Full Question & Answer Text (for Search Engines)
Question 1:
A 35-year-old male presents after an MVC with a systolic BP of 75 mmHg. Heart rate is 135 bpm. FAST scan is negative. Pelvic radiograph shows an APC-III pelvic ring injury. A pelvic binder is applied. Fluid resuscitation is initiated but his BP remains 80 mmHg. What is the most appropriate next step in management?
Options:
- CT abdomen and pelvis with IV contrast
- Pelvic angiography with embolization
- Pre-peritoneal pelvic packing and external fixation
- Laparotomy
- Retrograde urethrogram
Correct Answer: Pre-peritoneal pelvic packing and external fixation
Explanation:
In a hemodynamically unstable patient with a pelvic ring injury and a negative FAST (ruling out intra-abdominal bleeding), the source of bleeding is likely the pelvis (venous or arterial). If the patient remains unstable despite a pelvic binder and initial fluid resuscitation, emergent mechanical stabilization (e.g., external fixation) and pre-peritoneal pelvic packing (PPP) is indicated. Currently, ATLS/AAOS guidelines support PPP + Ex-Fix as a rapid, definitive initial step in the operating room for venous bleeding (which accounts for ~80% of pelvic hemorrhage), often followed by angio if bleeding persists.
Question 2:
A 22-year-old motorcyclist presents after a high-speed collision. He has a mangled, pulseless left upper extremity with massive swelling over the shoulder and chest wall. Radiographs show lateral displacement of the scapula with a widened sternoclavicular joint. What is the most likely neurologic injury associated with this pattern?
Options:
- Complete brachial plexus avulsion
- Axillary nerve transection
- Spinal accessory nerve palsy
- Long thoracic nerve neurapraxia
- Isolated ulnar nerve injury
Correct Answer: Complete brachial plexus avulsion
Explanation:
Scapulothoracic dissociation is a high-energy injury characterized by complete disruption of the scapulothoracic articulation. It is associated with severe neurovascular injuries, most notably complete brachial plexus avulsion (which occurs in up to 80% of cases) and subclavian/axillary artery disruption. The presentation typically involves a pulseless, flail upper extremity and lateral displacement of the scapula on chest X-ray.
Question 3:
Which of the following radiographic findings is most predictive of avascular necrosis (AVN) following a complex 4-part proximal humerus fracture?
Options:
- Disruption of the medial periosteal hinge (calcar length < 8 mm)
- Greater tuberosity displacement > 5 mm
- Varus angulation of 15 degrees
- Involvement of the bicipital groove
- Shortening of the surgical neck > 10 mm
Correct Answer: Disruption of the medial periosteal hinge (calcar length < 8 mm)
Explanation:
Hertel et al. described radiographic predictors for humeral head ischemia (and subsequent AVN) in proximal humerus fractures. The most significant predictors include a medial metaphyseal head extension (calcar length) of less than 8 mm, disruption of the medial periosteal hinge, and basicervical fracture patterns. Disruption of the medial periosteal hinge eliminates the protection to the ascending branch of the anterior humeral circumflex artery and intraosseous collateral vessels.
Question 4:
A 28-year-old male sustains severe bilateral femur fractures, multiple rib fractures, and bilateral pulmonary contusions in an MVC. Upon arrival, his serum lactate is 5.5 mmol/L, base deficit is -9, and pH is 7.21. After initial resuscitation, his lactate remains at 4.2 mmol/L. What is the most appropriate management for his femur fractures?
Options:
- Immediate bilateral intramedullary nailing
- Bilateral external fixation (Damage Control Orthopedics)
- Intramedullary nailing of one femur, external fixation of the other
- Non-operative management with skeletal traction for 6 weeks
- Open reduction and internal fixation with plates
Correct Answer: Bilateral external fixation (Damage Control Orthopedics)
Explanation:
This patient presents with polytrauma and remains physiologically 'borderline' to 'in extremis' based on his persistent lactic acidosis, base deficit, and pulmonary contusions. Early Total Care (ETC) with reamed intramedullary nailing can exacerbate the systemic inflammatory response syndrome (SIRS), leading to acute respiratory distress syndrome (ARDS), the 'second hit' phenomenon. Damage Control Orthopedics (DCO) using temporary external fixation is indicated to provide skeletal stability while minimizing the physiological burden.
Question 5:
A 30-year-old male sustains a Pauwels type III femoral neck fracture. To maximize biomechanical stability and reduce the risk of non-union, which of the following internal fixation constructs is most appropriate?
Options:
- Three parallel cancellous screws
- Two parallel cancellous screws
- A sliding hip screw (SHS) with an anti-rotation screw
- A dynamic condylar screw (DCS)
- Hemiarthroplasty
Correct Answer: A sliding hip screw (SHS) with an anti-rotation screw
Explanation:
Pauwels type III fractures have a vertical fracture line (angle > 50 degrees), which creates high shear forces across the fracture site, predisposing them to non-union and varus collapse. While parallel cancellous screws are commonly used for more horizontal (Pauwels I or II) fractures, a sliding hip screw (with or without an anti-rotation screw) or a proximal femoral locking plate provides better biomechanical stability against vertical shear forces. The addition of an anti-rotation screw to an SHS construct is highly recommended in young patients.
Question 6:
A 45-year-old male suffers a Gustilo-Anderson IIIB open tibia fracture with a 10 cm soft tissue defect over the distal third of the tibia, exposing the bone without periosteal coverage. After serial debridements and skeletal stabilization, what is the most appropriate soft tissue coverage option?
Options:
- Split-thickness skin graft
- Medial gastrocnemius rotational flap
- Soleus rotational flap
- Free tissue transfer (e.g., anterolateral thigh or latissimus dorsi flap)
- Reverse sural artery flap
Correct Answer: Free tissue transfer (e.g., anterolateral thigh or latissimus dorsi flap)
Explanation:
Soft tissue defects over the distal third of the tibia that expose bone lacking periosteum require robust coverage. Rotational muscle flaps are geographically limited: the medial gastrocnemius covers the proximal third, and the soleus covers the middle third of the tibia. For the distal third, a free tissue transfer (such as an ALT, gracilis, or latissimus dorsi flap) is the gold standard for reliable coverage. A reverse sural flap is an option for smaller defects, but a 10 cm defect typically necessitates a free flap.
Question 7:
A 65-year-old female sustains a subtrochanteric femur fracture. During closed reduction prior to intramedullary nailing, the proximal fragment is noted to be flexed, abducted, and externally rotated. Which muscle groups are primarily responsible for this classic deformity?
Options:
- Flexion by iliopsoas, abduction by gluteus medius/minimus, external rotation by short external rotators
- Flexion by rectus femoris, abduction by tensor fasciae latae, external rotation by piriformis
- Flexion by sartorius, abduction by gluteus maximus, external rotation by obturator internus
- Extension by hamstrings, adduction by adductor longus, internal rotation by gluteus minimus
- Flexion by iliopsoas, adduction by adductor magnus, external rotation by quadratus femoris
Correct Answer: Flexion by iliopsoas, abduction by gluteus medius/minimus, external rotation by short external rotators
Explanation:
In a subtrochanteric fracture, the proximal fragment is subjected to distinct deforming muscle forces: the iliopsoas (inserting on the lesser trochanter) causes flexion; the gluteus medius and minimus (inserting on the greater trochanter) cause abduction; and the short external rotators (inserting in the trochanteric fossa/crest) cause external rotation. The distal fragment is typically adducted (by the adductor muscles) and shortened.
Question 8:
Which of the following describes the threshold value of 'delta pressure' typically considered an indication for emergency fasciotomy in a suspected acute compartment syndrome of the lower leg?
Options:
- Delta pressure < 40 mmHg
- Delta pressure < 30 mmHg
- Delta pressure < 20 mmHg
- Delta pressure < 45 mmHg
- Delta pressure < 10 mmHg
Correct Answer: Delta pressure < 30 mmHg
Explanation:
The diagnosis of acute compartment syndrome is primarily clinical, but in obtunded or polytrauma patients, compartment pressure monitoring is essential. While an absolute intracompartmental pressure > 30 mmHg is considered a warning sign, the delta pressure (diastolic blood pressure minus intracompartmental pressure) is a more accurate threshold. A delta pressure of < 30 mmHg indicates inadequate tissue perfusion and is a strong indication for emergency four-compartment fasciotomy.
Question 9:
A 28-year-old male presents with a posterior hip dislocation following a dashboard injury. Post-reduction CT scan reveals a Pipkin Type II fracture. What defines a Pipkin Type II fracture?
Options:
- Fracture of the femoral head caudad to the fovea capitis
- Fracture of the femoral head cephalad to the fovea capitis
- Femoral head fracture associated with a femoral neck fracture
- Femoral head fracture associated with an acetabular fracture
- Isolated fracture of the posterior wall of the acetabulum
Correct Answer: Fracture of the femoral head cephalad to the fovea capitis
Explanation:
The Pipkin classification describes fractures of the femoral head associated with posterior hip dislocations. Type I is a fracture caudad (inferior) to the fovea capitis (non-weight-bearing portion). Type II is a fracture cephalad (superior) to the fovea capitis (weight-bearing portion). Type III is any femoral head fracture (Type I or II) with an associated femoral neck fracture. Type IV is a femoral head fracture with an associated acetabular fracture.
Question 10:
A 40-year-old male falls from a height and sustains an acetabular fracture. Radiographs and CT demonstrate a transverse fracture line through the acetabulum and an oblique fracture extending down through the obturator ring, separating the anterior and posterior columns. The ischiopubic ramus and iliopubic ramus are fractured, but a portion of the articular surface remains attached to the intact ilium. What is the correct classification?
Options:
- Both-column fracture
- T-type fracture
- Transverse fracture
- Anterior column posterior hemi-transverse
- Posterior column with posterior wall
Correct Answer: T-type fracture
Explanation:
The Letournel classification divides acetabular fractures into 5 elementary and 5 associated types. A T-type fracture is an associated fracture pattern characterized by a transverse fracture component combined with a vertical split that extends into the obturator foramen, effectively separating the anterior and posterior columns inferiorly. Unlike a both-column fracture (where NO articular segment remains attached to the intact ilium, denoted by the 'spur sign'), in a T-type fracture, the superior articular surface (the roof) remains attached to the intact ilium.
Question 11:
A 55-year-old woman underwent volar locking plate fixation for a distal radius fracture 6 months ago. She now presents with an inability to actively flex the interphalangeal joint of her thumb. She reports a sudden pop without significant trauma. What is the most likely cause?
Options:
- Non-union of the distal radius
- Attritional rupture of the flexor pollicis longus (FPL) tendon
- Anterior interosseous nerve (AIN) palsy
- Extensor pollicis longus (EPL) rupture
- Trigger thumb
Correct Answer: Attritional rupture of the flexor pollicis longus (FPL) tendon
Explanation:
Attritional rupture of the flexor pollicis longus (FPL) tendon is a recognized complication of volar plating of the distal radius. It typically occurs due to prominent hardware (especially the distal edge of the plate) irritating the tendon as it crosses the watershed line. Patients present with loss of active IP joint flexion of the thumb. A sudden 'pop' is characteristic of the tendon rupturing.
Question 12:
A 24-year-old football player sustains a high-energy knee dislocation (Schenck KD-IV). The knee is grossly unstable, and on examination, the dorsalis pedis and posterior tibial pulses are absent. Ankle-brachial index (ABI) is 0.7. Following closed reduction of the knee, the pulses remain absent. What is the most appropriate next step in management?
Options:
- Observe and re-examine in 2 hours
- Emergent CT angiography
- Immediate surgical exploration of the popliteal artery
- Duplex ultrasonography
- Apply an external fixator and admit to ICU
Correct Answer: Immediate surgical exploration of the popliteal artery
Explanation:
In the setting of a knee dislocation with 'hard signs' of vascular injury (such as absent pulses that do not return after reduction, active hemorrhage, expanding hematoma, or distal ischemia), the most appropriate step is immediate surgical exploration of the popliteal artery in the operating room. Delaying surgical revascularization for imaging (like CT angio) in the presence of hard signs risks irreversible limb ischemia.
