Orthopedic Ob Trauma D Review | Dr Hutaif Trauma & Frac -...

Key Takeaway
For anyone wondering about ORTHOPEDIC MCQS ONLINE OB 20 TRAUMA 2D, Poor pre-injury cognitive function significantly increases mortality for patients femur fracture, particularly hip fractures. Studies show that pre-injury functional independence and cognitive scores are independent predictors of functional outcome and survival. This is especially true for elderly patients with displaced femoral neck fractures, where reduced cognition and mobility elevate mortality risk within the first year.
Orthopedic Ob Trauma D Review | Dr Hutaif Trauma & Frac -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
Poor pre-injury cognitive function has been proven to increase mortality for which of the following injuries?

Explanation
Hip fractures are common injuries and typically sustained from a standing level fall in the elderly. These fragility fractures can be a clinical sign of overall decline of the patient, and when coupled with poor pre-injury cognitive function and decreased mobility, mortality rates are increased as compared to
patients of the same age.
The Soderqvist et al study showed that a Short Portable Mental Status Questionnaire score of <3 and male gender were associated with an increased mortality rate during the first twelve months. Moreover, patients with a score of <3 had a significantly worse outcome with regard to the ability to walk and to perform the activities of daily living.
The referenced study by Holt et al is a prospective review of 1000 hip fractures and reported that pre-injury mobility to be the most significant determinant for post-operative survival.
The referenced study by Cornwall et al found that six-month mortality was lowest for patients with nondisplaced femoral neck fractures (5.7%) and highest for patients with displaced femoral neck fractures (15.8%), but multivariate analysis only identified preinjury function as an independent predictor of mortality.
Illustration A shows a displaced femoral neck fracture in an elderly patient. Incorrect Answers:
1,2,3,5: These injuries can be associated with elderly patients and are common
fragility fractures. However, no relationship between mortality and pre-injury cognitive function has been established at this point with any of these fractures.
Question 2
A 55-year-old male sustained the injury in Figure A. His injury was complicated by an acute compartment syndrome. He underwent external fixation of his extremity and four compartment fasciotomy. When should the treatment shown in Figure B be performed to minimize the risk of infection?

Explanation
The incidence of compartment syndrome is high in tibial plateau fractures. In the presence of tense anterior and lateral tibial compartments, combined with pain with passive stretch of involved muscles or unrelenting pain, compartment pressures should be measured and fasciotomies performed when necessary.
Schatzker type V and VI fractures are more likely to have this potential complication. Examination of leg compartments should be repeated at regular intervals because compartment syndrome may occur 24 hours or more after injury.
Zura et al. performed a study to analyze whether there is an association between infection and the timing of definitive fracture fixation in relation to fasciotomy closure or coverage. They found that no statistical difference in the rate of infection when tibial plateau fractures with four-compartment fasciotomies were treated with open reduction and internal fixation before fasciotomy closure, at fasciotomy closure, or after fasciotomy closure. They conclude that timing of definitive fracture treatment can be determined by the medical condition of the patient.
Shah et al. performed a retrospective chart review of all bicondylar tibial plateau fractures that had fixation with two incisions. They reported an infection rate of 13.8% which is lower than historical reports. They concluded that the lower infection rate was due to their treatment algorithm that requires recovery of the soft tissue envelope prior to definitive fixation.
Figure A demonstrates a bicondylar tibial plateau fracture. Figure B demonstrates fixation of a tibial plateau fracture through a dual plating technique.
Incorrect Answers:
Answers 1, 2, 3, and 4 are incorrect as infection risk is unchanged with timing of definitive fracture fixation.
Question 3
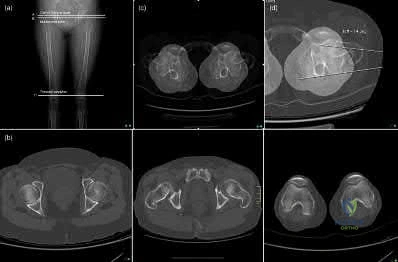
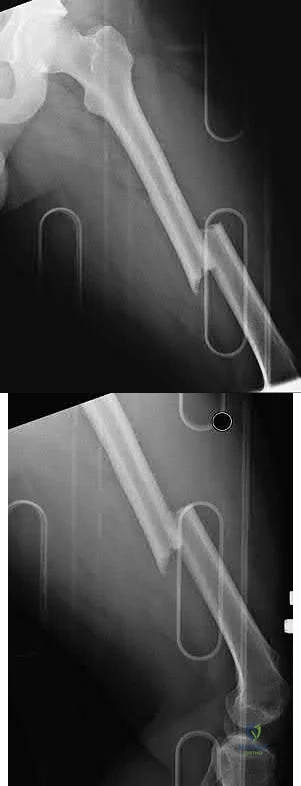
A 37-year-old male sustained the injury shown in figure A. He was treated with an intramedurally nail and a post-operative radiograph is shown in figure B. He underwent a post-operative CT Scanogram to assess for rotation. Figures C and D are of the operative side and Figures E and F are of the uninjured side. What is the version of the injured side and should any further procedures be undertaken for correction?

Explanation
Rotational malalignment or torsional deformity is expressed as a difference in femoral version between the injured and uninjured leg. It can be measured clinically, radiograpically, and most accurately by CT scan. CT scan is the method of choice because of its reliability and reproducibility. The incidence of rotational malalignment may be as high 30% in some fracture patterns.
Fracture comminution is a risk for rotational malalignment as it alters the ability to obtain a cortical read. Differences between sides of <10 degrees are considered variations of normal while differences of >15 degrees are considered true torsional deformities and likely require de-rotation.
Jaarsma et al. detail how to obtain a rotational profile of the femur. Rotational alignment is determined by the angle between a line tangential to the femoral condyles and a line drawn through the axis of the femoral neck. The difference in angle between the fractured and unaffected side determines the rotational alignment. A decrease in anteversion of the femoral neck of the fractured side implies increased external rotation and an increase denotes increased internal rotation of the distal fragment.
Koerner et al. measured 328 normal femora and found that there were no statistically significant differences in mean version between African American, white, and Hispanic patients for males or females. They found retroversion to be common in white males, African American males, and all females. They conclude that this may have implications in proper alignment restoration after IM nailing of femur fractures.
Gardner et al. performed a cadeveric study and found that freehand distal interlocking may be a substantial cause of rotational deformity. They found that freehand insertion may cause a 7 degree change in alignment. They saw that when inserting the drill freehand, drill/nail contact caused a visible shift of the fracture site. They conclude that the use of computer navigation systems may improve this issue.
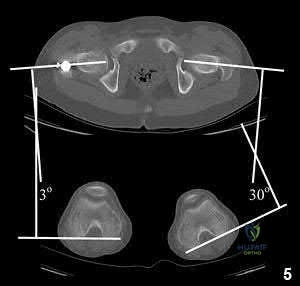
Figure A demonstrates a subtrochanteric femur fracture, while Figure B demonstrates the same fracture, stabilized with a piriformis entry nail. Figures C-F demonstrate axial CT cuts to determine femoral version. Figure C demonstrates hip anteversion of 18 degrees, while figure D reveals knee external rotation of 18 degrees. This side exhibits neutral rotation (18-18).
Figure E demonstrates hip anteversion of 9.2 degrees while figure F demonstrates knee external rotation of 3.2 degrees. This side exhibits 6 degrees of anteversion (9.2-3.2).
Incorrect Answers:
Answers 1, 2, 4, 5 do not have the correct combination of version and need for further procedures.
Question 4
A 33-year-old male suffers a gunshot to the right forearm as seen in figure A. There is a 2 cm radial-sided wound with exposed bone. What is the most appropriate treatment?

