal fragment is noted to be severely displaced. Which combination of muscles is responsible for the classic flexion, abduction, and external rotation deformity of the proximal segment?
Explanation
Question 67
In the surgical treatment of a displaced intra-articular calcaneus fracture, the 'constant fragment' remains anatomically aligned with the talus. Which structure provides the primary ligamentous attachment holding this fragment in place?
Explanation
Question 68
According to the Lower Extremity Assessment Project (LEAP) study, which of the following is the most significant predictor of poor long-term functional outcome following severe, limb-threatening lower extremity trauma?
Explanation
Question 69
A 65-year-old female who has been taking alendronate for 8 years presents with severe, progressive right thigh pain. Radiographs reveal cortical thickening and a transverse radiolucent line on the lateral cortex of the subtrochanteric femur, but no complete fracture. What is the most appropriate management?
Explanation
Question 70
Recent quantitative anatomical studies (e.g., Hettrich et al.) have redefined the primary arterial blood supply to the humeral head. Which vessel provides the majority of the blood supply to the humeral head, putting it at risk for avascular necrosis in 4-part proximal humerus fractures?
Explanation
Question 71
A 30-year-old male sustains a closed, spiral fracture of the distal third of the humeral shaft (Holstein-Lewis fracture). On initial presentation in the emergency department, his radial nerve function is intact. Following a closed reduction and application of a coaptation splint, he develops a complete wrist drop and inability to extend his fingers. What is the most appropriate next step in management?
Explanation
Question 72
A 40-year-old male involved in a high-speed motor vehicle collision sustains an isolated intra-articular distal femur fracture. CT imaging demonstrates a coronal plane fracture of the lateral femoral condyle (Hoffa fracture). Which fixation strategy offers the highest biomechanical stability for this specific fragment?
Explanation
Question 73
A 25-year-old polytrauma patient (ISS 45) presents with bilateral closed femoral shaft fractures, severe bilateral pulmonary contusions, and a pelvic ring injury. His initial serum lactate is 4.5 mmol/L, base deficit is 8 mEq/L, and temperature is 34.5°C. What is the most appropriate initial management of his femoral fractures?
Explanation
Question 74
A 45-year-old male sustains a pelvic injury after being struck by a vehicle from the side. Pelvic radiographs and CT demonstrate an internal rotation deformity of the hemipelvis with a fracture extending from the sacroiliac joint through the posterior iliac wing. How is this injury classified according to the Young-Burgess system?
Explanation
Question 75
An 8-week follow-up radiograph of a 25-year-old patient who sustained a talar neck fracture shows a distinct subchondral radiolucent band running across the talar dome. What does this radiographic finding signify?
Explanation
Question 76
A 35-year-old construction worker falls from a ladder and sustains a displaced intra-articular calcaneus fracture. The surgeon elects to perform an open reduction and internal fixation via an extensile lateral approach. Which of the following is the most common complication specifically associated with this surgical approach?
Explanation
Question 77
A 22-year-old collegiate football player presents with severe midfoot pain after a plant-and-twist injury. Weight-bearing radiographs reveal a 3 mm widening between the base of the first and second metatarsals. The primary ligament disrupted in this injury normally connects which two anatomic structures?
Explanation
Question 78
A 45-year-old female falls onto an outstretched hand with her wrist in palmar flexion. Radiographs demonstrate a fracture of the volar margin of the distal radius with associated volar subluxation of the carpus. What is the eponymous name for this fracture pattern?
Explanation
Question 79
Why is a fracture through the proximal pole of the scaphoid at a significantly higher risk for nonunion and avascular necrosis compared to a distal pole fracture?
Explanation
Question 80
A 60-year-old male sustains a basicervical femoral neck fracture. From a biomechanical and treatment perspective, how should this specific fracture pattern be managed?
Explanation
Question 81
A 30-year-old male sustains a low-velocity gunshot wound to the thigh resulting in a comminuted midshaft femur fracture. The bullet passed cleanly through the thigh, and the patient has no vascular deficits. What is the most appropriate management of the fracture?
Explanation
Question 82
A 28-year-old male is admitted with a comminuted tibial shaft fracture. He complains of excruciating leg pain unresponsive to intravenous opioids. His current blood pressure is 110/60 mmHg. Intracompartmental pressure testing of the anterior compartment yields a measurement of 45 mmHg. What is the Delta P (ΔP), and what is the indicated treatment?
Explanation
Question 83
A 40-year-old male sustains a high-energy OTA/AO 43-C3 pilon fracture. On presentation, the soft tissues about the ankle are severely swollen with multiple fracture blisters. What is the most appropriate initial management?
Explanation
None