Question 13:
A 35-year-old male presents with an ipsilateral femur and tibia fracture (floating knee). Radiographs reveal a diaphyseal femur fracture and an intra-articular tibial plateau fracture. According to the Fraser classification, what type of floating knee injury is this?
Options:
- Type I
- Type IIA
- Type IIB
- Type IIC
- Type III
Correct Answer: Type IIB
Explanation:
The Fraser classification categorizes 'floating knee' injuries (ipsilateral femur and tibia fractures) based on articular involvement. Type I: both fractures are diaphyseal. Type II: involves the joint. Type IIA: diaphyseal tibia fracture + intra-articular distal femur fracture. Type IIB: diaphyseal femur fracture + intra-articular proximal tibia fracture. Type IIC: both fractures are intra-articular. This case is a Type IIB.
Question 14:
A 42-year-old male sustains a high-energy Reudi-Allgower Type III pilon fracture. The soft tissues are severely swollen with fracture blisters. What is the gold-standard initial management protocol for this injury?
Options:
- Immediate definitive open reduction and internal fixation (ORIF)
- Primary arthrodesis of the tibiotalar joint
- Spanning external fixation with delayed definitive ORIF
- Non-operative management in a long leg cast
- Immediate intramedullary nailing of the tibia
Correct Answer: Spanning external fixation with delayed definitive ORIF
Explanation:
High-energy Pilon fractures are associated with severe soft tissue compromise. Immediate open reduction and internal fixation (ORIF) carries an unacceptably high risk of wound breakdown, deep infection, and osteomyelitis. The current gold-standard protocol is a staged approach: immediate application of a spanning external fixator across the ankle joint to restore length and alignment, followed by a delay of 1-3 weeks for soft tissue swelling to resolve (positive 'wrinkle sign'), after which definitive ORIF is performed.
Question 15:
A 28-year-old snowboarder sustains a Hawkins Type III fracture of the talar neck. Which of the following best describes the fracture pattern and the associated risk of avascular necrosis (AVN) of the talar body?
Options:
- Undisplaced fracture, AVN risk < 10%
- Fracture with subtalar subluxation/dislocation, AVN risk 20-50%
- Fracture with subtalar and tibiotalar dislocation, AVN risk near 100%
- Fracture with subtalar, tibiotalar, and talonavicular dislocation, AVN risk 100%
- Fracture with isolated talonavicular dislocation, AVN risk 50%
Correct Answer: Fracture with subtalar and tibiotalar dislocation, AVN risk near 100%
Explanation:
The Hawkins classification for talar neck fractures is predictive of the risk of AVN. Type I: nondisplaced (AVN risk 0-15%). Type II: displaced with subtalar subluxation or dislocation (AVN risk 20-50%). Type III: displaced with both subtalar and tibiotalar (ankle) dislocation (AVN risk > 90% or near 100% historically). Type IV: Type III + talonavicular subluxation/dislocation. Therefore, Type III involves dislocation of both the subtalar and ankle joints.
Question 16:
A 45-year-old construction worker falls from a ladder and sustains a displaced intra-articular calcaneus fracture (Sanders Type III). A decision is made to proceed with open reduction and internal fixation (ORIF) via an extensile lateral approach. Which of the following structures is at greatest risk of injury during the elevation of the full-thickness soft tissue flap?
Options:
- Medial plantar nerve
- Sural nerve
- Superficial peroneal nerve
- Posterior tibial artery
- Deep peroneal nerve
Correct Answer: Sural nerve
Explanation:
The extensile lateral approach to the calcaneus involves creating a full-thickness fasciocutaneous flap containing the sural nerve, peroneal tendons, and the lesser saphenous vein. The sural nerve is at significant risk of injury (either transection, traction neuritis, or entrapment in scar) during the incision and elevation of this flap. The flap must be meticulously elevated in a subperiosteal plane from the lateral wall of the calcaneus.
Question 17:
A 50-year-old male sustains a severe valgus force to the knee, resulting in a split-depression fracture of the lateral tibial plateau. According to the Schatzker classification, what type of fracture is this?
Options:
- Type I
- Type II
- Type III
- Type IV
- Type V
Correct Answer: Type II
Explanation:
The Schatzker classification for tibial plateau fractures is: Type I: split fracture of the lateral plateau (typically younger patients). Type II: split-depression fracture of the lateral plateau (most common, older patients). Type III: pure central depression of the lateral plateau. Type IV: medial plateau fracture. Type V: bicondylar fracture. Type VI: metaphyseal-diaphyseal dissociation. A split-depression lateral plateau fracture is a Type II.
Question 18:
An 82-year-old female with a history of severe rheumatoid arthritis and osteoporosis sustains a comminuted, intra-articular distal humerus fracture (AO/OTA 13-C3). What is the most appropriate surgical treatment that allows for immediate post-operative mobilization and predictable functional outcomes?
Options:
- Open reduction and internal fixation with dual orthogonal locking plates
- Total elbow arthroplasty (TEA)
- Hemiarthroplasty of the elbow
- Closed reduction and percutaneous pinning
- Olecranon osteotomy with tension band wiring
Correct Answer: Total elbow arthroplasty (TEA)
Explanation:
In elderly patients with osteoporotic bone, severe comminution, and pre-existing joint disease (like rheumatoid arthritis), obtaining stable internal fixation to permit early range of motion is notoriously difficult. Total elbow arthroplasty (TEA) has emerged as the treatment of choice for non-reconstructible distal humerus fractures in low-demand elderly patients, providing reliable pain relief, immediate stability, and early mobilization.
Question 19:
A 25-year-old male presents with midfoot pain after missing a step and axially loading a plantarflexed foot. Weight-bearing radiographs reveal a 3 mm diastasis between the base of the first and second metatarsals, and a 'fleck sign' in the medial cuneiform-second metatarsal space. What does the 'fleck sign' represent?
Options:
- Avulsion of the anterior tibialis tendon insertion
- Avulsion of the Lisfranc ligament from the base of the second metatarsal
- Fracture of the os peroneum
- Avulsion of the plantar fascia from the calcaneus
- Avulsion of the bifurcate ligament
Correct Answer: Avulsion of the Lisfranc ligament from the base of the second metatarsal
Explanation:
The Lisfranc ligament is a strong interosseous ligament connecting the medial cuneiform to the base of the second metatarsal. It is critical for the stability of the tarsometatarsal joint complex. The 'fleck sign' is a small bony avulsion fragment seen in the space between the medial cuneiform and the base of the second metatarsal on an AP or internal oblique radiograph. It represents a bony avulsion of the Lisfranc ligament and is pathognomonic for a Lisfranc injury.
Question 20:
A 22-year-old active male sustains a closed, completely displaced midshaft clavicle fracture with 2.5 cm of shortening. There is no neurovascular deficit. Based on current orthopedic evidence, what is the primary advantage of open reduction and internal fixation (ORIF) over non-operative management for this specific injury pattern?
Options:
- Decreased risk of infection
- Lower rate of symptomatic non-union
- Elimination of the need for future hardware removal
- Reduced risk of pneumothorax
- Improved cosmetic appearance without a scar
Correct Answer: Lower rate of symptomatic non-union
Explanation:
While historically most midshaft clavicle fractures were treated non-operatively, recent randomized controlled trials (such as the Canadian Orthopaedic Trauma Society - COTS study) have shown that completely displaced midshaft clavicle fractures with > 2 cm of shortening have a high non-union rate (up to 15-20%) when treated non-operatively. ORIF with plate and screws significantly reduces the rate of symptomatic non-union and malunion, providing a faster return to function.
Question 21:
A 35-year-old male is brought to the ED after a high-speed motorcycle collision. He is hypotensive with a blood pressure of 80/40 mmHg and a heart rate of 125 bpm. Secondary survey reveals an unstable pelvis. A pelvic binder is to be applied. What is the correct anatomical landmark for optimal placement of the pelvic binder to effectively reduce pelvic volume?
Options:
- Greater trochanters
- Anterior superior iliac spines
- Iliac crests
- Pubic symphysis
- Umbilicus
Correct Answer: Greater trochanters
Explanation:
Pelvic binders are most effective at reducing pelvic volume and stabilizing the fracture when placed directly over the greater trochanters. Placing the binder too high (e.g., over the ASIS or iliac crests) is mechanically less effective and may paradoxically exacerbate the deformity.
Question 22:
A 40-year-old male presents with a posterior hip dislocation and an associated posterior wall acetabular fracture following a dashboard injury. After closed reduction of the hip, a CT scan reveals a posterior wall fragment constituting 45% of the articular surface with marginal impaction. What is the most appropriate definitive management?
Options:
- Non-weight-bearing for 6 weeks
- Skeletal traction for 6 weeks
- Open reduction and internal fixation through a Kocher-Langenbeck approach
- Open reduction and internal fixation through an ilioinguinal approach
- Total hip arthroplasty
Correct Answer: Open reduction and internal fixation through a Kocher-Langenbeck approach
Explanation:
Posterior wall fractures involving >20-40% of the articular surface, or those with marginal impaction or hip instability, require surgical fixation. The Kocher-Langenbeck approach provides excellent exposure to the posterior column and posterior wall, making it the standard approach for this injury.
Question 23:
A 25-year-old male polytrauma patient sustains a severe closed femoral shaft fracture, bilateral rib fractures, and a grade III liver laceration. On arrival, his pH is 7.15, lactate is 6.5, core temperature is 34°C, and he has required 6 units of PRBCs. According to Damage Control Orthopedics (DCO) principles, what is the best management of his femur fracture at this time?
Options:
- Reamed antegrade intramedullary nailing
- Unreamed retrograde intramedullary nailing
- Temporary spanning external fixation
- Open reduction and internal fixation with a compression plate
- Skeletal traction
Correct Answer: Temporary spanning external fixation
Explanation:
This patient is in extremis and exhibiting the 'lethal triad' of trauma (acidosis, hypothermia, coagulopathy). According to DCO principles, Early Total Care (ETC) with prolonged procedures like IM nailing is contraindicated as it acts as a 'second hit'. Rapid temporary stabilization with external fixation limits further physiological insult and allows for ongoing resuscitation.
Question 24:
A 32-year-old female sustains a distal femur fracture following a fall. Radiographs and CT show a coronal shear fracture of the lateral femoral condyle. What is the eponym for this fracture pattern, and what is the preferred method of fixation?
Options:
- Segond fracture; conservative management
- Hoffa fracture; anterior-to-posterior (AP) or PA lag screws
- Barton fracture; volar plating
- Stieda fracture; excision
- Tillaux fracture; percutaneous pinning
Correct Answer: Hoffa fracture; anterior-to-posterior (AP) or PA lag screws
Explanation:
A coronal shear fracture of the femoral condyle is known as a Hoffa fracture. It most commonly affects the lateral condyle. Definitive fixation is typically achieved using lag screws placed from anterior to posterior (or PA), often countersunk beneath the cartilage to prevent articular damage.
Question 25:
A 55-year-old male sustains a high-energy varus impact to his knee. Radiographs reveal a medial tibial plateau fracture with significant depression and widening. What is the Schatzker classification for this injury, and what is the associated soft tissue injury most commonly seen?
Options:
- Schatzker I; medial meniscus tear
- Schatzker II; lateral collateral ligament tear
- Schatzker IV; lateral collateral ligament / posterolateral corner injury
- Schatzker V; patellar tendon rupture
- Schatzker VI; isolated medial meniscus tear
Correct Answer: Schatzker IV; lateral collateral ligament / posterolateral corner injury
Explanation:
A medial tibial plateau fracture represents a Schatzker IV. This is typically a high-energy pattern resulting from severe varus stress, often leading to distraction or avulsion injuries to the lateral-sided structures, including the lateral collateral ligament (LCL) and the posterolateral corner (PLC).