Explanation
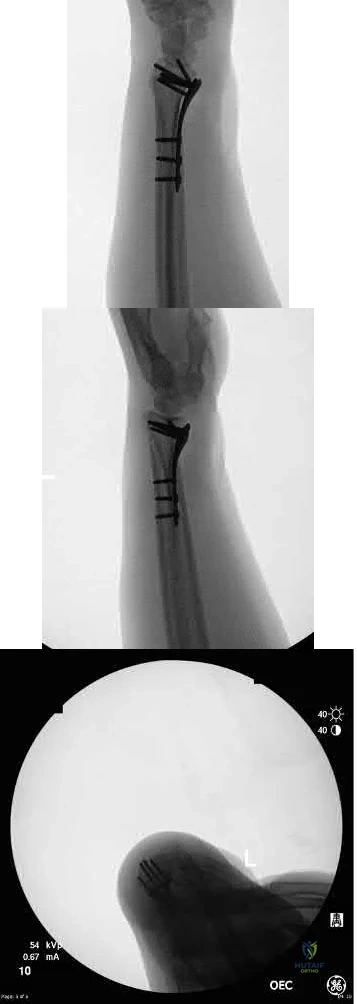
Diaphyseal forearm fractures are best treated with open reduction and internal fixation to restore anatomic alignment and absolute stability. Typically this is achieved by the use of 3.5 mm plates, placed in such a manner to produce interfragmentary compression. Due to the comminution in this case, bridge plating will provide a superior outcome as it will minimize interfragmentary strain and preserve the local bone biology. Multiple studies have demonstrated that open reduction and internal fixation at the initial encounter is appropriate, even if there is comminution, bone loss, or an open injury requiring multiple debridements.
Anderson et al. performed a retrospective study of 87 patients with 129 diaphyseal forearm fractures treated with dynamic compression plates. Open fractures were fixed primarily and the overall union rate was 98%. Refracture occurred in 2 patients after removal of 4.5 mm plates, whereas there were no refractures after removal of the 3.5 mm plates.
Moed et al. reviewed 57 patients that underwent immediate internal fixation of a diaphyseal forearm fracture. Functional results were good to excellent in 85% of patients and there were 2 deep infections and 6 non-unions overall.
The authors conclude immediate plate fixation is an appropriate treatment method for open diaphyseal forearm fractures and recommend autogenous grafting at the time of wound closure.
Jones et al. analyzed a retrospective case series of 18 patients with grade 3 open diaphyseal forearm fractures treated with irrigation and debridement and immediate open reduction and internal fixation followed by aggressive soft tissue management over the following weeks. Their treatment protocol provided good to excellent results in 66% of patients, indicating immediate reduction and fixation may be an acceptable treatment for some patients.
Figure A demonstrates comminuted radius and ulna shaft fractures with retained bullet fragments.
Incorrect answers:
Answer 2: The patient has an open fracture which requires urgent debridement Answer 3: Compression plating will not work for this comminuted fracture pattern.
Answer 4: While bridge plating is appropriate, 4.5mm plates are too large and have an increased risk of refracture if later removal is required
Answer 5: External fixation is not necessary, this fracture can be treated with immediate open reduction and internal fixation.
Question 5
A 29-year-old obese patient is transferred from an outside facility for the management of a closed-head injury and the fracture shown in Figure A. He presents to the trauma bay as a transient responder to blood products, and undergoes urgent pre-surgical angiography embolization. Surgery is performed within 8 hours from the time of injury. The patient develops a deep wound infection 1 week post-operatively. Which of the following factors would be considered the MOST statistically significant predictor for post-operative infection in this patient.

Explanation
Wound complications following pelvic and acetabular fracture fixation is relatively uncommon. Literature suggests and prevalence of 2-8% with closed fracture injuries. Factors shown to increase infection rates include both patient and surgical factors. They include obesity, diabetes, immunocompromised, elderly, pre-operative embolization and open fractures.
Sagi et al. looked at the factors contributing to wound infection after pelvic and acetabular surgery. Open pelvic or acetabular fractures were excluded. Of all the factors, only obesity (OR 8, PPV 33%), obesity plus leukocytosis (OR 12, PPV 39%), and preoperative angioembolization (OR 11, PPV 67%) were strong predictors of postoperative infection.
Manson et al. aimed to determine if embolization of pelvic arterial injuries before open reduction and internal fixation (ORIF) of acetabular fractures is associated with an increased rate of deep surgical site infection. They retrospective reviewed 1440 patients who underwent ORIF of acetabular fractures. They found a 58% infection rate of the patients who underwent embolization before ORIF vs, historical controls (2%-5%) and angiography without embolization (14%).
Figure A shows an AP radiograph and 3D CT reconstruction of a APC3 pelvic ring fracture.
Incorrect Answers:
Answer 1: Head injury has not been shown to increase infection rates. It has been shown to increase heterotrophic ossification.
Answer 3: Gender has not shown to increase infection rates
Answer 4: Early surgery has not been shown to affect infection rates. Answer 5: Transfer from an outside facility has not been shown to affect infection rates.
Question 6
A 40-year-old man sustains a fall while mountain biking and presents with a posterior elbow fracture-dislocation. The elbow is reduced in the ER and noted to be grossly unstable with varus and valgus stress. Imaging demonstrates a two part radial head fracture involving 40% of the articular surface and a fracture involving less than 10% of the coronoid tip. He is taken to the OR for surgical reconstruction. After fixation of the radial head and repair of the LCL complex, the elbow is fluoroscopically examined and noted to be unstable with valgus stress. The elbow is ranged and dislocates at less
than 45 degrees of flexion with the forearm in full supination. What is the next best step in management?
Explanation
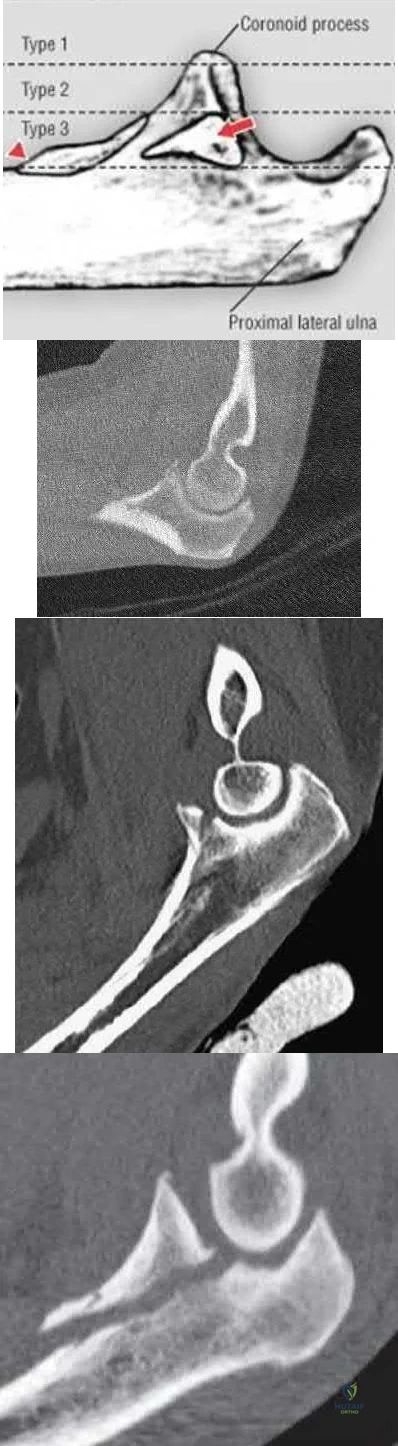
Terrible triad injuries of the elbow are characterized by: 1. Radial head fracture, 2. Coronoid fracture, and 3. Elbow dislocation. Whether to surgically address the coronoid fracture depends on the size of the fragment (Reagan-Morrey types I-III; Illustration A) as well as elbow stability. Reagan and Morrey suggested that small fractures of the coronoid tip (type I) involving less than 10% of the coronoid may represent anterior capsule avulsions; however, recent cadaveric studies demonstrate that the capsule inserts more distally on the tip and that small fractures often do not contain capsule insertion. Gross elbow instability in the presence of a type I fracture is most likely due to an independent MCL injury and NOT the coronoid avulsion. Surgical repair of type I fractures has not been shown to affect stability and may detrimentally affect elbow range of motion.
Matthew et al reviewed the terrible triad injury of the elbow. While the coronoid process provides substantial resistance to posterior subluxation, small fractures involving 10% of the coronoid process have been shown to have little effect on elbow stability. In a cadaveric study of a simulated terrible triad injury, when residual instability was present after radial head repair or arthroplasty and lateral ulnar collateral ligament (LUCL) repair, repair of the MCL was more effective than fixation of small coronoid fractures in restoring elbow stability. However, the authors note that in clinical series of terrible triad injuries, most coronoid fragments were larger than 10%, suggesting that fixation of the coronoid process is usually part of the treatment of terrible triad injuries.
Papatheodorou et al performed a retrospective analysis of 14 patients with acute terrible triad injuries and type I or type II coronoid fractures who
underwent radial head fixation or arthroplasty and LUCL repair without coronoid fixation. Intraoperative stability was confirmed under fluoroscopy. At 2 year follow up, none of the patients demonstrated elbow instability. Mean elbow flexion-extension was 123 and forearm rotation 145. The authors concluded that terrible triad injuries with type I or II coronoid fractures can be treated without coronoid fixation when intraoperative stability is restored with radial head repair or arthroplasty and LUCL repair.
Illustration A demonstrates the Regan-Morrey classification of coronoid fractures. Type I fractures involve < 10% of the coronoid tip and do not result in significant elbow instability. Type II fractures involve < 50% of the coronoid and may result in elbow instability secondary to loss of the anterior bony buttress that resists posterior displacement of the ulna, as well as loss of the anterior capsule insertion. These fractures are often repaired, particularly when associated with elbow instability. Type III fractures involve > 50% of the coronoid and often contain the insertion of the anterior band of the MCL (red arrow). The insertion of the brachialis (red triangle) may also be involved resulting in proximal displacement of the fracture fragment. Surgical repair of type III fractures is necessary to reconstitute the MCL and restore elbow stability. Illustration B is a CT scan of a type I coronoid fracture. Illustration C is a CT scan of a type II coronoid fracture. Illustration D is a CT scan of a type III coronoid fracture.
Incorrect Answers:
Answers 1: All possible ligamentous injuries should be addressed prior to proceeding with external fixation. If the elbow remains unstable following MCL repair, then external fixation may be considered.
Answer 2: Two part radial head fractures that involve more than 30% of the articular surface are most often treated with ORIF. Under-sizing the radial head arthroplasty component can result in residual valgus stability, as the radial head is a secondary stabilizer to valgus stress.
Answer 3: Coronoid fractures involving 10% of the coronoid tip do not affect elbow stability and therefore repair is not necessary.
Answer 5: Splinting at 90 degrees of flexion and full pronation is appropriate for a stable elbow following LCL repair in the presence of an uninjured MCL. This patient has a persistently unstable elbow likely secondary to a deficient MCL and therefore should not be splinted. Following MCL repair if the elbow remains persistently unstable, a hinged external fixator should be applied.
Question 7
Which of the following fluoroscopic views is used to assess
intra-articular screw penetration during volar fixation of a distal radius fracture?
Explanation
The amount of elevation will depend on the degree to which the surgeon restores radial inclination; for example, if the surgeon only restores 15° of radial inclination, then the surgeon would only have to elevate the wrist 15° from a true lateral in order to have the radiographic beam point down the joint line. Failure to diagnose intra-articular screws intraoperatively can lead to degenerative changes.
Tweet et al. performed a survey of orthopedic surgeons regarding their preferred method of visualizing screw placement during wrist fixation. The majority of surgeons reported that they obtain multiple views, including AP/PA wrist views, a 23° lateral inclination view, and a true lateral view. They also performed a cadaveric study looking at different x-ray views and screw penetration. They reported that live rotational fluoroscopy provided the highest sensitivity (93%) and specificity (96%) for the detection of intra-articular screw penetration.
Patel et al. evaluated the ability of surgeons at different levels to critically assess distal radius fixation and screw placement. They found that supplementation with a 23° lateral view increased accuracy and confidence in all position, specialty, and experience groups. Confidence scores were significantly higher following the evaluation of three views versus two views. Residents exhibited the greatest improvements in accuracy and confidence. For first-phase (standard view) assessments, accuracy scores were significantly better for attendings with less than 10 years of post-fellowship experience than those with more.
Illustration A is a non-elevated lateral of the wrist, while illustration B is a 23° elevated lateral radiograph. Illustration C is an example of a skyline view, which assesses for screws penetrating the dorsal cortex.
Incorrect Answers:
Answer 1: The dorsal skyline view shows dorsal screw length and is useful to
check for long distal screws.
Answers 2 and 3: The AP and PA wrist views do not show intra-articular screw penetration due to the volar tilt and concavity of the joint.
Answer 5: A 45° oblique lateral view does not visualize the joint as this angle does not match the radial inclination.
Question 8
A 46-year-old male sustains a patella fracture and is treated with cannulated screws and a tension band construct. Which of the following is correct regarding this treatment?

