Orthopedic Trauma Review | Dr Hutaif Trauma & Fractures -...

Key Takeaway
This topic focuses on ORTHOPEDIC MCQS ONLINE 015 TRAUMA, Internal fixation (ORIF) for displaced femoral neck fractures in older patients carries a high risk of osteonecrosis due to compromised femoral head blood supply. Consequently, arthroplasty (hemiarthroplasty or total hip arthroplasty) is often preferred as primary treatment, especially for older, active individuals with higher functional demands, to avoid complications and potential multiple procedures associated with internal fixation orif.
Orthopedic Trauma Review | Dr Hutaif Trauma & Fractures -...
Comprehensive 100-Question Exam
00:00
Start Quiz
Question 1
A 25-year-old male sustains a severe open tibia fracture with extensive soft tissue stripping (Gustilo-Anderson IIIB) after a motorcycle collision.
What is the most critical factor in reducing the risk of deep infection in this patient?

Explanation
Question 2
A 40-year-old male is brought to the trauma bay after a severe motor vehicle crash. He is hemodynamically unstable with a blood pressure of 80/50 mmHg. Radiographs show an anteroposterior compression (APC-III) pelvic ring injury.
A circumferential pelvic binder is indicated. What is the most appropriate anatomical landmark for the correct placement of the pelvic binder?
Explanation
Question 3
A 28-year-old male sustains a vertically oriented (Pauwels type III) femoral neck fracture. What fixation construct provides the most biomechanically stable fixation to resist the high shear forces associated with this fracture pattern?
Explanation
Question 4
A 32-year-old male presents with a closed midshaft tibia fracture treated with closed reduction and casting. Twelve hours later, he complains of severe pain out of proportion to the injury. Which of the following is the most sensitive early clinical sign of acute compartment syndrome?
Explanation
Question 5
A 55-year-old female sustains a volar Barton's fracture of the distal radius. Which of the following carpal bones is most likely to subluxate volarly along with the fracture fragment?
Explanation
Question 6
A 45-year-old male sustains a coronal plane fracture of the lateral femoral condyle (Hoffa fracture) after a high-speed collision. Which of the following is true regarding the characteristics and management of this injury?
Explanation
Question 7
Which of the following scenarios is considered an absolute indication for the operative treatment of an acute midshaft clavicle fracture?
Explanation
Question 8
A 22-year-old male falls on an outstretched hand and sustains a fracture of the proximal pole of the scaphoid.
He undergoes percutaneous fixation. What is the primary arterial supply to the proximal pole of the scaphoid that places it at high risk for avascular necrosis?

Explanation
Question 9
A 60-year-old female sustains a Schatzker type II tibial plateau fracture. During surgical fixation, elevation of the depressed lateral articular fragment is performed, leaving a large metaphyseal void.
What is the most appropriate intraoperative step to address this void?

Explanation
Question 10
A 35-year-old male sustains a high-energy acetabular fracture.
Imaging reveals involvement of both the anterior and posterior columns. Crucially, no portion of the articular surface remains attached to the intact axial skeleton (ilium). What is the correct Judet-Letournel classification for this fracture pattern?

Explanation
Question 11
A 29-year-old snowboarder sustains a Hawkins type III fracture of the talar neck.
On follow-up radiographs taken 6-8 weeks post-injury, a subchondral radiolucent band is noted in the talar dome (Hawkins sign). What does this radiographic finding indicate?

Explanation
Question 12
A 40-year-old female falls from a height and sustains a 'terrible triad' injury of the elbow.
This complex injury pattern is associated with profound instability. Which of the following defines the three components of the terrible triad of the elbow?

Explanation
Question 13
A 35-year-old male sustains a pronation-external rotation (Weber C) ankle fracture.
Intraoperatively, after rigid internal fixation of the fibula, the surgeon performs a 'Cotton test' by applying a lateral pull on the fibula using a bone hook. What ligamentous structure is primarily being assessed for integrity?

Explanation
Question 14
A 45-year-old roofer falls 15 feet, landing on his heels, and sustains bilateral intra-articular calcaneus fractures.
Which of the following radiographic angles is characteristically decreased, flattened, or inverted in this injury pattern due to posterior facet collapse?

Explanation
Question 15
A 50-year-old male presents with a high-energy closed pilon fracture. Clinical examination reveals severe soft tissue swelling and the presence of fracture blisters around the ankle.
What is the most appropriate initial management for this injury?