Question 26:
A 28-year-old male presents with a closed, severely displaced tibial shaft fracture. He complains of excruciating pain out of proportion to the injury. On examination, there is tense swelling and pain with passive stretch of the hallux, but he has palpable dorsalis pedis and posterior tibial pulses. His diastolic blood pressure is 80 mmHg, and his anterior compartment pressure is measured at 60 mmHg. What is the most appropriate next step in management?
Options:
- Elevate the leg above the level of the heart
- Application of a tight compression dressing
- Immediate four-compartment fasciotomy
- Observation and repeat pressure measurements in 4 hours
- Intravenous dexamethasone
Correct Answer: Immediate four-compartment fasciotomy
Explanation:
The clinical presentation (pain out of proportion, pain with passive stretch) and compartment pressures confirm acute compartment syndrome. A delta pressure (diastolic BP - compartment pressure) of < 30 mmHg (here it is 80 - 60 = 20 mmHg) is an absolute indication for immediate surgical decompression via a four-compartment fasciotomy. Palpable pulses are typically maintained until very late in the disease process.
Question 27:
A 45-year-old male sustains a high-energy tibial pilon fracture. The initial presentation includes severe soft tissue swelling, massive fracture blisters, and skin tenting. What is the most widely accepted initial management strategy for this patient?
Options:
- Immediate open reduction and internal fixation with dual plating
- Immediate unreamed intramedullary nailing
- Spanning external fixation across the ankle joint with delayed definitive fixation
- Application of a short leg cast and immediate weight-bearing
- Primary arthrodesis of the tibiotalar joint
Correct Answer: Spanning external fixation across the ankle joint with delayed definitive fixation
Explanation:
High-energy pilon fractures with severely compromised soft tissues (swelling, blisters) are at extremely high risk for wound necrosis and deep infection. They are best managed with a staged protocol: initial spanning external fixation to restore length and alignment, followed by definitive ORIF once the soft tissues have recovered (typically 10-21 days later), evidenced by the return of skin wrinkles.
Question 28:
A 30-year-old pilot sustains a hyperdorsiflexion injury to his foot resulting in a displaced talar neck fracture. He undergoes ORIF. At 8 weeks postoperatively, an AP radiograph of the ankle shows a subchondral radiolucent band in the talar dome. What does this radiographic finding indicate?
Options:
- Immediate need for subtalar fusion
- Onset of avascular necrosis (AVN) of the talar body
- Septic arthritis of the ankle joint
- Revascularization and intact blood supply to the talar body
- Nonunion of the talar neck
Correct Answer: Revascularization and intact blood supply to the talar body
Explanation:
This radiographic finding is the 'Hawkins sign', which is a subchondral radiolucent band seen in the talar dome 6 to 8 weeks following a talar neck fracture. It indicates subchondral osteopenia secondary to bone resorption, confirming an intact vascular supply to the talar body and indicating that avascular necrosis (AVN) is unlikely.
Question 29:
A 50-year-old male falls from a ladder and sustains an intra-articular calcaneus fracture. Which of the following is considered the primary indication for operative management (ORIF) of this fracture?
Options:
- Non-displaced extra-articular fracture
- Age over 65 with severe peripheral vascular disease
- Displaced intra-articular fracture with loss of height, increased width, and decreased Böhler's angle in a healthy patient
- Fracture in a patient who is a heavy, active smoker (2 packs per day)
- Sanders type I fracture
Correct Answer: Displaced intra-articular fracture with loss of height, increased width, and decreased Böhler's angle in a healthy patient
Explanation:
Operative treatment for calcaneus fractures is indicated for displaced intra-articular fractures (Sanders Type II or III) to restore heel height, heel width, Böhler's angle, and congruity of the posterior facet. Severe peripheral vascular disease and heavy smoking are major contraindications due to the exceptionally high risk of wound slough and deep infection.
Question 30:
A 22-year-old football player presents with severe midfoot pain after his foot was axially loaded while plantarflexed. Radiographs show widening of the space between the base of the 1st and 2nd metatarsals and a small avulsion fracture at the medial base of the 2nd metatarsal. What is the name of this pathognomonic fracture, and what is the primary diagnosis?
Options:
- Jones fracture; fifth metatarsal base fracture
- Fleck sign; Lisfranc injury
- Nutcracker fracture; cuboid crush injury
- Pseudo-Jones fracture; plantar fascia avulsion
- Shepherd's fracture; posterior talar process injury
Correct Answer: Fleck sign; Lisfranc injury
Explanation:
The 'fleck sign' refers to a small avulsion fracture off the base of the 2nd metatarsal or medial cuneiform and is pathognomonic for a Lisfranc injury. The Lisfranc ligament, which connects the medial cuneiform to the base of the 2nd metatarsal, is critical for midfoot stability.
Question 31:
A 35-year-old farmer sustains an open tibial shaft fracture from agricultural machinery. The wound is 12 cm long with extensive soft tissue stripping, but adequate soft tissue remains to cover the fractured bone without the need for a free flap. The wound is heavily contaminated with soil. What is the Gustilo-Anderson classification, and what is the recommended empiric antibiotic regimen?
Options:
- Type II; First-generation cephalosporin alone
- Type IIIA; First-generation cephalosporin and an aminoglycoside, plus penicillin for anaerobic coverage
- Type IIIB; First-generation cephalosporin and an aminoglycoside
- Type IIIC; Penicillin alone
- Type IIIA; Clindamycin alone
Correct Answer: Type IIIA; First-generation cephalosporin and an aminoglycoside, plus penicillin for anaerobic coverage
Explanation:
An open fracture >10 cm with extensive soft tissue damage but adequate coverage is classified as Gustilo-Anderson Type IIIA. Farm injuries with soil contamination carry a high risk of Clostridium infection. Standard guidelines recommend a first-generation cephalosporin (gram-positives), an aminoglycoside (gram-negatives), and penicillin (anaerobes like Clostridium).
Question 32:
A 25-year-old male sustains a low-velocity gunshot wound to the lower extremity. The entry wound is on the medial aspect of the knee and the exit is lateral. Radiographs confirm a non-displaced transverse fracture of the distal femur. Fluid aspirate from the knee joint demonstrates a hemarthrosis with fat globules. What is the most appropriate initial management of the joint?
Options:
- Simple wound care and oral antibiotics
- Immediate intramedullary nailing of the femur
- Arthroscopic or open intra-articular debridement and irrigation of the knee joint
- Spanning external fixation and delayed primary closure
- Application of a cylinder cast
Correct Answer: Arthroscopic or open intra-articular debridement and irrigation of the knee joint
Explanation:
An intra-articular gunshot wound (indicated by the trajectory, fracture pattern, and hemarthrosis with fat globules) is an absolute indication for urgent arthroscopic or open intra-articular debridement and copious irrigation. This removes debris, bullet fragments, and osteochondral loose bodies, significantly reducing the risk of septic arthritis.
Question 33:
An 80-year-old female presents with a periprosthetic femur fracture around her cemented total hip arthroplasty. Radiographs reveal a fracture extending around the tip of the stem. The stem is loose, but there is good remaining proximal and distal bone stock. What is the Vancouver classification, and what is the standard treatment?
Options:
- Vancouver B1; ORIF with a locked plate and cables
- Vancouver B2; Revision arthroplasty with a long uncemented diaphyseal-engaging stem
- Vancouver B3; ORIF with strut allografts
- Vancouver C; Revision of the acetabular component
- Vancouver A; Non-operative management
Correct Answer: Vancouver B2; Revision arthroplasty with a long uncemented diaphyseal-engaging stem
Explanation:
The Vancouver classification for periprosthetic femur fractures defines Type B as fractures around the stem or just below it. It is subclassified based on implant stability and bone stock: B1 (well-fixed stem), B2 (loose stem, good bone stock), and B3 (loose stem, poor bone stock). A loose stem with adequate bone stock (B2) is treated with revision arthroplasty, typically using a long, diaphyseal-engaging stem to bypass the fracture.
Question 34:
A 40-year-old male sustains a severe crush injury to his lower leg. The Mangled Extremity Severity Score (MESS) is utilized to help determine the likelihood of amputation versus limb salvage. Which of the following is NOT a component of the MESS?
Options:
- Skeletal and soft tissue injury (energy of trauma)
- Limb ischemia
- Shock (hypotension)
- Patient age
- Associated head injury (GCS)
Correct Answer: Associated head injury (GCS)
Explanation:
The Mangled Extremity Severity Score (MESS) is calculated using four variables: 1) Skeletal and soft-tissue injury (energy), 2) Limb ischemia, 3) Shock, and 4) Patient age. While a severe head injury influences overall patient survival, it is not a component of the MESS itself.
Question 35:
A 45-year-old smoker is 9 months out from an open midshaft tibial fracture treated with a reamed intramedullary nail. He complains of pain with weight-bearing. Radiographs show a persistent fracture line with tapered, pencil-like bone ends and no bridging callus. What type of nonunion is this, and what is the primary underlying etiology?
Options:
- Hypertrophic nonunion; inadequate stability
- Oligotrophic nonunion; infection
- Atrophic nonunion; inadequate biology/blood supply
- Infected nonunion; retained hardware
- Pseudarthrosis; mechanical failure
Correct Answer: Atrophic nonunion; inadequate biology/blood supply
Explanation:
Tapered, sclerotic bone ends with an absence of callus formation characterize an atrophic nonunion. This indicates a biological failure of healing (inadequate vascularity, poor osteogenic response), which is strongly exacerbated by smoking. Treatment requires improving biology, typically with autologous bone grafting.
Question 36:
A 22-year-old cyclist falls onto his shoulder and sustains a midshaft clavicle fracture. Which of the following physical exam or radiographic findings is considered an absolute indication for acute operative fixation?
Options:
- Complete displacement with 5 mm of shortening
- Impending open fracture with severe skin tenting and blanching
- Associated ipsilateral non-displaced radial head fracture
- Patient preference to return to sports 1 week earlier
- Comminution with an intact butterfly fragment
Correct Answer: Impending open fracture with severe skin tenting and blanching
Explanation:
Absolute indications for operative fixation of a clavicle fracture include open fractures, impending open fractures (severe skin tenting with blanching/ischemia of the overlying skin), and neurovascular compromise. Displacement with shortening > 2 cm is a strong relative indication, but 5 mm is not.
Question 37:
A 78-year-old right-hand-dominant female with osteoporosis falls and sustains a complex 4-part proximal humerus fracture. There is a valgus impacted head, significant tuberosity displacement, and a compromised medial calcar hinge. What is the most reliable surgical option for pain relief and functional restoration in this patient?
Options:
- Closed reduction and percutaneous pinning
- Open reduction and internal fixation with a locked plate
- Hemiarthroplasty
- Reverse total shoulder arthroplasty (RTSA)
- Non-operative management with a sling for 6 weeks
Correct Answer: Reverse total shoulder arthroplasty (RTSA)
Explanation:
In elderly patients with poor bone stock (osteoporosis) and complex 4-part proximal humerus fractures, ORIF has a high risk of hardware cutout and failure. Hemiarthroplasty relies heavily on tuberosity healing, which is unpredictable. Reverse total shoulder arthroplasty (RTSA) provides more reliable outcomes for pain relief and functional restoration because it is less dependent on tuberosity healing and native rotator cuff function.
Question 38:
A 35-year-old male sustains a spiral fracture of the distal third of the humeral shaft while arm wrestling. He presents to the ED with an inability to extend his wrist and fingers. What is the proper eponym for this fracture pattern, and what structure is typically injured?