Explanation
Tension band constructs result in absolute stability when performed correctly. This technique works by converting tension from muscle pull into compressive force on the articular side of the fracture. Tension band constructs require a fracture pattern or bone that is able to withstand compression, an intact cortical buttress opposite to the tension band, and fixation that withstands tensile forces.
LeBrun et al. and associates evaluated functional outcomes of surgically isolated patella fractures. They reported that 52% of patients underwent surgery for hardware removal, and 38% of patients who retained their hardware reported pain at some time. They also found that nearly 20% had extensor lag, and almost 38% had restricted flexion. Extension power on testing showed significant mean deficits when compared to the contralateral side.
Bayar et al. evaluated 20 patients with patella fractures and found that articular incongruity of >1mm was the largest risk factor for quadriceps weakness at a mean of 30 months postoperatively. No significant differences were seen with sex, fracture pattern, or time from injury to surgery.
Illustration A shows patella fixation with plate/screw construct. Incorrect Answers:
Answer 1: Knee flexion arc is generally limited more than the non-injured side.
Answer 2: Extensor lag can be permanent with this treatment method. Answer 4: Quadriceps weakness is common after tension band fixation of patella fractures.
Answer 5: Patients generally have poorer outcomes after patella tension band fixation, regardless of implant maintenance or removal.
Question 9
A 55-year-old male is involved in a motorcycle crash and sustains a closed, right-sided, midshaft femur fracture. This is an isolated injury. He is treated with retrograde femoral nailing, and postoperatively is noted to have 30 degrees of internal rotation of the operative extremity, when compared with his nonsurgical side. Which of the following is the most likely cause of this malrotation deformity?
Explanation
Postsurgical internal malrotation after treatment for a diaphyseal femur fracture typically occurs either via internal rotation of the distal segment relative to the proximal or external rotation of the proximal segment relative to the distal. These clinical findings are consistent with an iatrogenic increase in femoral anteversion.
Dimitriou et al. performed a study to quantify the side-to-side anatomic variation in the proximal femur and the implications for preoperative planning and leg length discrepancy following hip arthroplasty. CT-based 3D femoral models were reconstructed for 122 paired femurs in 61 young healthy subjects with no history of hip pathology. Significant side-to-side differences were found in femoral anteversion, horizontal offset, and femoral head center location.
They concluded that relying on the anatomic landmarks of the contralateral femur during hip arthroplasty may not necessarily result in restoration of native anatomy and leg-length.
Karaman et al. conducted a study which saught to clarify the influence of a femoral rotational malalignment of ≥10° after intramedullary nailing on daily activities. They evaluated twenty-four femoral shaft fracture patients treated with closed antegrade IMN, and determined the presence of malrotation with post-operative CT scans. Ten of the 24 patients had a CT-detected true rotational malalignment of ≥10° compared with the unaffected side, and were noted to have significantly worse functional outcome scores compared with normally rotated femoral shaft patients.
Espinoza et al. present a technique using intraoperative fluoroscopy and the anteversion inherent to the IM nail for obtaining appropriate femoral rotational alignment during surgery. The authors state that their technique reliably sets the femoral anteversion within a normal physiologic range with minimal additional intraoperative steps and without preoperative measurements.
Illustration A shows a CT evaluation of femoral malrotation. The angle on the uninjured side measures 30°, while the malrotated fractured side measures only 3°, indicating a 27° external rotation deformity.
Incorrect Answers:
Answer 1: This would result in external rotation of the femur. Answer 2: This would result in external rotation of the femur. Answer 3: This would result in external rotation of the femur. Answer 4: The contralateral femur would not be affected in this case.
Question 10
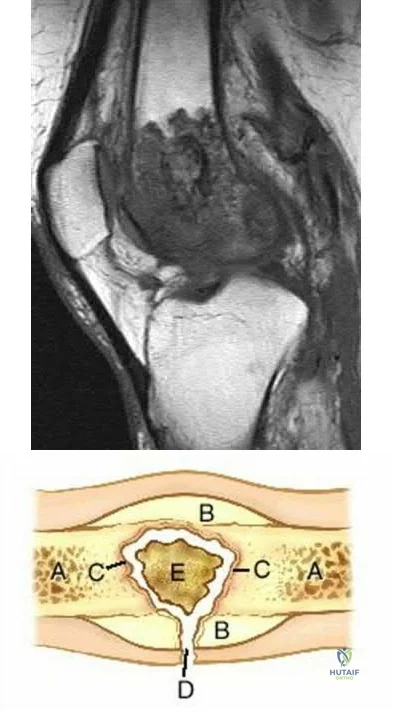
A 34-year-old man sustained a gunshot wound to the knee 18 months ago and was treated with bullet removal and a 10 day course of oral antibiotics. He now complains of 12 months duration of pain in the thigh and recent ulceration and drainage of the skin near the site of his gunshot wound. Physical exam is notable for a draining sinus tract, erythema and tenderness of the mid-thigh. He is afebrile. An MRI image of this patient is shown in Figure A. Which of the following is the most appropriate management?
Explanation
In the referenced article by Parsons and Strauss, the management of chronic osteomyelitis is reviewed.
Question 11
A 40-year-old man fell off of a ladder at work sustaining the injury shown in Figures A and B. On examination, his skin is intact, but the pulses in his foot are absent. Following closed reduction and splinting, what would be the next best step?