Explanation
Question 16
A 25-year-old male is involved in a motor vehicle crash and sustains an isolated, closed midshaft femur fracture. He is resuscitated in the trauma bay and is hemodynamically stable.
What is the optimal timing for intramedullary nailing of his femur to minimize the risk of pulmonary complications (such as ARDS)?

Explanation
Question 17
A 6-year-old boy falls off the monkey bars and sustains a widely displaced, extension-type supracondylar humerus fracture.
On examination, the hand is pink and capillary refill is normal, but the radial pulse is absent. What is the most appropriate next step in management?

Explanation
Question 18
A 30-year-old male football player sustains a hyperplantarflexion injury to his midfoot. Radiographs demonstrate widening of the space between the medial cuneiform and the second metatarsal base.
This finding signifies a disruption of the Lisfranc ligament. The Lisfranc ligament anatomically connects which two osseous structures?

Explanation
Question 19
A 65-year-old female sustains a displaced 4-part proximal humerus fracture.
Recent anatomical studies (e.g., Hettrich et al.) have redefined the primary blood supply to the humeral head. Based on current evidence, which artery provides the predominant blood supply to the humeral head, placing it at risk for avascular necrosis?

Explanation
Question 20
A 50-year-old male is undergoing open reduction and internal fixation of an anterior column acetabular fracture via the ilioinguinal approach.
During dissection over the superior pubic ramus, the surgeon encounters significant bleeding. Which of the following vascular anastomoses (often termed the 'Corona Mortis') is classically located in this region and at risk of iatrogenic injury?
Explanation
Question 21
A 28-year-old polytrauma patient presents with bilateral femoral shaft fractures and a severe pulmonary contusion. His admission lactate is 4.5 mmol/L, base deficit is 8 mEq/L, and he is hemodynamically transiently responsive to fluids. According to the principles of Damage Control Orthopedics (DCO), what is the most appropriate initial management of his femoral fractures?
Explanation
Question 22
A 35-year-old construction worker falls from a scaffolding. Pelvic radiographs are obtained, and the obturator oblique view demonstrates a pathognomonic "spur sign." What acetabular fracture pattern does this sign indicate?
Explanation
Question 23
A 24-year-old male undergoes reamed intramedullary nailing for a closed midshaft tibia fracture. Four hours postoperatively, he complains of escalating leg pain out of proportion to the injury. His blood pressure is 110/65 mmHg. Intracompartmental pressure testing reveals an anterior compartment pressure of 40 mmHg. What is the most appropriate next step in management?
Explanation
Question 24
A 45-year-old female sustains a high-energy supracondylar femur fracture. Computed tomography reveals a displaced coronal shear fracture of the lateral femoral condyle (Hoffa fragment).
What is the most biomechanically sound fixation strategy for this specific fragment?
Explanation
Question 25
A 32-year-old male is involved in a severe motor vehicle accident and sustains a displaced fracture of the talar neck with subtalar and tibiotalar dislocation (Hawkins Type III). Which of the following vessels provides the predominant blood supply to the talar body and is at greatest risk in this injury?
Explanation
Question 26
A 22-year-old motorcyclist is thrown from his bike. He presents with massive swelling over the left shoulder, an absent radial pulse, and complete paralysis of the left upper extremity. Chest radiograph demonstrates a widely displaced clavicle fracture with severe lateral displacement of the scapula. What is the most appropriate next step after stabilizing his airway and breathing?
Explanation
Question 27
A 50-year-old male sustains a Gustilo-Anderson IIIB open fracture of the proximal third of the tibia. After aggressive serial debridements, a 6 cm x 4 cm anterior soft tissue defect exposes the bare bone and the proximal tibial plate. What is the most appropriate soft tissue coverage option?
Explanation
Question 28
An 82-year-old female presents with a displaced intertrochanteric femur fracture. She has a history of coronary stents placed 2 years ago and takes clopidogrel (Plavix) daily. According to current AAOS guidelines, what is the safest and most effective approach regarding the timing of her surgery?
Explanation
Question 29
A 40-year-old male arrives in the trauma bay hypotensive and tachycardic. Radiographs confirm an anteroposterior compression type III (APC-III) pelvic ring injury. After application of a circumferential pelvic binder and transfusion of 2 units of packed red blood cells, his blood pressure remains 75/40 mmHg. A FAST examination is negative. What is the most appropriate next step in management?