Options:
- Monteggia fracture; posterior interosseous nerve
- Galeazzi fracture; median nerve
- Holstein-Lewis fracture; radial nerve
- Essex-Lopresti injury; ulnar nerve
- Nightstick fracture; superficial radial nerve
Correct Answer: Holstein-Lewis fracture; radial nerve
Explanation:
A spiral fracture of the distal one-third of the humeral shaft is known as a Holstein-Lewis fracture. It is classically associated with an increased risk of radial nerve palsy as the nerve becomes tethered or lacerated as it passes through the lateral intermuscular septum.
Question 39:
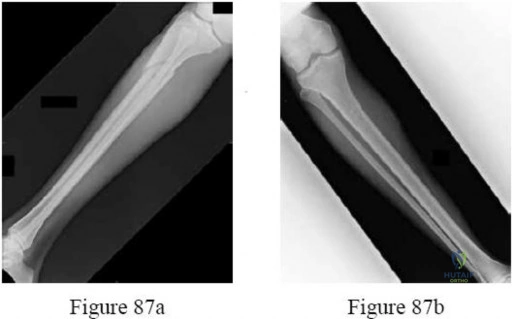
A 28-year-old motorcyclist presents after a high-speed collision. Radiographs demonstrate an ipsilateral femoral shaft fracture and a tibial shaft fracture. What is the standard term for this injury combination, and what systemic complication is most significantly increased in this specific patient population?
Options:
- Terrible triad; compartment syndrome
- Floating knee; fat embolism syndrome
- Floating hip; deep vein thrombosis
- Dashboard knee; popliteal artery rupture
- Mangled extremity; acute kidney injury
Correct Answer: Floating knee; fat embolism syndrome
Explanation:
An ipsilateral fracture of both the femur and tibia is termed a 'floating knee'. This high-energy injury pattern reflects massive trauma and is associated with a significantly higher risk of systemic complications, particularly fat embolism syndrome and acute respiratory distress syndrome (ARDS), compared to isolated long bone fractures.
Question 40:
A 24-year-old trauma patient has sustained bilateral femur fractures. Upon arrival to the trauma bay, his blood pressure is 110/80 mmHg, heart rate is 115 bpm, respiratory rate is 22 breaths/min, and he is slightly anxious. Urine output is measured at 25 mL/hr. Based on the ATLS classification of hemorrhagic shock, which class best describes this patient's clinical presentation?
Options:
- Class I
- Class II
- Class III
- Class IV
- Class V
Correct Answer: Class II
Explanation:
Class II hemorrhagic shock (15-30% blood volume loss) is characterized by tachycardia (HR > 100), a normal systolic blood pressure (though pulse pressure may be narrowed), mild tachypnea (RR 20-30), and mild anxiety. Class III would present with overt hypotension, and Class I would present with a heart rate < 100.
Question 41:
A 25-year-old motorcyclist is involved in a high-speed collision and sustains a 'floating knee' injury. Radiographs demonstrate a diaphyseal fracture of the femoral shaft and an intra-articular fracture of the proximal tibia. According to the Fraser classification, what type of injury is this?
Options:
- Type I
- Type IIc
- Type IIa
- Type IIb
- Type III
Correct Answer: Type IIa
Explanation:
Fraser classification describes 'floating knee' injuries. Type I is a true floating knee with diaphyseal fractures of both the femur and tibia. Type IIa is a diaphyseal femur fracture with an intra-articular tibia fracture. Type IIb is an intra-articular femur fracture with a diaphyseal tibia fracture. Type IIc involves intra-articular fractures of both the femur and the tibia.
Question 42:
A 30-year-old male presents after a motorcycle crash with severe shoulder swelling and pulselessness in the ipsilateral upper extremity. Radiographs show a widened scapulothoracic interval and an intact clavicle. Which of the following is the most significant predictor of poor functional outcome in this patient?
Options:
- Associated subclavian artery disruption
- Complete brachial plexus avulsion
- Severity of associated rib fractures
- Degree of lateral displacement of the scapula
- Development of compartment syndrome in the forearm
Correct Answer: Complete brachial plexus avulsion
Explanation:
Scapulothoracic dissociation represents a traumatic forequarter amputation with intact skin, characterized by lateral displacement of the scapula and severe neurovascular injury. While vascular injuries are limb-threatening, the most significant predictor of long-term functional recovery is neurological status. Complete brachial plexus avulsion carries a grim prognosis, often resulting in a flail, insensate limb that may necessitate amputation despite successful vascular reconstruction.
Question 43:
A 45-year-old obese female sustains a severe closed crush injury to her lateral thigh. Three weeks later, she presents with a fluctuant, painless mass over the greater trochanter. Aspiration yields serosanguinous fluid. What is the most definitive surgical management for this chronic lesion if conservative measures and simple drainage fail?
Options:
- Repeated percutaneous aspirations every 3 days
- Incision and drainage with placement of a negative pressure wound therapy device
- Open excision of the pseudocapsule and dead space obliteration
- Application of a tight compression dressing for 6 weeks
- Local injection of corticosteroids
Correct Answer: Open excision of the pseudocapsule and dead space obliteration
Explanation:
The clinical presentation describes a chronic Morel-Lavallée lesion, a closed degloving injury where subcutaneous tissue separates from the underlying fascia, creating a potential space that fills with hemolymph. Over time, a pseudocapsule forms, preventing adherence of tissue layers. When conservative measures fail, definitive treatment requires open excision of the pseudocapsule (capsulectomy) and closure of the dead space, often via quilting sutures or surgical drains.
Question 44:
In the management of open extremity fractures, large-scale studies (such as LEAP) have identified several factors that influence the rate of deep infection. Which of the following has the most significant evidence-based impact on reducing infection risk?
Options:
- The use of high-pressure pulsatile lavage during initial debridement
- Performing surgical debridement within exactly 6 hours of injury
- The administration of systemic antibiotics within 1 hour of injury
- The addition of local antibiotic beads at the time of initial debridement
- Routine application of negative pressure wound therapy (NPWT)
Correct Answer: The administration of systemic antibiotics within 1 hour of injury
Explanation:
The most critical intervention in reducing the infection rate of open fractures is the early administration of systemic antibiotics, ideally within 1 hour of injury. Delaying antibiotic administration significantly increases infection risk. The rigid '6-hour rule' for surgical debridement has been challenged; evidence shows outcomes do not significantly worsen if debridement is performed within 24 hours, provided prompt antibiotics were given.
Question 45:
According to the classic principles described by Marko Godina for the management of complex open tibial fractures requiring free tissue transfer, what is the optimal timeframe for soft tissue coverage to minimize the risk of flap failure and deep infection?
Options:
- Within 12 hours
- Within 24 hours
- Within 48 hours
- Within 72 hours
- After 5 days
Correct Answer: Within 72 hours
Explanation:
Marko Godina's classic 1986 study demonstrated that early free flap coverage of complex extremity injuries, performed within 72 hours, significantly decreased flap failure rates, infection rates, and time to bone union compared to delayed coverage. This timeframe takes advantage of a less colonized wound bed and favorable local anatomy before established fibrosis occurs.
Question 46:
A 28-year-old polytrauma patient (ISS 35) with a bilateral femoral shaft fracture is initially treated with Damage Control Orthopedics (DCO) via external fixation. He is currently in the ICU. Which laboratory parameter is the most reliable indicator that he is physiologically optimized for conversion to definitive intramedullary nailing?
Options:
- Serum lactate < 2.5 mmol/L and improving base deficit
- Hemoglobin > 10 g/dL
- White blood cell count < 10,000/mm³
- Platelet count > 150,000/mm³
- C-reactive protein < 5 mg/L
Correct Answer: Serum lactate < 2.5 mmol/L and improving base deficit
Explanation:
In DCO, timing for conversion to Early Total Care (ETC) or definitive fixation depends on physiologic optimization. The clearance of serum lactate (< 2.5 mmol/L) and correction of base deficit are the most reliable indicators of adequate tissue perfusion and successful resuscitation. Operating during uncorrected hypoperfusion increases the risk of a 'second hit' phenomenon, such as ARDS or MODS.
Question 47:
A 22-year-old male sustains a low-velocity civilian gunshot wound to the thigh, resulting in a closed, comminuted midshaft femur fracture. He has normal distal pulses and intact neurological function. The entry and exit wounds are clean and measure 5 mm. What is the standard of care?
Options:
- Immediate formal excision of the bullet tract and external fixation
- Intravenous antibiotics for 14 days followed by delayed intramedullary nailing
- Local wound care, short-course antibiotics, and early antegrade intramedullary nailing
- Skeletal traction for 6 weeks
- Immediate exploration of the femoral artery and vein, regardless of pulse status
Correct Answer: Local wound care, short-course antibiotics, and early antegrade intramedullary nailing
Explanation:
Low-velocity gunshot wounds resulting in femur fractures without neurovascular compromise or massive soft tissue destruction are treated similarly to closed fractures. Standard care includes local wound care, tetanus prophylaxis, a short course of IV antibiotics, and definitive internal fixation (antegrade intramedullary nailing). Formal debridement of the bullet tract is unnecessary unless there is gross contamination or massive tissue necrosis.
Question 48:
A 34-year-old male with a bilateral femoral shaft fracture begins to exhibit confusion, tachypnea, and an axillary petechial rash 48 hours after injury. According to Gurd and Wilson criteria, which combination of signs represents the major criteria triad for diagnosing Fat Embolism Syndrome (FES)?
Options:
- Respiratory insufficiency, neurologic involvement, and petechial rash
- Tachycardia, fever, and jaundice
- Hypotension, oliguria, and coagulopathy
- Pleuritic chest pain, hemoptysis, and deep vein thrombosis
- Retinal hemorrhages, lipiduria, and anemia
Correct Answer: Respiratory insufficiency, neurologic involvement, and petechial rash
Explanation:
The classic triad of Fat Embolism Syndrome (FES), typically presenting 24 to 72 hours after major long bone trauma, includes respiratory insufficiency (hypoxemia), neurologic involvement (altered mental status), and a petechial rash (typically on the chest, axilla, and conjunctiva). These three constitute the major criteria for clinical diagnosis. The others listed are minor criteria.
Question 49:
A 68-year-old female with an 8-year history of alendronate therapy complains of dull right thigh pain. Radiographs reveal lateral cortical thickening and a transverse radiolucent line in the subtrochanteric region of the right femur, but no complete fracture. What is the most appropriate management?
Options:
- Discharge with NSAIDs and physical therapy
- Immediate total hip arthroplasty
- Continue alendronate and apply a long leg cast
- Discontinue alendronate, and perform prophylactic cephalomedullary nailing
- Continue alendronate and recommend non-weight bearing with crutches
Correct Answer: Discontinue alendronate, and perform prophylactic cephalomedullary nailing
Explanation:
This patient presents with an impending atypical femur fracture (AFF) associated with long-term bisphosphonate use. Radiographic hallmarks include lateral cortical 'beaking' and a transverse radiolucent line. Because symptomatic lesions have a high rate of progression to complete fracture and poor healing potential, the standard of care is discontinuation of the bisphosphonate and prophylactic surgical fixation, typically with a cephalomedullary nail.
Question 50:
A 25-year-old male sustains a severe crush injury to his lower leg. He complains of pain out of proportion. His blood pressure is 110/70 mmHg. Intracompartmental pressure monitoring of the anterior compartment yields a reading of 45 mmHg. What is the delta pressure, and is fasciotomy indicated?
Options:
- Delta pressure is 25 mmHg; fasciotomy is indicated
- Delta pressure is 65 mmHg; fasciotomy is not indicated
- Delta pressure is 25 mmHg; fasciotomy is not indicated
- Delta pressure is 65 mmHg; fasciotomy is indicated
- Delta pressure is 45 mmHg; fasciotomy is indicated
Correct Answer: Delta pressure is 25 mmHg; fasciotomy is indicated
Explanation:
Delta pressure (Δp) is calculated as Diastolic Blood Pressure minus Intracompartmental Pressure. Here, 70 mmHg - 45 mmHg = 25 mmHg. A delta pressure of 30 mmHg or less is widely accepted as an absolute indication for emergency fasciotomy, as capillary perfusion is critically compromised.