Explanation
With any dislocation, an immediate closed reduction should be performed. Though the initial vascular examination was abnormal in this case, the dislocation is contributing to this finding. This unique ankle fracture is known as the hyperplantarflexion variant. It is composed of a posterior tibial lip fracture with posterolateral and posteromedial fracture fragments separated by a vertical fracture line.
Gardner et al. review the hyperplantarflexion variant and found that the fracture of the posteromedial tibial rim was the main feature of this injury which is sustained by a hyperflexion mechanism. They also reported that posterior malleolus fractures are present in a majority of these injuries as well.
On MRI they determined that the deltoid and posterior tibiofibular ligaments were intact in all cases. They conclude, when treating these fractures with ORIF of the posteromedial and posterior fragments with antiglide fixation, excellent results were obtained.
Hinds et al. name the unique double cortical density at the inferomedial tibial metaphysis the "spur sign." They found the spur sign to be present in 79% of variant ankle fracture cases. They found the positive predictive value and negative predictive value to be 100% and 99%, respectively when this sign is present.
Figures A and B demonstrate the hyperplantarflexion variant ankle fracture. Illustration A demonstrates the spur sign, as indicated by the red arrow.
Incorrect Answers:
Answer 2: Vascular consultation may be obtained if the vascular exam is abnormal.
Answer 3: CT angiography may be obtained after closed reduction to aid in the diagnosis of vascular injury if the exam is abnormal after closed reduction.
Answer 4: A formal angiogram may be necessary if there is an abnormality in the vascular exam.
Answer 5: Surgical exploration and stabilization may eventually be necessary, but are not the next best step in treatment.
Question 12
What is a known risk factor for lateral distal femoral locking plate failure when used for the fixation of comminuted extra-articular fractures?

Explanation
Implant failure is common in distal femur fractures stabilized with plate fixation. Contributors to failure include a short working length of the construct, plate-screw density more than 0.5 and short plate lengths. This will lead to failure as it causes increased strain on the plate over a short segment, and
does not allow enough motion at the fracture site to form bone for healing by secondary intention.
Ricci et al. reviewed 355 cases of distal femur plate fixation. 64 patients (19%) required reoperation to promote union, including 30 that had a planned staged bone grafting. Risk factors for proximal implant failure included open fracture, smoking, increased body mass index, and shorter plate length.
Kregor et al. reviewed 119 patients with distal femoral plate fixation. They found that 93% fractures healed without acute bone grafting. Complications included 5 losses of proximal fixation, 2 nonunions, and 3 acute infections.
Illustration A is an AP of the distal femur demonstrating a comminuted distal femur fracture which has failed fixation with a laterally based distal femur locking plate. It has undergone varus collapse which is a common mechanism of failure for these injuries. Illustration B is a series of AP radiographs of the distal femur of the same patient that was revised to an intramedullary retrograde nail. Illustration C and D show the concepts of plate length, plate-to-screw density and the working length of the plate.
Incorrect Answers:
Answer 1: Early postoperative knee range of motion has not been associated with failure of this construct.
Answer 2: Early weight-bearing can put too much force across the plate, causing fatigue failure of the plate.
Answer 4: Bridge plate fixation would have been the proper technique to use in this situation.
Answer 5: Plate-screw density less than 0.5 would have been the proper technique to use in this situation. This would have helped to avoid this complication.
Question 13
A 45-year-old male presented to the trauma department 10 hours after sustaining a fracture-dislocation of his ankle. The patient underwent an attempted closed reduction of his ankle which can be seen in Figures A and B. The splint was removed, and the appearance of the leg is shown in Figure C. Regarding the best next step in management and the intended goals, which of the following is most accurate?

Explanation
Patients with high-energy periarticular fractures in the lower extremity are at risk for surgical wound complications due to compromised soft tissues. As in this case, joint dislocations can place harmful tension on the skin that leads to blistering and/or skin necrosis. An urgent reduction is indicated, and if it cannot be obtained with a closed manipulation alone, percutaneous or open treatment is indicated. Staged joint-spanning external fixation can both hold a reduction and allow access for skin or wound care prior to a definitive open reduction of an articular fracture. Fracture healing during external fixation occurs by enchondral ossification by way of the relative stability.
Strauss et al. developed a treatment protocol for the treatment of fracture blisters. They used silver sulfadine to minimize soft tissue complications by promoting re-epithelialization. After providone-iodine prep, each blister was unroofed by removing the overlying epithelium of the fracture. Once the blister was unroofed, silver sulfadiazine was applied and covered with dry gauze. They would then perform bid dressing changes. Extremities were deemed operable when skin wrinkles were visible on the overlying skin of the injured extremity.
Anglen et al. in a review of external fixation, report that fractures of the lower extremity are frequently associated with soft tissue trauma that precludes safe surgical treatment in the early period. They present a technique of temporary joint-spanning external fixation which allows stabilization of length and alignment while awaiting resolution of soft tissue swelling. They report no differences between patients who had a temporary external fixator and those who did not with respect to healing time, time to partial or full weight bearing, or clinical score.
Figures A and B demonstrate a pronation-external rotation type fracture with disruption of the syndesmosis. Figure C demonstrates fracture blisters.
Illustration A demonstrates an ankle-spanning external fixator. Illustration B demonstrates skin wrinkling to indicate that the skin is safe to incise.
Incorrect Answers:
Answer 1: This fracture pattern has already failed closed reduction, therefore another attempt would likely be unsuccessful. Furthermore, closed reduction and splinting would result in relative stability of the fracture.
Answer 2: If transarticular fixation is to be used for provisional reduction, larger caliber wires need to be used to lower the risk of wires breaking within the joint. Furthermore, this mode of fixation would result in relative stability of the fracture.
Answer 3 and 4: Definitive ORIF through a compromised soft tissue envelope is not not appropriate in the setting of hemorrhagic blisters overlying the incision sites. In ORIF, relative and absolute stability are both possible, depending on the mode utilized during fixation (i.e. relative stability is achieved when a bridge plate is utilized to span a comminuted fracture, whereas absolute stability is obtained when a lag screw and/or compression plate are utilized).
Question 14
A young male patient underwent intramedullary nail fixation for a diaphyseal femur fracture. A post-operative CT scanogram is performed to assess rotational alignment between the surgical and non-surgical femur. Which of the following measurement(s) are considered acceptable differences in regards to femoral rotational
malreduction after intramedullary nail fixation as compared to the uninjured femur?
Explanation
Normal femoral neck anteversion is approximately 11-13°, with a normal range between 5-20°. The variation within the same patients can also be up to 15° difference between limbs. Current literature has shown that this 15° difference is well tolerated by patients, including when this has occured as a result of rotational malreduction following intramedullary nail fixation for a diaphyseal femur fracture.
Ayalon et al. aimed to compare the difference in femoral version (DFV) after intramedullary nailing performed by a trauma-trained and non-trauma trained surgeon. The mean post-operative DFV was 8.7° in these patients, compared to 10.7° in those treated by surgeons of other subspecialties. Post-operative version or percentage of DFV >15° did not significantly differ between these two groups.
Omar et al. studied the utility of pre-operative 'virtual reduction' of bilateral femoral fractures that were initially stabilized with external fixation. After external fixation, the mean rotational difference between both legs was 15.0°
± 10.2°. Following virtual reduction, the mean rotational difference between both legs was 2.1° ± 1.2°, after intramedullary nailing, compared to 6.1° ±
2.8° without the pre-operative tool.
Illustration A shows the typical CT scanogram cuts used to measure femoral version. Note, femoral version is obtained by measuring an angle between a line along the femoral neck and another line along the posterior condylar axis.
Incorrect Answers:
Answers 1-5: More than 15° difference in version between femurs is considered the upper limit for acceptable reduction.
Question 15
A 72-year-old male sustains the injury shown in Figure A as a result of a fall from a ladder. Which of the following factors has been shown to be associated with increased collapse or sliding displacement?