Explanation
Question 30
A 35-year-old female falls onto a fully extended knee. Radiographs reveal a depressed, split fracture of the medial tibial plateau.
What is the classic mechanism of injury for this Schatzker IV fracture, and what surgical approach is typically required?
Explanation
Question 31
A 26-year-old male presents with a closed, transverse fracture of the middle third of the humeral shaft following an arm wrestling match. Physical examination reveals an inability to extend the wrist and fingers, with numbness in the first dorsal web space, which was present immediately after the injury. What is the most appropriate initial management of this neurologic deficit?
Explanation
Question 32
A 30-year-old football player sustains an axial load to a plantarflexed foot. Weight-bearing radiographs show widening between the first and second metatarsals, and a small bony avulsion is noted in the intercuneiform space (the "fleck sign"). The Lisfranc ligament, responsible for this sign, connects which two anatomical structures?
Explanation
Question 33
A 14-month-old non-ambulatory child is brought to the emergency department crying with a swollen right thigh. Radiographs demonstrate a displaced spiral fracture of the femoral shaft. The parents state the child caught his leg in the crib slats. What is the most appropriate next step in management?
Explanation
Question 34
A 55-year-old female was treated non-operatively with a cast for a non-displaced Colles fracture. Six weeks post-injury, she returns to the clinic reporting a sudden, painless inability to extend the interphalangeal joint of her thumb. What is the most likely etiology of her new deficit?
Explanation
Question 35
A 68-year-old female on alendronate for 12 years presents with a low-energy transverse subtrochanteric fracture of the right femur with lateral cortical "beaking." She complains of 3 months of aching pain in her left thigh as well. Radiographs of the left femur show lateral cortical thickening but no complete fracture. What is the recommended management for the left femur?
Explanation
Question 36
A 45-year-old male sustains a displaced intra-articular calcaneus fracture (Sanders type III). Surgical fixation via an extensile lateral approach is planned. Which of the following patient factors is the most significant independent predictor for postoperative wound necrosis and deep infection?
Explanation
Question 37
A 38-year-old male presents with a severely displaced, comminuted distal tibia fracture (pilon fracture) extending into the tibiotalar joint. The ankle is massively swollen with multiple hemorrhagic fracture blisters. What is the most appropriate initial surgical management?
Explanation
Question 38
A 25-year-old hemodynamically stable male sustains an ipsilateral midshaft femur and midshaft tibia fracture ("floating knee") in a motorcycle collision. Assuming both fractures are amenable to intramedullary nailing, what is the most widely accepted sequence of operative fixation?
Explanation
Question 39
A 75-year-old female presents with a periprosthetic femur fracture around a cemented, polished taper-slip femoral stem sustained after a mechanical fall. Radiographs demonstrate that the fracture extends distal to the lesser trochanter but remains proximal to the tip of the stem. The stem is radiographically loose. According to the Vancouver classification, what is the most appropriate definitive management?
Explanation
Question 40
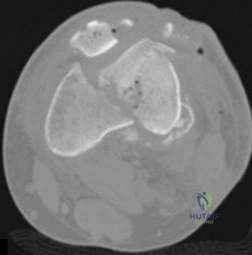
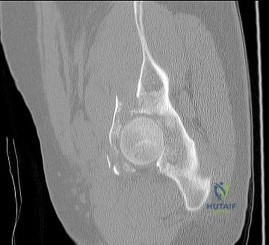
A 45-year-old male is struck by a vehicle and sustains the injury shown in the reference radiograph.
The imaging confirms a highly depressed, isolated medial tibial plateau fracture (Schatzker IV) with a varus deformity. Which of the following surgical approaches and fixation strategies is most appropriate?
Explanation
Question 41
A 24-year-old male falls onto an outstretched hand, sustaining a proximal pole scaphoid fracture. The high risk of avascular necrosis (AVN) in this fracture pattern is directly related to the retrograde blood supply of the scaphoid. The primary arterial supply to the proximal pole enters at which of the following anatomical locations?
Explanation
Question 42
A 68-year-old female sustains a 4-part proximal humerus fracture. Recent quantitative anatomic studies regarding the arterial supply to the humeral head indicate that which vessel is responsible for providing the majority of the blood supply to the articular segment?
Explanation
Question 43
A 32-year-old gymnast falls from a height and sustains a 'terrible triad' injury of the elbow. Operative intervention is planned. To properly restore elbow stability in a step-wise fashion, what is the accepted standard sequence of surgical repair?
Explanation
Question 44