Question 51:
A 40-year-old male presents with persistent pain 8 months after a midshaft tibial fracture treated in a cast. Radiographs show a prominent 'elephant foot' callus formation but a persistent radiolucent line across the fracture gap. The site is mobile on exam. What is the primary underlying cause, and the treatment of choice?
Options:
- Poor biological potential; requires autologous bone grafting
- Deep infection; requires debridement and systemic antibiotics
- Avascular necrosis; requires resection and bone transport
- Vitamin D deficiency; requires supplementation and prolonged casting
- Excessive mechanical instability; requires rigid internal fixation
Correct Answer: Excessive mechanical instability; requires rigid internal fixation
Explanation:
An 'elephant foot' callus is characteristic of a hypertrophic nonunion. The robust callus indicates excellent biological healing potential (adequate vascularity), but healing arrests because the mechanical environment is too unstable for the callus to bridge the gap. The treatment of choice is optimizing mechanical stability through rigid internal fixation (e.g., exchange nailing or plating); bone grafting is generally unnecessary.
Question 52:
In a patient rescued from a collapsed building after 12 hours of entrapment, crush syndrome is highly suspected. To prevent the most common fatal complication of this syndrome, what is the initial medical management priority?
Options:
- Administration of loop diuretics to prevent pulmonary edema
- Immediate fasciotomy of all involved limbs before fluid resuscitation
- Aggressive intravenous fluid hydration to maintain high urine output
- Intravenous administration of calcium channel blockers
- Prophylactic hemodialysis
Correct Answer: Aggressive intravenous fluid hydration to maintain high urine output
Explanation:
The most critical complication of crush syndrome is acute kidney injury (AKI) secondary to massive rhabdomyolysis and myoglobinuria. Myoglobin precipitates in the renal tubules, especially in hypovolemic, acidic states. The primary initial treatment is aggressive intravenous fluid resuscitation (normal saline) to correct hypovolemia, maintain high urine output, and flush myoglobin through the kidneys. Urine alkalinization is also adjunctive.
Question 53:
The Reamer-Irrigator-Aspirator (RIA) system is frequently used to harvest large volumes of autologous bone graft from the femoral intramedullary canal. Which of the following is the most common serious complication specific to this technique?
Options:
- High-pressure fat embolism
- Iatrogenic cortical perforation or fracture
- Deep vein thrombosis
- Osteomyelitis of the donor femur
- Complete avascular necrosis of the femoral head
Correct Answer: Iatrogenic cortical perforation or fracture
Explanation:
While the RIA system provides excellent autogenous graft volume and lowers intramedullary pressure during use compared to standard reaming, its most common serious complication is eccentric reaming. This can lead to severe iatrogenic cortical thinning, perforation, or frank postoperative fracture of the donor femur. Careful fluoroscopic monitoring is mandatory.
Question 54:
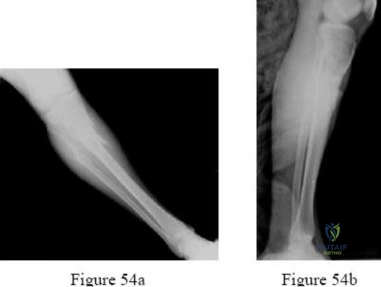
A 35-year-old polytrauma patient arrives in hemorrhagic shock with an open pelvic book fracture. The massive transfusion protocol (MTP) is activated. Current trauma resuscitation guidelines recommend administering PRBCs, FFP, and Platelets in what ratio to best mimic whole blood?
Options:
- 1:1:1
- 3:1:1
- 4:2:1
- 2:1:1
- 1:2:2
Correct Answer: 1:1:1
Explanation:
Based on landmark studies like the PROPPR trial, the standard of care for damage control resuscitation in severely bleeding trauma patients is a balanced ratio of 1:1:1 (PRBCs : FFP : Platelets). This proactively addresses trauma-induced coagulopathy by replacing clotting factors and platelets concurrently with oxygen-carrying red blood cells.
Question 55:
A 28-year-old male sustains a transverse subtrochanteric femur fracture. Due to the specific muscular attachments, what is the classic predictable deformity of the proximal fracture fragment?
Options:
- Extension, adduction, and internal rotation
- Flexion, adduction, and internal rotation
- Flexion, abduction, and external rotation
- Extension, abduction, and internal rotation
- Flexion, adduction, and external rotation
Correct Answer: Flexion, abduction, and external rotation
Explanation:
The proximal fragment in a subtrochanteric fracture is deformed by powerful muscle forces: the iliopsoas (lesser trochanter) causes flexion and external rotation, while the gluteus medius and minimus (greater trochanter) cause abduction. The short external rotators further contribute to external rotation. Therefore, the classic deformity is flexion, abduction, and external rotation.
Question 56:
A patient sustains an open pelvic ring injury in a high-speed collision. In the acute setting (within the first 24 hours), what is the most common cause of mortality in patients with this severe injury pattern?
Options:
- Severe sepsis
- Acute respiratory distress syndrome (ARDS)
- Exsanguinating hemorrhage
- Pulmonary embolism
- Fat embolism syndrome
Correct Answer: Exsanguinating hemorrhage
Explanation:
Open pelvic fractures are devastating injuries. In the acute phase (< 24 hours), the most common cause of mortality is exsanguinating hemorrhage arising from the highly vascular presacral venous plexus, major iliac vessels, and cancellous bone surfaces. If the patient survives the initial hemorrhagic shock, late mortality is most frequently due to sepsis and multi-organ failure.
Question 57:
The concept of 'Early Appropriate Care' (EAC) advocates for definitive fixation of major long bone fractures early in polytrauma patients if specific physiologic parameters are met. Which of the following laboratory values indicates a patient is sufficiently resuscitated to proceed with EAC?
Options:
- pH > 7.15
- Lactate < 4.0 mmol/L
- Base excess < -8.0 mmol/L
- Hemoglobin > 8.0 g/dL
- Fibrinogen > 100 mg/dL
Correct Answer: Lactate < 4.0 mmol/L
Explanation:
Early Appropriate Care (EAC) guidelines indicate that it is safe to proceed with definitive fracture fixation (e.g., within 36 hours) if the patient's physiology is optimized. Validated laboratory thresholds include a serum lactate < 4.0 mmol/L, pH >= 7.25, and base excess >= -5.5 mmol/L. These values confirm adequate restoration of tissue perfusion, reducing the risk of fatal systemic inflammatory responses to the surgery.
Question 58:
Emergency medical services bring in a hypotensive patient with a suspected 'open book' pelvic fracture. A pelvic binder was applied in the field. To effectively reduce pelvic volume and mechanically control hemorrhage, the binder should be centered precisely over which anatomical landmark?
Options:
- The iliac crests
- The anterior superior iliac spines (ASIS)
- The umbilicus
- The greater trochanters
- The pubic symphysis
Correct Answer: The greater trochanters
Explanation:
To optimally close an open-book pelvic ring injury and reduce intrapelvic volume (thereby creating a tamponade effect), the compressive force must be applied directly across the greater trochanters. Placing the binder too high (over the iliac crests or ASIS) compresses the false pelvis, failing to stabilize the true pelvic ring and potentially paradoxically opening the symphysis further.
Question 59:
An 80-year-old male is admitted after a ground-level fall, resulting in three unilateral rib fractures. He is neurologically intact and stable. Which of the following complications is he at the highest risk of developing, representing a major predictor of mortality in geriatric trauma?
Options:
- Aortic dissection
- Flail chest
- Pneumonia
- Tension pneumothorax
- Myocardial contusion
Correct Answer: Pneumonia
Explanation:
Rib fractures in the elderly are highly morbid due to decreased physiologic reserve. Pain leads to splinting, hypoventilation, and an inability to clear secretions, making the development of pneumonia the most significant risk and a major cause of mortality. Aggressive multimodal pain control (often epidural) and pulmonary hygiene are essential.
Question 60:
A 45-year-old male is involved in a motor vehicle collision and sustains a traumatic spondylolisthesis of the axis (Hangman's fracture). What is the most common mechanism of injury for this fracture pattern in modern civilian trauma?
Options:
- Axial loading and hyperflexion
- Severe lateral bending
- Hyperextension and axial loading
- Extreme rotation and flexion
- Distraction and hyperflexion
Correct Answer: Hyperextension and axial loading
Explanation:
A Hangman's fracture involves bilateral fractures of the C2 pars interarticularis. While historically caused by sudden severe distraction and hyperextension (judicial hanging), the most common mechanism in modern civilian trauma (e.g., an unrestrained occupant striking the dashboard with their face) involves violent hyperextension combined with axial loading.
Question 61:
Which of the following is considered an absolute indication for operative fixation of a scapula fracture?
Options:
- Glenopolar angle of 35 degrees
- Medialization of the lateral border of 10 mm
- Intra-articular step-off greater than 4 mm at the anterior glenoid rim
- Scapular body fracture with 10 mm displacement
- Angulation of the scapular body of 20 degrees
Correct Answer: Intra-articular step-off greater than 4 mm at the anterior glenoid rim
Explanation:
Indications for operative fixation of a scapula fracture include intra-articular glenoid displacement > 4 mm, glenopolar angle < 22 degrees, medialization of the lateral border > 20 mm, and severe double disruptions of the superior suspensory shoulder complex (SSSC). A glenopolar angle of 35 degrees is within normal limits (30-45 degrees).
Question 62:
A 25-year-old male develops acute compartment syndrome of the leg following a tibial shaft fracture. The surgeon elects to perform a dual-incision fasciotomy. During the medial approach, which specific surgical step is critical to adequately release the deep posterior compartment?
Options:
- Incising the fascia over the superficial posterior compartment only
- Detaching the soleus origin from the posteromedial border of the tibia
- Releasing the intermuscular septum between the anterior and lateral compartments
- Transecting the interosseous membrane from anterior to posterior
- Decompressing the tarsal tunnel at the ankle
Correct Answer: Detaching the soleus origin from the posteromedial border of the tibia
Explanation:
During the medial approach of a two-incision fasciotomy for the leg, the superficial posterior compartment is released first. The deep posterior compartment is then accessed by retracting the superficial compartment posteriorly and detaching the soleus fascial bridge from the posteromedial border of the tibia. Failure to release this fascial attachment is the most common reason for an incomplete decompression of the deep posterior compartment.
Question 63:
A 30-year-old male falls from a ladder, sustaining a Hawkins Type III talar neck fracture. Which of the following describes the most likely mechanism of injury and the approximate risk of developing avascular necrosis (AVN) of the talar body?
Options:
- Hyperplantarflexion; 20%
- Hyperdorsiflexion; greater than 80%
- Axial loading with inversion; 50%
- Direct crush injury; 10%
- Pronation-abduction; 100%
Correct Answer: Hyperdorsiflexion; greater than 80%
Explanation:
The classic mechanism for a talar neck fracture is hyperdorsiflexion, where the talar neck impacts against the anterior distal tibia (e.g., 'aviator/'s astragalus'). A Hawkins Type III fracture involves the talar neck with dislocation of both the subtalar and tibiotalar joints. Because of the extensive disruption to the blood supply (artery of the tarsal canal, deltoid branches, and artery of the sinus tarsi), the rate of avascular necrosis approaches 80-100%.
Question 64:
A 40-year-old male is scheduled for open reduction and internal fixation of a Sanders Type III calcaneus fracture via an extensile lateral approach. During the development of the full-thickness subperiosteal flap, which nerve is at greatest risk of iatrogenic injury?