Explanation
Palm et al showed that 22% of patients with a fractured lateral femoral wall underwent reoperation for collapse of fracture compared to 3% with an intact lateral femoral wall. Interestingly, 74% of the lateral proximal femoral wall fractures were iatrogenic during the procedure itself.
Gotfried et al reported on 24 patients with postoperative intertrochanteric hip fracture collapse and noted that this complication followed fracture of the lateral wall in every instance and resulted in a protracted period of disability until fracture healing. They recommend care when drilling at the base of the lateral wall intraoperatively.
Lindskog et al review the diagnosis, treatment, as well as biomechanical reviews of treatment options for unstable intertrochanteric hip fractures.
Incorrect Answers:
Answer 1, 2, and 3: No difference in collapse has been shown between long or short intramedullary devices and an external fixator in stable intertrochanteric hip fractures.
Answer 4: Early postoperative weightbearing is the goal after repair, and no differences have been shown in collapse rates with different weight bearing protocols.
Question 16
A 20-year old male was involved in a motor vehicle accident. He is complaining of bilateral leg pain. He has a mean arterial pressure of 80, heart rate of 90, a lactate level of 1.2 mmol/L, and base deficit of
0.5. On physical examination, he has no open wounds and is neurologically intact in both lower extremities. Imaging of the right femur (Figures A and B) and the left femur (Figures C and D) is shown. What is the next best step in treatment?

Explanation
This patient has been adequately resuscitated and should undergo definitive stabilization of his injuries. Indicators for adequate resuscitation are mean arterial pressure > 60, heart rate <100, urine output of 30 cc/hour, serum lactate of < 2.5, gastric mucosal pH > 7.3, and a base deficit of -2 to +2.
Bilateral femoral shaft fractures are a relative indication for retrograde femoral nailing. When compared to antegrade nailing of this injury pattern, retrograde nailing has a decreased operative time because the extremities may be prepped and draped together, eliminating the need to re-position and re-prep the patient.
Nork et al. performed a review of patients treated with reamed intramedullary nailing of a femoral shaft fracture. They found 54 patients with bilateral femoral shaft fractures. They report that mortality in these patients was 5.6% compared to 1.5% in the unilateral group. Bilateral fractures are also associated with a longer length of stay in the hospital and a longer length of stay in the intensive care unit. They conclude that patients with bilateral fractures sustain a higher injury burden than patients with unilateral injuries.
Pape et al. performed a study to determine whether the use of a reamer that provides simultaneous irrigation and aspiration of intramedullary contents can lower the risk of pulmonary embolization when performing a femoral nail. The experiment was performed in sheep treated with femoral nails separated into 3 groups: reamed femoral nailing, reaming with irrigation and aspiration, and unreamed nailing. They conclude that in the presence of unilateral pulmonary injury, the effects of reaming may be minimized by irrigating and aspirating the canal.
Brumback et al. wrote a review on intramedullary nailing of the femur comparing reamed and unreamed techniques. They report that reamed intramedullary nailing has not been associated increases in pulmonary complications while unreamed nailing has been shown to have slightly higher rates of delayed union and nonunion. They conclude that reamed interlocking intramedullary fixation remains the treatment of choice for femoral shaft fractures in adults.
Figures A-D are radiographs demonstrating a femoral shaft fracture. Incorrect Answers:
Answers 1 & 2: This patient is adequately resuscitated and definitive fixation
may be performed.
Answer 3: Though plate and screw fixation may be used in the treatment of femoral shaft fractures, intramedullary nailing is the preferred treatment.
Answer 4: Unreamed nailing should not be performed in adults.
Question 17
A 34-year-old male presents with elbow pain after sustaining a ground level fall 2 weeks ago. An injury radiograph is shown in Figure
A. Which of the following provocative maneuvers will most likely be positive?

Explanation
Varus posteromedial rotatory instability (VPMRI) of the elbow is caused by a varus and posteromedial rotation force, resulting in rupture of the lateral collateral ligament (LCL) from its humeral origin. The medial coronoid process is subsequently forced against the medial trochlea, which results in fracture of the anteromedial portion. The most sensitive test is the gravity-assisted varus stress test. The arm is abducted to 90° and the patient is asked to flex and extend the elbow. The test is positive for pain, grinding, or instability during range of motion, as the ulnohumeral joint is closed medially by the lack of the buttress from the anteromedial coronoid. Treatment involves surgically addressing the anteromedial facet of the coronoid and repairing the LCL.
Steinmann performed a review of coronoid process fractures. He reports that with an anteromedial coronoid fracture, the anteroposterior (AP) radiograph of the elbow will demonstrate progressive narrowing of the joint space from lateral to medial. They conclude that an important determinant of stability is the involvement of the sublime tubercle (insertion point of the MCL). When the sublime tubercle is involved, medial elbow instability is likely.
Doornberg et al. performed a retrospective review of coronoid fracture patterns. They found that large fractures of the coronoid were involved with anterior and posterior olecranon fracture/dislocations, small transverse fractures were involved with terrible triad injuries, and anteromedial facet fractures were associated with VPMRI.
Doornberg et al. performed a retrospective review of patients with fracture of the anteromedial facet of the coronoid. They report that if the fracture is not specifically treated, patients ultimately developed arthrosis. They report that the coronoid fracture may be secured with a plate, screw, or sutures. They conclude that secure fixation of the coronoid usually restores good elbow function.
Figure A is an AP radiograph of the elbow demonstrating a fracture of the anteromedial facet of the coronoid. Illustration A is a fluoroscopic stress view demonstrating ulnohumeral instability due to an associated LCL injury.
Illustration B is an AP radiograph demonstrating plate and screw fixation of the coronoid and suture anchor repair of the LCL.
Incorrect Answers:
Answer 1: The lateral pivot shift test is performed with the patient supine with the affected arm overhead. The forearm is supinated and valgus stress is applied while flexing the elbow. Subluxation constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 2: The milking maneuver is performed by creating valgus stress by pulling the patient's thumb with the forearm supinated and elbow flexed to 90°. Subluxation constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 3: The chair rise test is performed by asking the patient to push off from a seated position in a chair. Subluxation when transitioning to elbow extension constitutes a positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Answer 4: The posterior drawer test is performed with the patient in a seated position with the elbow flexed to 90°. The clinician stabilizes the humerus and gives a superior and inferior force to the forearm. Subluxation constitutes a
positive finding and is seen in valgus posterolateral rotatory instability of the elbow.
Question 18
A 32-year-old man is brought to the emergency department after being involved in an MVC. He is found to have a closed left femoral shaft fracture (Figures A and B) and a Glasgow Coma Scale (GCS) score of 13. A CT scan of the head is performed and demonstrates no significant bleeding. He has no other injuries and is hemodynamically stable. Which of the following statements is true?
Explanation
Treatment of patients with a closed head injury and a femoral fracture remains controversial but recent data suggests that intramedullary nails done acutely
leads to decreased pulmonary complications, decreased thromboembolic events, improved rehabilitation, decreased length of stay and cost of hospitalization, and improved GCS scores on discharge. However, it is important to note that intraoperative hypotension should be avoided in these patients, as it has been associated with worsening outcomes following acute intramedullary nailing of the femur.
Starr et al. performed a retrospective study to determine if the timing of treatment of femur fractures in patients with an associated head injury had an effect on the risk of pulmonary and CNS complications. They found that delaying fracture stabilization (> 24 hours) made pulmonary complications 45 times more likely, while early fracture stabilization had no effect on the risk of CNS complications.
McKee et al. performed a retrospective case-control study to determine the effect of early intramedullary nailing of femoral shaft fractures on the neurologic outcome of patients with multiple injuries and a concomitant head injury. They found no significant differences between the two groups in terms of early mortality, length of hospital/ICU stay, level of neurologic disability, or results of cognitive testing. Their results support the continued early intramedullary nailing of femoral fractures for patients with a concomitant head injury.
Richards et al. performed a retrospective study evaluating lactate levels before reamed intramedullary nailing (IMN) of femur fractures treated with early fixation (< 24 hours) and its effects on pulmonary complications (defined as mechanical ventilation lasting ≥ 5 days). They found that a median admission lactate of 3.7 mmol/L was associated with duration of mechanical ventilation ≥ 5 days, whereas a median preoperative lactate of 2.8 mmol/L was not.
Figures A and B are radiographs demonstrating a transverse femoral shaft fracture.
Incorrect Answers:
Answer 1: Early stabilization of the patient's femur fracture places him at decreased risk of pulmonary complications.
Answer 2: A concomitant head injury is not a contraindication to early fixation of the patient's femur fracture.
Answer 3: Damage control orthopaedics using external fixation is not indicated in this patient. Intramedullary nailing should be performed instead.
Answer 5: A concomitant chest injury is not a contraindication to early fixation of the patient's femur fracture.
Question 19
Which of the following pelvic injury types has the highest reported mortality rate?