A 22-year-old male undergoes open reduction and intramedullary nailing for a closed tibial shaft fracture. In the recovery room, he complains of unremitting leg pain out of proportion to the injury. Which of the following defines the critical 'Delta P' threshold used to diagnose acute compartment syndrome?
Explanation
Question 45
A 40-year-old male sustains a severe subtrochanteric femur fracture. Preoperative radiographs demonstrate the classic deformity of the proximal fracture fragment, which is flexed, abducted, and externally rotated. Which muscle is primarily responsible for the flexion deformity of the proximal segment?
Explanation
Question 46
A 35-year-old female is diagnosed with a displaced transverse acetabular fracture after a rollover motor vehicle collision. On physical examination, a large, fluctuant, ecchymotic mass is palpated over the ipsilateral greater trochanter. What is the most appropriate management of this soft tissue lesion in the context of planned surgical fixation?
Explanation
Question 47
A patient with a talar neck fracture demonstrates a subchondral radiolucent band in the talar dome on a radiograph at 6 weeks (Hawkins sign). What does this finding indicate?
Explanation
Question 48
A 45-year-old female presents with an acetabular fracture after a motor vehicle collision. Computed tomography imaging reveals a fracture extending through the anterior column and the posterior hemitransverse. What is the classic surgical approach for this specific Letournel pattern?
Explanation
Question 49
A 28-year-old male with multiple injuries has a severely comminuted femur fracture, bilateral pulmonary contusions, and a lactate of 4.5 mmol/L. What is the most appropriate initial management of the femur fracture?
Explanation
Question 50
A 35-year-old male sustains a closed tibial plateau fracture. Six hours later, he develops severe pain out of proportion to the injury. Which of the following is the most sensitive early clinical finding of acute compartment syndrome?
Explanation
Question 51
A 40-year-old male sustains a high-energy trauma resulting in a coronal plane fracture of the lateral femoral condyle (Hoffa fracture). According to biomechanical studies, what is the optimal trajectory for screw fixation to achieve maximum stability?
Explanation
Question 52
A 22-year-old cyclist falls onto his shoulder, sustaining a completely displaced, shortened (>2 cm) midshaft clavicle fracture. Compared to nonoperative management, what is the primary advantage of open reduction and internal fixation (ORIF) for this specific fracture pattern?
Explanation
Question 53
A 72-year-old female sustains a 4-part proximal humerus fracture. She has a history of severe osteoporosis and osteoarthritis of the glenohumeral joint. Which of the following is the most appropriate surgical treatment?
Explanation
Question 54
Following intramedullary nailing of a proximal third tibial shaft fracture, the fracture is most commonly observed to deviate into which deformity?
Explanation
Question 55
A 38-year-old male sustains a pelvic ring injury and presents with a large, fluctuant swelling over the greater trochanter with ecchymosis. What is the underlying pathophysiology of this specific soft tissue lesion?
Explanation
Question 56
A 6-year-old boy falls on an outstretched hand and sustains a Bado Type I Monteggia equivalent fracture. Which of the following describes this classic injury pattern?
Explanation
Question 57
A 45-year-old female sustains a 'terrible triad' injury to the elbow. During surgical reconstruction, after fixing the coronoid and radial head, the elbow remains persistently unstable in extension. What is the next most appropriate step?
Explanation
Question 58
When treating a completely displaced intra-articular distal radius fracture with a volar locking plate, the plate must be placed proximal to the watershed line to minimize the risk of which complication?
Explanation
Question 59
A 25-year-old agricultural worker sustains a Gustilo-Anderson Type IIIA open tibia fracture heavily contaminated with soil. In addition to a first-generation cephalosporin and an aminoglycoside, what prophylactic antibiotic is indicated?
Explanation
Question 60
A 7-year-old girl sustains an extension-type supracondylar fracture of the humerus that is posteromedially displaced. Which nerve is at the highest risk of injury in this specific displacement pattern?
Explanation
Question 61
A 30-year-old male sustains a high-energy basicervical femoral neck fracture. To minimize the risk of avascular necrosis, which of the following is the most critical principle of management?
Explanation
Question 62
A 35-year-old male sustains a subtrochanteric femur fracture. During intramedullary nailing, the proximal fragment is typically difficult to reduce due to unopposed muscle forces. What is the characteristic deformity of the proximal fragment and the primary muscle responsible for its flexion?
Explanation
None