Options:
- Sural nerve
- Superficial peroneal nerve
- Deep peroneal nerve
- Medial calcaneal nerve
- Saphenous nerve
Correct Answer: Sural nerve
Explanation:
The sural nerve courses along the lateral aspect of the hindfoot and is at significant risk during the extensile lateral approach to the calcaneus. The incision must be carefully planned, and a full-thickness subperiosteal flap must be elevated utilizing 'no-touch' retraction techniques to minimize traction injury or transection of the sural nerve.
Question 65:
A 45-year-old male presents with a Schatzker Type IV tibial plateau fracture with a large posteromedial shear fragment. The surgeon plans a posteromedial approach with the patient in the prone position. The optimal internervous/intermuscular interval for this approach is between the:
Options:
- Medial head of the gastrocnemius and the soleus
- Medial head of the gastrocnemius and the pes anserinus
- Lateral head of the gastrocnemius and the biceps femoris
- Tibialis posterior and the flexor hallucis longus
- Semimembranosus and the semitendinosus
Correct Answer: Medial head of the gastrocnemius and the pes anserinus
Explanation:
The posteromedial approach to the tibial plateau utilizes the interval between the medial head of the gastrocnemius (which is retracted laterally, protecting the neurovascular bundle) and the pes anserinus/semimembranosus tendons (which are retracted medially). This provides excellent visualization for buttress plating of posteromedial shear fragments.
Question 66:
A 35-year-old male sustains a high-energy OTA 43-C3 distal tibia pilon fracture. On presentation, the skin is tense with hemorrhagic fracture blisters. He is initially managed with a joint-spanning external fixator. What is the most reliable clinical indicator that the soft tissues are ready for definitive open reduction and internal fixation?
Options:
- Resolution of hemorrhagic blisters with epithelialization and presence of the 'wrinkle sign'
- Normalization of the erythrocyte sedimentation rate (ESR)
- 72 hours post-injury regardless of swelling
- Pin site drainage from the external fixator
- Appearance of bridging callus on radiographs
Correct Answer: Resolution of hemorrhagic blisters with epithelialization and presence of the 'wrinkle sign'
Explanation:
Pilon fractures are frequently associated with severe soft tissue compromise. Standard protocol involves a staged approach: immediate spanning external fixation followed by definitive ORIF once the soft tissues have recovered. The 'wrinkle sign'—the return of normal skin wrinkling with resolution of tense edema and re-epithelialization of blisters—is the most reliable clinical sign that the soft tissue envelope can safely tolerate surgical incisions, typically occurring 10-14 days post-injury.
Question 67:
A 65-year-old female presents with wrist pain after a fall. Radiographs reveal a volar Barton's fracture of the distal radius. Which of the following describes the pathognomonic feature of this fracture pattern?
Options:
- Extra-articular fracture with dorsal angulation of the distal fragment
- Intra-articular fracture characterized by volar subluxation of the carpus with the volar articular fragment
- Isolated fracture of the radial styloid
- Metaphyseal comminution with extension into the distal radioulnar joint (DRUJ) without radiocarpal involvement
- Fracture-dislocation of the radiocarpal joint with intact volar ligaments and a dorsal shear fragment
Correct Answer: Intra-articular fracture characterized by volar subluxation of the carpus with the volar articular fragment
Explanation:
A volar Barton's fracture is a shear fracture of the volar lip of the distal radius articular surface. Its pathognomonic feature is that the carpus remains articulated with the fractured volar fragment and subluxates or dislocates volarly along with it. It typically requires open reduction and internal fixation with a volar buttress plate.
Question 68:
A 28-year-old male involved in a high-speed motor vehicle collision sustains an anteroposterior compression type III (APC-III) pelvic ring injury. After successful hemodynamic resuscitation and application of a pelvic binder, what is the most appropriate definitive orthopedic management?
Options:
- Anterior symphyseal plating alone
- Percutaneous posterior sacroiliac screw fixation alone
- Both anterior symphyseal fixation and posterior pelvic ring stabilization
- Application of an anterior supra-acetabular external fixator alone
- Non-operative management with skeletal traction
Correct Answer: Both anterior symphyseal fixation and posterior pelvic ring stabilization
Explanation:
An APC-III pelvic ring injury is rotationally and vertically unstable, characterized by complete disruption of the pubic symphysis (or rami) anteriorly, and complete disruption of the anterior and posterior sacroiliac ligaments posteriorly. Definitive management necessitates stabilization of both the anterior and posterior ring to restore stability and pelvic volume.
Question 69:
On the standard AP pelvis radiograph of a 40-year-old male trauma patient, the iliopectineal line is disrupted, but the ilioischial line and the posterior wall margin remain intact. According to the Letournel and Judet classification, which structural component of the acetabulum is fractured?
Options:
- Anterior column
- Posterior column
- Transverse
- T-shaped
- Posterior wall
Correct Answer: Anterior column
Explanation:
The radiographic lines of the acetabulum on an AP pelvis view correlate with specific anatomical structures. The iliopectineal line represents the anterior column, and the ilioischial line represents the posterior column. Disruption of the iliopectineal line with an intact ilioischial line indicates an isolated anterior column fracture.
Question 70:
A 24-year-old male sustains a distal femur fracture after a motorcycle accident. A computed tomography (CT) scan is obtained to characterize the articular involvement, revealing a coronal plane fracture of the lateral femoral condyle. What is the eponymous name of this fracture?
Options:
- Barton fracture
- Chauffeur's fracture
- Hoffa fracture
- Tillaux fracture
- Chaput fracture
Correct Answer: Hoffa fracture
Explanation:
A Hoffa fracture is a coronal plane fracture of the femoral condyle (most commonly the lateral condyle). Because it is an intra-articular shear fracture, it requires rigid anatomic fixation, typically with anterior-to-posterior (AP) or posterior-to-anterior (PA) lag screws, often supplemented with a neutralization plate.
Question 71:
A 30-year-old male sustains a subtrochanteric fracture of the femur. Which combination of muscles is primarily responsible for the typical flexion, abduction, and external rotation deformity of the proximal fracture fragment?
Options:
- Flexion by iliopsoas, abduction by gluteus medius/minimus, external rotation by short external rotators
- Flexion by rectus femoris, abduction by tensor fasciae latae, external rotation by gluteus maximus
- Extension by hamstrings, adduction by adductor longus, internal rotation by gluteus minimus
- Flexion by sartorius, abduction by gluteus maximus, external rotation by piriformis
- Flexion by pectineus, adduction by adductor magnus, internal rotation by obturator internus
Correct Answer: Flexion by iliopsoas, abduction by gluteus medius/minimus, external rotation by short external rotators
Explanation:
In subtrochanteric fractures, the proximal fragment is acted upon by robust muscular forces causing a predictable deformity: the iliopsoas flexes the fragment, the gluteus medius and minimus abduct it, and the short external rotators externally rotate it. The distal fragment is pulled proximally and adducted by the hamstrings and adductor musculature.
Question 72:
A 75-year-old female undergoes cephalomedullary nailing for a reverse obliquity intertrochanteric femur fracture. To minimize the risk of lag screw cut-out from the femoral head, the surgeon utilizes the Tip-Apex Distance (TAD) concept described by Baumgaertner. What is the maximum recommended TAD to effectively reduce the risk of cut-out?
Options:
- 10 mm
- 15 mm
- 20 mm
- 25 mm
- 35 mm
Correct Answer: 25 mm
Explanation:
The Tip-Apex Distance (TAD) is the sum of the distance from the tip of the lag screw to the apex of the femoral head on the AP and lateral radiographs. Baumgaertner demonstrated that a TAD of less than 25 mm is highly predictive of successful fixation, whereas a TAD > 25 mm significantly increases the risk of lag screw cut-out.
Question 73:
A 25-year-old male sustains a Pauwels Type III (high vertical shear angle) femoral neck fracture. Biomechanical studies have demonstrated that using a sliding hip screw with a derotation screw, compared to three parallel cannulated cancellous screws, provides which of the following advantages for this specific fracture pattern?
Options:
- Elimination of the risk of avascular necrosis
- Superior construct stiffness and resistance to vertical shear forces
- Increased fracture gap to promote secondary bone healing
- Decreased operative time and blood loss
- Preservation of the lateral epiphyseal vessels
Correct Answer: Superior construct stiffness and resistance to vertical shear forces
Explanation:
Pauwels Type III femoral neck fractures have a fracture line greater than 50 degrees relative to horizontal, creating massive vertical shear forces. Biomechanical studies show that a fixed-angle device such as a sliding hip screw (often supplemented with a derotation screw) provides superior construct stiffness and resists vertical shear and varus collapse much better than three parallel cannulated screws.
Question 74:
A 40-year-old male presents to the emergency department after a fall onto an outstretched hand, sustaining a 'terrible triad' injury of the elbow. Which of the following is NOT a classic component of this injury pattern?
Options:
- Elbow dislocation
- Radial head fracture
- Coronoid process fracture
- Disruption of the lateral collateral ligament (LCL) complex
- Olecranon fracture
Correct Answer: Olecranon fracture
Explanation:
The 'terrible triad' of the elbow historically refers to an elbow dislocation associated with a radial head fracture and a coronoid fracture. The dislocation universally causes disruption of the lateral collateral ligament (LCL) complex (and often the MCL). An olecranon fracture is not a component of the terrible triad; injuries with olecranon fractures, coronoid fractures, and radial head fractures are typically transolecranon fracture-dislocations.
Question 75:
A 65-year-old female sustains a displaced 4-part proximal humerus fracture. According to Hertel's radiographic criteria, which of the following is the strongest predictor of subsequent avascular necrosis (ischemia) of the humeral head?
Options:
- Displacement of the greater tuberosity greater than 5 mm
- Posteromedial metaphyseal hinge length (calcar extension) less than 2 mm
- Varus angulation of the humeral head greater than 20 degrees
- Inferior subluxation of the humeral head
- Valgus impaction of the humeral head
Correct Answer: Posteromedial metaphyseal hinge length (calcar extension) less than 2 mm
Explanation:
Hertel identified specific radiographic predictors for ischemia (AVN risk) of the humeral head following proximal humerus fractures. The most reliable predictors are a posteromedial metaphyseal hinge length (calcar extension) of less than 2 mm, an absent medial hinge (medial displacement of the shaft > 2mm), and an anatomical neck (basicervical) fracture pattern.
Question 76:
A 22-year-old collegiate football player sustains a midfoot injury during a tackle. Weight-bearing radiographs demonstrate 3 mm of widening between the base of the first and second metatarsals, with a 'fleck sign' visible in the intercuneiform space. What is the most appropriate management for this athlete?
Options:
- Non-weight-bearing in a short leg cast for 6 weeks
- Immediate return to play with a rigid carbon-fiber orthotic
- Open reduction and internal fixation or primary arthrodesis of the Lisfranc complex
- Corticosteroid injection into the tarsometatarsal joints
- Closed reduction and percutaneous pinning with smooth Kirschner wires
Correct Answer: Open reduction and internal fixation or primary arthrodesis of the Lisfranc complex
Explanation:
The presentation describes a ligamentous Lisfranc injury with instability (diastasis > 2 mm and a positive 'fleck sign' representing avulsion of the Lisfranc ligament). Non-operative management is inadequate for unstable injuries. Stable anatomic fixation via Open Reduction Internal Fixation (ORIF) or primary arthrodesis is required to prevent debilitating post-traumatic midfoot arthrosis.
Question 77:
A 20-year-old basketball player presents with chronic lateral foot pain that acutely worsened during a game. Radiographs reveal a transverse fracture of the fifth metatarsal base located strictly at the metaphyseal-diaphyseal junction, extending into the intermetatarsal articulation between the 4th and 5th metatarsals. What is the classification of this fracture and the recommended treatment for an elite athlete?