Explanation
APC injuries have high rates of concomitant thoracic and abdominal visceral injuries leading to the highest rates of mortality among pelvic fractures. Lateral compression (LC) fractures have particularly high incidences of associated brain and head injury with lower mortality than APC injuries. Overall, as the grade of pelvic ring injury increases the rates of associated injuries increases, regardless of exact mechanism of injury. The overall mortality rate for any pelvic trauma is roughly 15%, with APC III mortality around 37%, and overall
APC mortality rates around 26%. LC of any grade has an estimated mortality around 13%. Vertical shear and CMI have estimated mortality of 25% and 17.1%, respectively. The lowest mortality rates are following acetabular fractures with estimates around 1.5%.
Dalal et al retrospectively reviewed 340 trauma patients with pelvic injuries to analyze organ injury, resuscitative requirements, and outcomes. They found the highest mortality rates were in APC III and that more severe APC injuries had greater organ damage and mortality. They conclude that the mechanical force type and classification of injury are predictors of organ injury pattern, resuscitation needs, and mortality.
Eastridge et al reviewed 1,014 injured pedestrians for pelvic injuries, associated injuries, and relationship of treatments to outcomes. They found the highest mortality rates were associated with APC III and LC III injuries patterns at 50%. They conclude that pelvic fractures are a sign of significant energy imparted on the body and severity of associated injuries lead to the high rates of morbidity and mortality.
Illustration A and B show an APC III and LC III injury, respectively. Incorrect Answers:
Answer 2, 3, 4, and 5: LC III, acetabular fracture, vertical shear, and combined
mechanism injuries all have lower mortality rates than APC injuries.
Question 20
Which of the following structures is at risk during proximal dissection of a single lateral perifibular approach for compartment syndrome of the leg?
Explanation
peroneal nerve as it exits the fascia of the lateral compartment and runs anteriorly in the distal third of the leg.
The referenced article by Whitesides is a review of compartment syndrome pathology, diagnosis, and treatment.
Question 21
Which of the following is an indication for surgical treatment of an acute humeral shaft fracture?
Explanation
Question 22
Which of the following patients who sustained a calcaneal fracture will most likely undergo an eventual subtalar fusion?
Explanation
The meta-analysis by Randle et al reviewed 6 clinical studies comparing the results of operative vs. conservative management of calcaneal fracture studies. They found a trend for nonoperatively treated patients to have a higher risk of experiencing severe foot pain than did operatively treated patients, however they could not draw any definitive conclusions guiding treatment.
Question 23
An 78-year-old woman who lives in a nursing home sustains an injury to her left forearm. Radiograph is shown in Figure A. It is determined that the injury occurred as the result of elder abuse. All of the following are considered risk factors for elder abuse EXCEPT?

Explanation
Risk factors include substance abuse or mental illness on the part of the abuser, dependence of the abuser on the victim, shared living arrangements, external factors causing stress, social isolation, a history of violence, increased age of victim, race, poverty, functional disability and cognitive impairment. A strong association between reported child abuse and reported elder abuses within a regional population has been reported.
The review by Chen et al states the prevalence of elder abuse is 32 cases per 1,000 persons and is increasing with the growing elderly population.
The review by Lachs states that risk factors for abuse include dementia, poor physical and emotional health, disruptive or aggressive behavior, social dysfunction and prior violence or abusive acts by the victim toward the abuser.
Question 24
Which of the following factors is associated with the highest rate of nonunion of a midshaft clavicle fracture?

Explanation
Clavicle fractures are often secondary to direct blows to the lateral aspect of the shoulder. Physical examination is important to ascertain the status of the
skin and neurovascular structures to help guide treatment management. Although most non-displaced middle 1/3 clavicle fractures may be treated successfully with conservative measures, the risk for non-union (1-5%) increases with increasing comminution, female gender, shortening greater than 2 cm and an advanced age of the patient.
Robinson et al. reviewed 581 patients treated non-operatively for midshaft clavicle fractures. A nonunion rate of 4.5 % was identified at 24 weeks after the injury. They identified four factors that contributed to non-union, including: female gender, lack of cortical apposition, comminution of the fracture fragments and advancing age.
Zlowdzki et al. reviewed 2144 clavicle fracture cases in a comprehensive meta-analysis. They report displacement as the highest risk factor for nonunion (15.1%) in nonoperatively treated clavicle fractures, and simple slings were favored over figure of 8 braces. They also report an 86% reduction in the nonunion rate when operative fixation is chosen over nonoperative treatment for displaced clavicle fractures.
Illustration A shows the presence of a non-union of a midshaft clavicle fracture. A video is provided that reviews management of clavicle injuries.
Incorrect Answers
Answers 1, 3: Older patients and comminution of the fracture were found to be risk factors for non-union in midshaft clavicle injuries
Answers 4, 5: Neither of these are associated with an increased risk of nonunion in midshaft clavicular fractures.
Question 25
You are planning operative treatment of the injury shown in figure A. If the MCL is intact, in what position should the elbow and
forearm be splinted at the end of the case?

Explanation
Neale et al (Presentation at the 23rd Annual Meeting of the American Society of Biomechanics, University of Pittsburgh; October 21-23, 1999) showed that the coronoid is clearly a primary stabilizer of the elbow, with the radial head being a secondary stabilizer. When the elbow was slowly brought into extension to find the point at which it becomes unstable, the degree of flexion needed to maintain stability was greater with progessive loss of coronoid and with loss of the radial head. Therefore, the elbow is more stable in flexion due to the support provided by the coronoid and radial head.
Dunning et al investigated the contribution of forearm position to the stability of a lateral collateral ligament deficient elbow. They determined that varus and valgus laxity was significantly less with the forearm in pronation than in supination. They speculated that the internal rotation torque applied to the
wrist to maintain the forearm in pronation may cause the ulna to pivot about the intact soft tissues on the medial side of the elbow and close the gap on the lateral side. The most stable position is flexion with forearm pronation.
If both the MCL and LCL are repaired, newer recommendations from Mathew et al. are for splinting in flexion and neutral rotation.
Question 26
A 32-year-old male sustains a closed head injury, a closed pelvic ring injury, as well as the bilateral open femoral fractures shown in Figures A-C. He remains borderline hypotensive with a base deficit of
4.9 after an exploratory laparatomy and splenectomy. After irrigation and debridement of his open fractures, what is the most appropriate treatment for this patient at this time?

Explanation
The referenced article by Scalea et al found that external fixation for femur fractures is a viable alternative to attain temporary rigid stabilization in patients with multiple injuries.
Question 27
A 35-year-old male has a closed mid-shaft tibia fracture following a skiing accident. You have recommended intramedullary nailing of the tibia. What is the most common complication he must be advised about?
Explanation
(77% and 50% respectively). Toivanen et al. investigated this question when the group randomized fifty patients with a tibial shaft fracture requiring intramedullary nailing equally to treatment with paratendinous or transtendinous nailing. Fourteen (67%) of the twenty-one patients treated with transtendinous nailing reported anterior knee pain at the final evaluation. Of these fourteen patients, thirteen were mildly to severely impaired by the pain. Fifteen (71%) of the twenty-one patients treated with paratendinous nailing reported anterior knee pain, and ten of the fifteen were impaired by the pain.
The Lysholm, Tegner, and Iowa knee scoring systems; muscle-strength measurements; and functional tests showed no significant differences between the two groups. Compared with a transpatellar tendon approach, a paratendinous approach for nail insertion does not reduce the prevalence of chronic anterior knee pain or functional impairment by a clinically relevant amount after intramedullary nailing of a tibial shaft fracture.
Question 28
A polytrauma patient sustains a right bicondylar tibial plateau fracture and a right humeral shaft fracture both treated with open reduction and internal fixation. He also underwent statically locked intramedullary nailing of a left femoral shaft fracture. What is the appropriate weightbearing status?
Explanation
Tingstad et al found favorable results of immediate weightbearing on humeral shaft fractures treated with plating and full weightbearing did not have any effect on the union or malunion rates.
Brumback et al evaluated the feasibility, safety and efficacy of immediate
weightbearing after treatment of femoral shaft fractures with statically locked IM nail. All the patients went on to union and no loss of fixation occurred.
Question 29
A 25-year-old male is a driver in a motor vehicle accident and sustains the isolated closed injury seen in Figures A and B. He is treated with an intramedullary nail, and postoperative radiographs are shown in Figures C and D. Which of the statements concerning reaming and nails is true?