Options:
- Zone 1 (Pseudo-Jones fracture); managed with a walking boot
- Zone 2 (Jones fracture); managed with intramedullary screw fixation
- Zone 3 (Diaphyseal stress fracture); managed with excision of the proximal fragment
- Zone 2 (Jones fracture); managed with conservative casting for 8 weeks
- Zone 3 (Diaphyseal stress fracture); managed with conservative casting
Correct Answer: Zone 2 (Jones fracture); managed with intramedullary screw fixation
Explanation:
This fracture is at the metaphyseal-diaphyseal junction, classifying it as a Zone 2 or 'true' Jones fracture. Due to a vascular watershed area, it has a high risk of delayed union or nonunion. For high-demand or elite athletes, intramedullary screw fixation is the standard of care to maximize healing rates and expedite return to sport compared to conservative management.
Question 78:
A 30-year-old male sustains a traumatic knee dislocation (KD-III) following a motor vehicle collision. After prompt closed reduction in the trauma bay, the foot is warm with palpable dorsalis pedis and posterior tibial pulses. The Ankle-Brachial Index (ABI) is measured at 0.8. What is the most appropriate next step in management?
Options:
- Discharge with a knee immobilizer and outpatient follow-up
- Serial clinical examinations and repeat ABI in 24 hours
- Immediate CT angiography (CTA) of the lower extremity
- Immediate prophylactic four-compartment fasciotomy
- Application of a spanning external fixator without further vascular workup
Correct Answer: Immediate CT angiography (CTA) of the lower extremity
Explanation:
Traumatic knee dislocations have a high rate of popliteal artery injury. Even if pulses are palpable, an ABI of less than 0.9 is highly predictive of an occult arterial intimal injury or disruption. Immediate advanced vascular imaging, most commonly CT angiography (CTA), is mandatory to definitively rule out a surgical vascular lesion.
Question 79:
A 25-year-old male undergoes open reduction and internal fixation for a pronation-external rotation (PER) ankle fracture. After fibular plating and medial malleolus fixation, a 'hook test' (Cotton test) is performed intraoperatively, demonstrating 4 mm of lateral translation of the fibula relative to the tibia. What is the most appropriate next step?
Options:
- Accept the reduction, as 4 mm of translation is within normal physiologic limits
- Perform a primary repair of the deltoid ligament only
- Place a syndesmotic position screw or dynamic suture-button device
- Revise the fibular plate to a longer locking plate
- Perform a primary arthrodesis of the distal tibiofibular joint
Correct Answer: Place a syndesmotic position screw or dynamic suture-button device
Explanation:
A positive intraoperative hook test (Cotton test) demonstrating lateral translation of the fibula greater than 2-3 mm indicates ongoing syndesmotic instability despite bony fixation. The appropriate management is stabilization of the syndesmosis, utilizing either trans-syndesmotic position screws or dynamic suture-button devices.
Question 80:
A 19-year-old male cyclist falls directly onto his left shoulder, sustaining a midshaft clavicle fracture. Which of the following clinical scenarios is widely considered an absolute indication for acute open reduction and internal fixation (ORIF) of the clavicle?
Options:
- 1.5 cm of shortening of the clavicle
- 10 degrees of angulation
- Presence of an open fracture
- Concomitant closed head injury
- Patient desire for rapid return to athletic competition
Correct Answer: Presence of an open fracture
Explanation:
Absolute indications for open reduction and internal fixation of a clavicle fracture include open fractures, fractures with associated neurovascular compromise, and severe skin tenting that threatens skin viability (impending open fracture). Shortening, displacement, and patient activity level are relative indications.
Question 81:
A 42-year-old male sustains a closed scapula fracture in a motorcycle collision. Which of the following radiographic findings represents the most widely accepted indication for operative fixation of a scapular body/neck fracture?
Options:
- 10 mm of medial translation of the glenohumeral joint
- 30 degrees of angular deformity of the scapular neck
- Glenoid articular step-off of 2 mm
- Glenopolar angle of 20 degrees
- Coracoid fracture with 5 mm of displacement
Correct Answer: Glenopolar angle of 20 degrees
Explanation:
Normal glenopolar angle (GPA) is 30 to 45 degrees. A GPA of less than 22 degrees is considered an indication for operative management because it implies significant malrotation and inferior displacement of the glenoid fragment, which can lead to altered shoulder biomechanics and poor functional outcomes. Articular step-off >4-5 mm, medialization >20 mm, and angulation >40 degrees are also indications.
Question 82:
Six weeks following open reduction and internal fixation of a Hawkins type III talar neck fracture, a patient undergoes a follow-up radiograph. The radiograph demonstrates a subchondral radiolucent band in the talar dome. This radiographic finding:
Options:
- Indicates the presence of advanced avascular necrosis
- Is a poor prognostic sign for subtalar arthritis
- Indicates intact vascularity to the talar body
- Represents a nonunion of the talar neck
- Dictates the need for immediate bone grafting
Correct Answer: Indicates intact vascularity to the talar body
Explanation:
The subchondral radiolucency in the dome of the talus, seen 6 to 8 weeks post-injury, is known as the Hawkins sign. It represents subchondral atrophy due to hyperemia and disuse. Its presence is a highly reliable indicator of intact vascularity to the talar body and virtually excludes the development of avascular necrosis.
Question 83:
A 35-year-old male sustains a Sanders type III calcaneus fracture. He undergoes ORIF via an extensile lateral approach. Which of the following is the most frequent complication associated with this specific surgical approach?
Options:
- Sural nerve injury
- Tibial nerve palsy
- Wound edge necrosis and dehiscence
- Subtalar arthritis
- Flexor hallucis longus tethering
Correct Answer: Wound edge necrosis and dehiscence
Explanation:
The extensile lateral approach to the calcaneus is associated with a high rate of wound complications, including wound edge necrosis, dehiscence, and infection (reported up to 10-25%). Careful handling of the full-thickness soft tissue flap, avoiding sharp angles, and delaying surgery until the "wrinkle sign" appears are essential to minimize this risk. Subtalar arthritis is a common complication of the fracture itself, but wound issues are the most frequent complication specifically attributed to the extensile lateral approach.
Question 84:
A 45-year-old male sustains an anterior column and anterior wall acetabular fracture. An ilioinguinal approach is planned. During the exposure, the surgeon identifies a vascular structure passing over the superior pubic ramus connecting the external iliac and obturator systems. This structure is known as the corona mortis. What is the approximate incidence of this vascular variant?
Options:
- 5-10%
- 15-20%
- 40-50%
- 70-80%
- >95%
Correct Answer: 40-50%
Explanation:
The corona mortis ('crown of death') is a vascular anastomosis between the external iliac/inferior epigastric system and the obturator system. It crosses the superior pubic ramus. Its incidence varies in anatomic studies but is generally cited as approximately 40-50% (venous being more common than arterial). It is at risk during the ilioinguinal approach and intrapelvic approaches (Stoppa) and must be carefully ligated to avoid life-threatening hemorrhage.
Question 85:
A 28-year-old male sustains a closed, spiral fracture of the distal third of the humerus. On initial examination, he has an intact radial nerve pulse but is unable to extend his wrist or fingers. Closed reduction and splinting are performed. Post-reduction examination reveals persistent complete radial nerve palsy. What is the most appropriate management regarding the radial nerve?
Options:
- Immediate surgical exploration and nerve repair
- Observation with clinical and EMG follow-up at 6 weeks
- Urgent MRI of the humerus
- Immediate ORIF of the humerus with concurrent nerve exploration
- Ultrasound-guided nerve block
Correct Answer: Observation with clinical and EMG follow-up at 6 weeks
Explanation:
In closed humeral shaft fractures with radial nerve palsy (whether primary or secondary to closed reduction), the initial management is observation. Over 85% of radial nerve palsies in this setting will recover spontaneously. Holstein-Lewis fractures (distal third spiral fractures) have a higher incidence of radial nerve palsy, but even in these cases, observation is the standard of care for closed injuries unless there is a loss of nerve function AFTER a previously successful reduction where the nerve may have been entrapped, although many still observe post-reduction palsies if the reduction is acceptable. The AAOS guidelines recommend observation. Surgery is indicated for open fractures, vascular injury, or failure to recover clinically/EMG at 3-4 months.
Question 86:
A 32-year-old male presents after a high-speed ATV accident with an APC-II pelvic ring injury. Examination reveals a large, fluctuant area over the greater trochanter with overlying skin hypermobility and decreased sensation. Which of the following describes the pathophysiology of this clinical finding?
Options:
- Fasciocutaneous arterial avulsion
- Closed degloving injury separating the subcutaneous tissue from the underlying fascia
- Rupture of the gluteus medius muscle belly
- Subfascial hematoma due to superior gluteal artery injury
- Lymphatic disruption leading to a deep seroma
Correct Answer: Closed degloving injury separating the subcutaneous tissue from the underlying fascia
Explanation:
The clinical presentation describes a Morel-Lavallée lesion, which is a closed degloving injury resulting from a shearing force that separates the subcutaneous fat and skin from the underlying deep fascia. This creates a potential space that fills with blood, lymph, and necrotic fat. It is highly associated with pelvic and acetabular fractures. If unrecognized or untreated, it can lead to skin necrosis and a high rate of deep infection following surgical fixation of underlying fractures.
Question 87:
A 40-year-old farmer sustains an open fracture of the tibia and fibula (Gustilo-Anderson Grade IIIA) from a tractor accident in a muddy field. According to current guidelines for severe open fractures in a highly contaminated agricultural environment, the most appropriate initial intravenous antibiotic regimen is:
Options:
- Cefazolin alone
- Cefazolin and Gentamicin
- Ceftriaxone alone
- Cefazolin, Gentamicin, and Penicillin G
- Vancomycin and Piperacillin/Tazobactam
Correct Answer: Cefazolin, Gentamicin, and Penicillin G
Explanation:
For a Grade III open fracture, current guidelines typically recommend a first-generation cephalosporin (e.g., Cefazolin) plus an aminoglycoside (e.g., Gentamicin). In the setting of agricultural injuries or gross fecal contamination, the addition of Penicillin G (or Ampicillin) is recommended to provide coverage against Clostridium species. High-dose penicillin is the drug of choice to prevent gas gangrene in farm-related severe open wounds.
Question 88:
A 55-year-old female sustains a high-energy varus stress injury to her knee. Radiographs and CT scan reveal a displaced fracture of the medial tibial plateau with a coronal plane fracture line exiting posteromedially. The lateral plateau is intact. According to the Schatzker classification, what type of fracture is this, and what is the optimal surgical approach?
Options:
- Schatzker II, Anterolateral approach
- Schatzker IV, Posteromedial approach
- Schatzker V, Dual incisions (Anterolateral and Posteromedial)
- Schatzker VI, Anterior midline approach
- Schatzker III, Arthroscopic-assisted percutaneous fixation
Correct Answer: Schatzker IV, Posteromedial approach
Explanation:
An isolated medial tibial plateau fracture is a Schatzker type IV injury. It is typically a high-energy injury with significant soft tissue trauma and varus instability. The posteromedial fragment is best addressed via a posteromedial approach with anti-glide plating, as standard anteromedial or medial plates often fail to adequately capture and buttress the posteromedial shear fragment.
Question 89:
A 65-year-old female with a history of breast cancer presents with right thigh pain. Radiographs reveal a 2 cm lytic lesion in the peritrochanteric region of the proximal femur. It is moderately painful with weight-bearing but does not involve the cortex circumferentially. Based on Mirels' criteria, what is her calculated score, and what is the recommendation for prophylactic fixation?
Options:
- Score 7; Observation with radiation therapy
- Score 8; Borderline, consider prophylactic fixation
- Score 9; Prophylactic fixation recommended
- Score 10; Prophylactic fixation strongly recommended
- Score 11; Immediate prophylactic fixation and arthroplasty
Correct Answer: Score 9; Prophylactic fixation recommended
Explanation:
Mirels' criteria assess the risk of pathological fracture based on four factors (Site, Pain, Lesion type, Size). Site: Peritrochanteric = 3 points. Pain: Moderate = 2 points. Lesion type: Lytic = 3 points. Size: 1/3 to 2/3 of cortex roughly equates to 2 points. 3+2+3+1 = 9. A score of 9 or greater indicates prophylactic internal fixation is recommended.