Explanation
In 1998, Hupel et al studied the effect of loose and tight unreamed, locked nails on cortical blood flow and strength of union in a canine model. They found that loose nails allowed higher cortical reperfusion at the time of insertion and at eleven weeks.
In a later study by the same group in 2001, they studied the effect of non-reamed, limited reamed and standard reamed nails on porosity, new bone formation and mineral apposition. They found the lowest porosity in the limited reaming group but found new bone formation and mineral apposition rates similar at eleven weeks across the three groups. They concluded that limited reaming is preferred in patients with vascular compromise to the tibia.
Incorrect Answers:
1: Reamed and unreamed tibias have similar mineral apposition rates. 2: Reamed tibias have the highest amount of new bone formation.
3: The lowest porosity of bone is seen with limited reaming.
5: Nails that are tight to the cortex have less reperfusion than appropriately fitting or loose nails.
Question 30
A 42-year-old man reports persistent arm pain after undergoing intramedullary nailing of a humeral shaft fracture 13 months ago.
Physical exam shows near normal shoulder and elbow range-of-motion. Infection work-up is normal. A radiograph is shown in Figure
A. What is the next most appropriate step in treatment?

Explanation
Rubel et al in a combined cadaveric and clinical study comparing one versus two plate constructs for humeral nonunions found that the two plate construct was significantly stiffer, but had no difference in healing rate compared with a single plate construct; 92% of the humeral shaft nonunion patients went onto union with rigid plate fixation.
Ring et al successfully treated a cohort of osteoporotic humeral shaft nonunions with locked plating. They
report 100% union rate with locking plate fixation of these humeral shaft nonunions, with use of autograft in >50% of their cases. Subjective shoulder scores were excellent or good in 22 of 24 patients.
Brinker and O'Connor analyzed the current available evidence for exchange nailing of nonunions and could not recommend this treatment for humeral shaft nonunions.
Question 31
When comparing the fibular plating techniques shown in Figures A and B, the plate position shown in Figure B is associated with which of the following?

Explanation
Figure A shows an antiglide (posterior) plating of the distal fibula, while Figure B shows a lateral neutralization plating of the distal fibula. Both methods are acceptable, but posterior antiglide plating is associated with increased construct stiffness and strength, decreased hardware prominence, decreased rates of ankle joint screw penetration, and improved biomechanical findings in osteoporotic bone. However, posterior plating is associated with an increased rate of peroneal tendonitis and irritation. Illustration A shows a lateral radiograph of a posterior fibular plate.
The referenced article by Ostrum et al is a case series of 32 patients who had antiglide plating; he reported a 100% union rate, 95% patient satisfaction rate, and only 4/32 reported peroneal tendinitis, with all resolving by 2
months.
The other referenced article by Schaffer et al reported that the posterolateral antiglide plate demonstrated improved biomechanical stability as compared to the lateral plating, with increased construct stiffness and load to failure.
Question 32
A 32-year-old man sustains a pilon fracture which is treated initially with a spanning external fixator, as shown in figure A. He is now 3 weeks from injury and skin swelling has subsided significantly. What is the most appropriate definitive treatment?

Explanation
Question 33
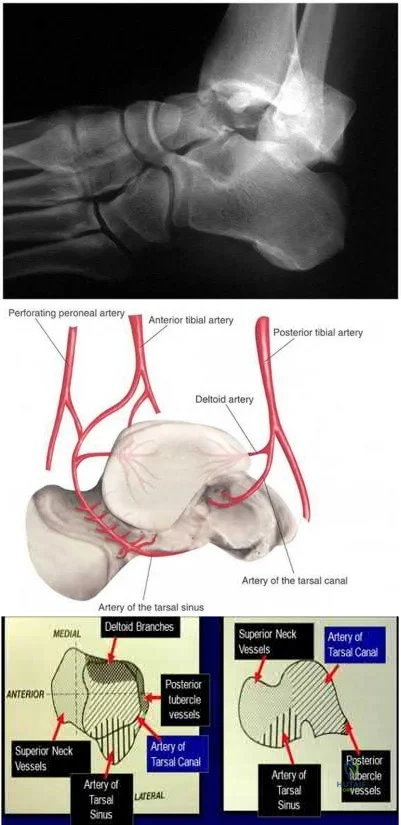
A 29-year-old male sustains the isolated lower extremity injury shown in Figure A. During open reduction, what structure must be kept intact in order to protect the remaining blood supply to the talar body?
Explanation
The review article by Fortin et al discusses talar blood supply, injury mechanisms and classifications, and treatment options. They state that the main artery to the body of the talus is the artery of the tarsal canal, which is a branch of the posterior tibial artery. The peroneal and anterior tibial artery also contribute branches to the talus.
Illustration A and B show the arterial network of the talus.
Question 34
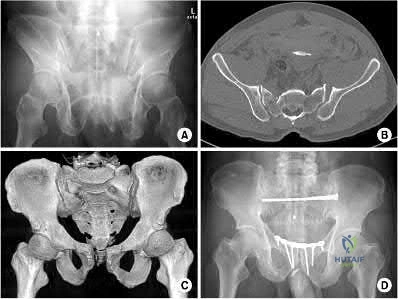
Based on the Young and Burgess classification of pelvic ring injuries, an anterior-posterior compression type II injury does not result in disruption of which of the following?
Explanation
Young and Burgess classification of pelvic ring injuries is largely based on the mechanism and energy of injury. An APC type I involves slight widening of
pubic symphysis and/or anterior sacroiliac (SI) joint. An APC II is a continuation of this force, and additionally involves a disrupted anterior SI joint, as well as sacrotuberous and sacrospinous ligaments. An APC III also involves disrupted posterior SI ligaments, causing complete SI joint disruption with potential translational and rotational displacement.
The reference by Young et al is a classic article that describes the Young and Burgess classification of pelvic ring injuries. They retrospectively analyzed pelvic ring radiographs and discussed four patterns of injury: anteroposterior compression, lateral compression, vertical shear, and a complex/combined pattern.
The reference by Burgess et al is a validation of the aforementioned classification and study, as they reviewed 210 consecutive patients who sustained a pelvic ring injury. They validated the classification scheme and found that overall blood replacement averaged: lateral compression, 3.6 units; anteroposterior compression, 14.8 units; vertical shear, 9.2 units; combined mechanical, 8.5 units. Overall mortality was: lateral compression, 7.0%; anteroposterior, 20.0%, vertical shear, 0%; combined mechanical, 18.0%.
Illustration A shows an APC-II injury pattern - (a) is an outlet radiograph, (b) is an axial CT cut, (c) is a 3-D CT cut, and (d) is a representative fixation construct.
Incorrect answers:
1,2,4,5: An APC - 2 pelvic ring injury involves injury to all of these structures.
Question 35
A 25-year-old male involved in a motor vehicle accident sustains multiple injuries. He undergoes operative treatment for his humeral shaft fracture. Figures A and B show his preoperative and postoperative radiographs. The distal interlocks for this implant place which of the following nerves at risk?

Explanation
Rupp et al performed a cadaveric study with IM nails utilizing either lateral-to-medial or anterior-to-posterior distal interlocking screws. They showed that anterior-to-posterior screws placed the musculocutaneous nerve at high risk, while lateral-to-medial screws placed the radial nerve at high risk as it courses laterally distally along the humerus.
Question 36
A 25-year-old male sustains a humeral shaft fracture and is treated with the implant seen in Figure A. Compared with open reduction and internal fixation with a plate and screw construct, the treatment shown in Figure A is associated with all of the following EXCEPT?

Explanation
It is important to note that the answer to this question continues to evolve as more data and studies are performed.
McCormack prosepectively randomized 44 humeral shaft fractures to treatment by intramedullary nailing vs. dynamic compression (DCP) plating and found the risk of shoulder impingement, iatrogenic comminution, and nonunion were higher in the nail treatment group resulting in a higher revision rate. They found no significant differences in shoulder/elbow function, VAS pain scores, ROM, or time to return to normal activity.
Chapman et al in their prospective randomized trial between IMN and plate fixation found that the IMN group had higher rates of post operative shoulder pain and a slower time to fracture union. The ORIF had faster time to union, but reduced elbow range of motion. Both studies show the effectiveness of IMN and ORIF in the treatment of humeral shaft fractures.
More recent meta-analysis such as by Ma et al show that both IMN and DCP can achieve similar fracture union with a similar incidence of radial nerve injury and infection. IMN was associated with an increased risk of shoulder impingement, more restriction of shoulder movement, an increased risk of intraoperative fracture comminution, a higher incidence of implant failure, and an increased risk of re-operation.
Question 37
A 69-year-old female sustains the injuries seen in Figures A and
B. This injury is best classified as which of the following?

Explanation
The referenced article by Bennett et al reviews the associated soft tissue injury with tibial plateau fractures. They found a 56% frequency of associated soft tissue injuries overall, with MCL injured in 20%, the LCL in 3% , the menisci in 20%, the peroneal nerve in 3%, and the anterior cruciate ligaments in 10%.
Schatzker type IV and type II fracture patterns were associated with the highest frequency of soft tissue injuries.
Question 38
A 25-year-old polytraumatized male is intubated and sedated. He has a closed tibial shaft fracture. Which of the following pressure measurements is an absolute indication for a four-compartment fasciotomy?
Explanation
Question 39
A 30-year-old farmer sustains an open tibial shaft fracture heavily contaminated with soil and manure. Which of the following intravenous antibiotic regimens is most appropriate for initial management?
Explanation
Question 40
A 40-year-old male presents with bilateral femoral shaft fractures and a severe head injury (GCS 6) following a motor vehicle collision. His serum lactate is 4.5 mmol/L. What is the most appropriate initial management of his femoral fractures?
Explanation
Question 41
What is the maximum acceptable coronal plane deformity (varus/valgus) when treating a closed tibial shaft fracture non-operatively in a long leg cast?
Explanation
Question 42
A 75-year-old female taking alendronate for 10 years presents with insidious onset thigh pain. Radiographs reveal a transverse radiolucent line with lateral cortical thickening in the subtrochanteric femur. What is the primary mechanism leading to this injury?
Explanation
Question 43
A 45-year-old male is struck by a vehicle, sustaining a closed pelvic ring injury. Examination reveals a large, fluctuant swelling over the greater trochanter with overlying skin bruising and necrosis. What is the most likely diagnosis?
Explanation
Question 44
A 28-year-old motorcyclist sustains a distal femur fracture. Radiographs and CT scan show a coronal plane fracture of the lateral femoral condyle. What is the standard classification and recommended fixation for this specific fragment?
Explanation
Question 45
A 22-year-old male sustains a low-velocity gunshot wound to the thigh. Radiographs show a minimally displaced midshaft femur fracture. The bullet passed through the thigh and exited. There are no hard signs of vascular injury. What is the most appropriate management?
Explanation
Question 46
Which of the following is a classic triad associated with Fat Embolism Syndrome (FES)?
Explanation
Question 47
A 32-year-old male presents with a displaced, vertically oriented Pauwels type III femoral neck fracture. Which of the following fixation constructs provides the most biomechanically stable construct for this fracture pattern?
Explanation
Question 48
A 35-year-old male undergoes intramedullary nailing for a proximal third tibial shaft fracture. Post-operatively, a significant apex-anterior (procurvatum) deformity is noted. Which technique could have been used to prevent this deformity during the procedure?
Explanation
Question 49
A hemodynamically unstable patient with an anterior-posterior compression (APC-III) pelvic ring injury requires emergent pelvic binder application. What is the correct anatomical landmark for positioning the binder?
Explanation
Question 50
A 40-year-old female presents with a distal third spiral fracture of the tibial shaft. Which of the following associated injuries MUST be ruled out with advanced imaging or careful radiographic scrutiny?
Explanation
Question 51
According to Godina's classic principles, what is the optimal timeframe for performing free tissue transfer to cover a severe open tibial fracture (Gustilo IIIB) to minimize infection and maximize flap survival?
Explanation
Question 52
An 18-year-old male presents with a severely mangled lower extremity following a motorcycle accident. Which of the following is considered an absolute indication for primary amputation?
Explanation
Question 53
A 28-year-old polytrauma patient with a severe bilateral femur fracture presents to the emergency department. Which of the following laboratory values is the best indicator to proceed with Damage Control Orthopedics (DCO) rather than Early Total Care (ETC)?
Explanation
Question 54
A 35-year-old male sustains a Gustilo-Anderson Type IIIB open tibia fracture following a motorcycle collision. What is the most critical factor in reducing the patient's risk of deep infection?
Explanation
Question 55
A 25-year-old male presents with a vertically oriented, displaced femoral neck fracture (Pauwels Type III). What fixation construct provides the most biomechanical stability for this high-shear fracture pattern?
Explanation
Question 56
In a hemodynamically unstable patient with a suspected anteroposterior compression (APC) pelvic ring injury, what is the correct anatomic landmark for the optimal placement of a circumferential pelvic binder?
Explanation
Question 57
During an ilioinguinal approach for an anterior column acetabular fracture, significant hemorrhage occurs while dissecting the posterior aspect of the superior pubic ramus. Which of the following vascular anastomoses is most likely injured?
Explanation
Question 58
A 42-year-old male sustains a severe intra-articular distal femur fracture (OTA 33-C3). CT imaging reveals a distinct coronal plane fracture of the lateral femoral condyle. What is the optimal surgical approach to directly visualize and reduce this specific fragment?
Explanation
Question 59
A 30-year-old male with a closed tibial shaft fracture complains of pain out of proportion to the injury. Compartment pressure monitoring reveals an absolute anterior compartment pressure of 45 mmHg. His diastolic blood pressure is 65 mmHg. What is the most appropriate next step?
Explanation
Question 60
A 45-year-old diabetic male sustains a high-energy closed pilon fracture with severe soft tissue swelling and prominent fracture blisters over the medial ankle. What is the most appropriate initial management?
Explanation
Question 61
During surgical approach for a displaced intra-articular calcaneus fracture, care must be taken to avoid a specific tendon that runs directly inferior to the sustentaculum tali. Which tendon is this?
Explanation
Question 62
A 32-year-old female sustains a talar neck fracture. Six weeks post-operatively, a subchondral radiolucent line is visible in the talar dome on the AP ankle radiograph. What does this radiographic finding indicate?
Explanation
Question 63
A 24-year-old athlete sustains a midfoot injury. Weight-bearing radiographs show a 3 mm diastasis between the base of the first and second metatarsals. What is the most appropriate definitive management?
Explanation
Question 64
A 22-year-old male with bilateral femur fractures develops acute confusion, a petechial rash over the axilla and thorax, and hypoxia 36 hours after his injury. What is the most likely diagnosis?
Explanation
Question 65
A 72-year-old female on long-term alendronate therapy presents with progressively worsening anterior thigh pain. Radiographs reveal a localized periosteal reaction and a transverse radiolucent line on the lateral cortex of her subtrochanteric femur. What is the recommended management?
Explanation
Question 66
A 30-year-old male sustains a low-velocity gunshot wound to the thigh resulting in a comminuted midshaft femur fracture. The bullet remains lodged in the vastus lateralis. He has normal distal pulses and a normal neurologic exam. What is the standard of care for the soft tissue injury?
Explanation
Question 67
According to the classic principles described by Godina for lower extremity open fractures, within what optimal timeframe should definitive soft tissue coverage be performed to minimize infection and flap failure?
Explanation
Question 68
An 80-year-old male on warfarin for atrial fibrillation sustains a displaced femoral neck fracture. His admission INR is 3.5. To minimize mortality and morbidity, what is the most appropriate sequence of management?
Explanation
Question 69
A 40-year-old female presents with a posteromedial shear fracture of the tibial plateau. What surgical approach provides the most direct and optimal access for buttress plating of this specific fragment?
Explanation
Question 70
A 45-year-old male presents with a painful midshaft tibia 8 months after cast treatment for a closed fracture. Radiographs show a fracture line with abundant, bridging callus that fails to cross the fracture site (elephant shoe appearance). What is the underlying cause and preferred treatment?
Explanation
Question 71
When evaluating a severely injured lower extremity to determine the appropriateness of amputation versus salvage, the Mangled Extremity Severity Score (MESS) is often referenced. Which of the following is NOT a variable included in the MESS?
Explanation
Question 72
A 35-year-old male sustains a closed transverse fracture of the middle third of the humerus. On physical exam in the emergency department, he is unable to actively extend his wrist or digits. What is the most appropriate initial management?
Explanation
Question 73
A 25-year-old polytrauma patient is intubated in the ICU with a closed tibial shaft fracture. His blood pressure is 90/60 mmHg. His leg is tense and swollen. Which compartment pressure measurement definitively confirms the diagnosis of acute compartment syndrome in this hypotensive patient?
Explanation
Question 74
A 28-year-old male with a severe traumatic brain injury (GCS 6) and an isolated closed femoral shaft fracture is brought to the emergency department. His intracranial pressure (ICP) is being continuously monitored and is consistently measuring 28 mmHg despite maximal medical therapy. What is the most appropriate initial orthopedic management of his femoral shaft fracture?
Explanation
Question 75
A 35-year-old obtunded polytrauma patient is admitted to the intensive care unit after sustaining a closed tibial shaft fracture. Due to the patient's altered mental status, continuous intracompartmental pressure monitoring is initiated. Which of the following pressure thresholds is the most reliable indicator for performing a four-compartment leg fasciotomy?
Explanation
Question 76
Which of the following physiologic parameters is the most reliable indicator of adequate systemic resuscitation, allowing safe progression from temporary damage control external fixation to definitive intramedullary nailing in a polytrauma patient?
Explanation
None