Question 90:
A 22-year-old professional football player sustains an acute, closed injury to his foot during a game. Radiographs show a transverse fracture through the diaphyseal-metaphyseal junction of the fifth metatarsal base, involving the 4th-5th intermetatarsal articulation. What is the most appropriate management for this elite athlete to ensure the fastest return to play with the lowest risk of nonunion?
Options:
- Non-weight bearing cast for 6-8 weeks
- Weight-bearing as tolerated in a stiff-soled shoe
- Intramedullary screw fixation
- Open reduction and internal fixation with a mini-fragment plate
- Primary bone grafting and immobilization
Correct Answer: Intramedullary screw fixation
Explanation:
This is a Zone 2 fracture of the proximal fifth metatarsal, also known as a Jones fracture. It involves the metaphyseal-diaphyseal junction and extends into the 4th-5th intermetatarsal facet. Due to a vascular watershed area, it has a high risk of delayed union or nonunion. In elite athletes, early intramedullary screw fixation is recommended to decrease the time to union, minimize the risk of nonunion, and allow for a faster return to sport compared to conservative management.
Question 91:
A 30-year-old male sustains a femoral neck fracture following a fall from height. Radiographs demonstrate a vertically oriented fracture line with an angle of 75 degrees relative to the horizontal. According to Pauwels' classification, this fracture is characterized by:
Options:
- High compressive forces and low shear forces, favoring primary bone healing
- High shear forces, leading to a high rate of nonunion and varus collapse
- Extracapsular involvement, requiring dynamic hip screw fixation
- Low risk of avascular necrosis due to intact retinacular vessels
- Stability in flexion and extension, allowing early weight-bearing
Correct Answer: High shear forces, leading to a high rate of nonunion and varus collapse
Explanation:
Pauwels' classification is based on the angle of the fracture line relative to the horizontal. Type I is <30 degrees, Type II is 30-50 degrees, and Type III is >50 degrees. A 75-degree angle is a Pauwels type III fracture. These vertically oriented fractures are subjected to high shear forces rather than compressive forces across the fracture site, leading to a high rate of nonunion, varus collapse, and hardware failure. Fixation often requires a sliding hip screw with a derotation screw or specialized fixed-angle constructs to counteract these shear forces in young patients.
Question 92:
A 25-year-old male sustains a closed comminuted tibial shaft fracture. He complains of severe pain out of proportion to the injury. Which of the following clinical or objective findings is the most reliable indicator for emergent fasciotomy?
Options:
- Loss of dorsalis pedis and posterior tibial pulses
- Intracompartmental pressure of 25 mmHg
- Delta pressure (Diastolic blood pressure minus intracompartmental pressure) of 20 mmHg
- Capillary refill time greater than 3 seconds
- Mild swelling and pain with active toe flexion
Correct Answer: Delta pressure (Diastolic blood pressure minus intracompartmental pressure) of 20 mmHg
Explanation:
Acute compartment syndrome is a clinical diagnosis, but when objective measurement is used, the delta pressure is the most reliable parameter. Delta pressure = Diastolic BP - Intracompartmental pressure. A delta pressure of 30 mmHg or less (e.g., 20 mmHg) is a strong indication for emergent fasciotomy. Loss of pulses and capillary refill changes are late and unreliable signs (pulses usually remain intact). An absolute pressure of 25 mmHg alone is not necessarily an indication for surgery without considering the patient's blood pressure.
Question 93:
A 45-year-old male presents with a high-energy closed pilon fracture (OTA/AO 43-C3) with severe soft tissue swelling and fracture blisters. The standard of care for the initial management of this injury involves:
Options:
- Immediate open reduction and internal fixation of the tibia and fibula
- Closed reduction and placement in a long leg cast
- Spanning external fixation and delayed definitive fixation in 10-14 days
- Immediate intramedullary nailing of the tibia
- Primary tibiotalar arthrodesis
Correct Answer: Spanning external fixation and delayed definitive fixation in 10-14 days
Explanation:
High-energy pilon fractures are associated with severe soft tissue injury. Immediate open reduction and internal fixation (ORIF) carries an unacceptably high risk of wound complications, necrosis, and deep infection. The standard of care is a staged protocol: initial closed reduction and application of a spanning external fixator (with or without initial fibular fixation) to restore length and alignment, followed by delayed definitive ORIF of the tibial articular surface 10-21 days later, once the soft tissue envelope has recovered (evidenced by resolving edema and the appearance of skin wrinkles).
Question 94:
A 60-year-old female presents with a wrist injury after falling on an outstretched hand. Radiographs reveal a fracture of the volar lip of the distal radius with volar subluxation of the carpus along with the fracture fragment. Which of the following describes the fundamental mechanical instability of this fracture?
Options:
- Tension failure of the dorsal cortex
- Compression failure of the scaphoid fossa
- Shear failure of the volar articular margin
- Avulsion of the radioscaphocapitate ligament
- Axial impaction of the lunate into the radius
Correct Answer: Shear failure of the volar articular margin
Explanation:
A volar Barton's fracture is a shear fracture of the volar articular margin of the distal radius. The carpus subluxates volarly with the fracture fragment because the strong volar radiocarpal ligaments remain attached to the volar marginal fragment. Due to the shear forces and intrinsic instability, conservative management often fails, and volar buttress plating is the treatment of choice to resist the shear forces and maintain anatomic reduction.
Question 95:
A 28-year-old male is brought to the emergency department after a severe motorcycle accident. He has an obvious deformity of his left knee. Radiographs confirm an anterior knee dislocation, which is successfully reduced. Pulses are palpable, but the Ankle-Brachial Index (ABI) on the affected limb is 0.85. What is the most appropriate next step in management?
Options:
- Discharge with a knee immobilizer and outpatient follow-up
- Serial clinical examinations every 4 hours for 24 hours
- Immediate CT angiography of the lower extremity
- Emergent operative exploration of the popliteal artery
- Application of an external fixator
Correct Answer: Immediate CT angiography of the lower extremity
Explanation:
Knee dislocations have a high rate of associated popliteal artery injury. Even if pulses are present after reduction, an Ankle-Brachial Index (ABI) should be performed. An ABI less than 0.90 is highly suspicious for a vascular injury (such as an intimal tear or flow-limiting lesion) and warrants further advanced imaging, typically CT angiography, to evaluate the popliteal artery. Immediate surgical exploration is indicated for hard signs of vascular injury (expanding hematoma, absent pulses, pulsatile bleeding), but an ABI of 0.85 with palpable pulses mandates a CTA.
Question 96:
During open reduction and internal fixation of a severe supracondylar/intercondylar distal femur fracture (OTA/AO 33-C3) via a lateral approach, the surgeon identifies a separate, coronal plane fracture of the lateral femoral condyle. This fragment is often missed on plain AP and lateral radiographs. Which of the following represents the optimal fixation strategy for this specific fragment?
Options:
- Posterior-to-anterior directed lag screws
- Anterior-to-posterior directed lag screws, countersunk beneath the articular cartilage
- A separate medial buttress plate
- Intramedullary nailing
- Resection of the fragment and osteochondral allograft
Correct Answer: Anterior-to-posterior directed lag screws, countersunk beneath the articular cartilage
Explanation:
A coronal plane fracture of the femoral condyle is known as a Hoffa fracture (OTA/AO 33-B3). It is typically located posterior to the mid-axial line. Optimal biomechanical fixation for a Hoffa fracture is achieved with anterior-to-posterior (AP) directed lag screws. To avoid joint irritation, the screws must be countersunk beneath the articular cartilage. PA screws are biomechanically less stable and technically more challenging to insert via standard approaches.
Question 97:
A 35-year-old male twisted his midfoot while stepping off a curb. Plain non-weight-bearing radiographs of the foot are interpreted as normal. However, he continues to have severe pain over the tarsometatarsal joints and inability to bear weight. Which of the following imaging modalities or techniques is the most appropriate next step to rule out a subtle Lisfranc injury?
Options:
- MRI of the foot
- CT scan of the foot without contrast
- Weight-bearing AP, lateral, and oblique radiographs of both feet
- Ultrasound of the dorsal midfoot ligaments
- Three-phase bone scan
Correct Answer: Weight-bearing AP, lateral, and oblique radiographs of both feet
Explanation:
Subtle Lisfranc (tarsometatarsal) injuries can be missed on standard non-weight-bearing radiographs in up to 20% of cases. The most appropriate initial step for a suspected subtle Lisfranc injury with normal non-weight-bearing films is to obtain weight-bearing radiographs of both feet to stress the joint dynamically and compare it to the contralateral, normal side. Findings such as widening of the space between the 1st and 2nd metatarsal bases (the 'fleck sign') or subluxation indicate injury. If weight-bearing films are inconclusive, MRI or weight-bearing CT may be used.
Question 98:
An 8-month follow-up radiograph of a tibial shaft fracture treated with a cast shows a 'horse-shoe' or 'elephant foot' appearance at the fracture site, with abundant callus formation but a persistent radiolucent fracture line. The patient reports pain with walking. The underlying cause and the most appropriate treatment principle for this condition are:
Options:
- Biologic failure; requires decortication and bone grafting
- Infection; requires thorough debridement and culture-specific antibiotics
- Mechanical instability; requires rigid internal fixation
- Avascular necrosis; requires free vascularized fibular graft
- Malnutrition; requires Vitamin D and calcium supplementation
Correct Answer: Mechanical instability; requires rigid internal fixation
Explanation:
The 'elephant foot' or 'horse-shoe' appearance describes a hypertrophic nonunion. Hypertrophic nonunions are characterized by abundant, well-vascularized callus that fails to bridge the fracture site. The biological potential for healing is excellent, but the biological process is thwarted by inadequate mechanical stability (excessive motion at the fracture site). The primary treatment principle is to provide rigid mechanical stability (e.g., via intramedullary nailing or compression plating); bone grafting is generally not required.
Question 99:
A 45-year-old male falls onto his outstretched hand and sustains a 'terrible triad' injury of the elbow. This injury pattern typically includes a posterior elbow dislocation, a radial head fracture, and a fracture of which of the following structures?
Options:
- Olecranon
- Coronoid process
- Capitellum
- Medial epicondyle
- Lateral supracondylar ridge
Correct Answer: Coronoid process
Explanation:
The 'terrible triad' of the elbow consists of a posterior elbow dislocation, a radial head or neck fracture, and a fracture of the coronoid process. This injury is characterized by severe instability. Treatment focuses on restoring stability by repairing or reconstructing the lateral collateral ligament (LCL) complex, fixing or replacing the radial head, and addressing the coronoid fracture (typically if it involves the anteromedial facet or is a large fragment) to restore the anterior buttress.
Question 100:
A 30-year-old cyclist falls directly onto his shoulder. Radiographs demonstrate a fracture of the distal third of the clavicle. The fracture is displaced, with the medial fragment elevated superiorly. According to the Neer classification, what type of distal clavicle fracture is associated with rupture of the coracoclavicular ligaments and has a high rate of nonunion if treated conservatively?
Options:
- Neer Type I
- Neer Type II
- Neer Type III
- Neer Type IV
- Neer Type V
Correct Answer: Neer Type II
Explanation:
Neer Type II distal clavicle fractures involve the region of the coracoclavicular (CC) ligaments. In Type II fractures, the CC ligaments are detached from the medial fragment, which is consequently displaced superiorly by the pull of the trapezius. The lateral fragment remains attached to the acromion. Because of the significant displacement and deforming forces, Neer Type II fractures have a nonunion rate of up to 30% when treated non-operatively, and surgical fixation is frequently recommended for active patients.