Introduction & Epidemiology
Osteonecrosis of the humeral head (ONFH), commonly referred to as avascular necrosis (AVN), represents a debilitating condition characterized by the death of osteocytes and marrow cells due to an interruption of the blood supply to the humeral head. This ischemic insult leads to subchondral bone collapse, articular cartilage incongruity, and ultimately, glenohumeral osteoarthritis. While multifactorial in etiology, corticosteroid use is a prominent and well-recognized risk factor, significantly contributing to the incidence of non-traumatic ONFH.
The pathophysiology of corticosteroid-induced ONFH is complex, involving multiple proposed mechanisms. These include fat embolization leading to microvascular occlusion, corticosteroid-induced hypercoagulability, increased intraosseous pressure secondary to marrow adipogenesis, direct cytotoxicity to osteocytes, and impairment of reparative angiogenesis. High-dose and prolonged corticosteroid administration, particularly systemic corticosteroids, are strongly implicated. While a direct dose-response relationship is challenging to quantify definitively across all patients due to individual variability, cumulative dose, duration of therapy, and underlying conditions requiring steroid treatment are all critical considerations.
Epidemiologically, ONFH is less common than osteonecrosis of the femoral head, but its prevalence is increasing, partly due to the wider use of corticosteroids in various medical conditions and improved diagnostic imaging. It can affect individuals across a broad age spectrum, though corticosteroid-associated cases tend to manifest in adults. Other significant risk factors include heavy alcohol consumption, trauma (e.g., proximal humerus fractures disrupting vascularity), sickle cell disease, Gaucher's disease, systemic lupus erythematosus, HIV infection, organ transplantation, chemotherapy, radiation therapy, and diving-related decompression sickness. Approximately 15-20% of cases are idiopathic.
The natural history of ONFH is often characterized by progressive deterioration. Initially, patients may be asymptomatic or experience mild, intermittent shoulder pain. As the disease progresses, subchondral bone collapse ("crescent sign") develops, leading to increasingly severe pain, loss of range of motion, and functional impairment. Without intervention, joint destruction and secondary osteoarthritis are common sequelae.
Several classification systems are utilized to stage ONFH, guiding prognosis and treatment decisions:
*
Ficat and Arlet Classification:
Originally for femoral head AVN, adapted for the humeral head. Stages range from 0 (preclinical, pre-radiographic) to IV (severe collapse and secondary osteoarthritis).
*
Steinberg Classification:
A more detailed system, also adapted from the hip, incorporating the percentage of humeral head involvement. Stages 0-VI, with I and II representing pre-collapse, III and IV representing collapse, and V and VI representing end-stage arthritis.
*
ARCO (Association Research Circulation Osseous) Classification:
A contemporary international system that emphasizes MRI findings for early diagnosis. Stages 0-IV, with Stage I often detectable only by MRI, Stage II showing radiographic changes without collapse, Stage III with subchondral collapse, and Stage IV with secondary osteoarthritis. These classifications are crucial for standardized communication and for stratifying patients for appropriate management pathways.
Surgical Anatomy & Biomechanics
A thorough understanding of the surgical anatomy of the proximal humerus and glenohumeral joint, particularly its vascular supply, is paramount for both diagnosis and surgical management of ONFH.
The humeral head receives its primary blood supply from the ascending branch of the anterior humeral circumflex artery (AHCA) and branches from the posterior humeral circumflex artery (PHCA).
* The
ascending branch of the AHCA
, often termed the arcuate artery, penetrates the humerus just distal to the articular margin, typically beneath the bicipital groove. It then courses superiorly within the bone, supplying the majority of the anterosuperior humeral head and subchondral bone. This vessel is crucial and highly susceptible to compromise in trauma and surgical dissections.
* The
PHCA
branches provide additional supply to the posterior and inferior aspects of the humeral head, anastomosing with the AHCA branches. The PHCA typically courses around the surgical neck of the humerus, deep to the deltoid, and sends numerous branches into the bone.
* Additional contributions come from the suprascapular artery, thoracocromial artery, and deltoid perforators, though these are typically less significant for the humeral head itself.
The vulnerability of the humeral head's blood supply stems from its terminal end-artery configuration and the limited collateralization, particularly in the critical weight-bearing superior and anterior portions. Ischemia, often triggered by mechanisms like fat embolization, direct vascular damage (trauma), or increased intraosseous pressure, preferentially affects this region.
Biochemically, the glenohumeral joint is a ball-and-socket articulation designed for extensive range of motion at the expense of inherent stability.
* The
humeral head
is approximately one-third of a sphere, articulating with the much smaller, pear-shaped glenoid fossa. This incongruity necessitates dynamic stabilization from the rotator cuff muscles (supraspinatus, infraspinatus, teres minor, subscapularis) and static stabilization from the labrum, glenohumeral ligaments, and joint capsule.
* In ONFH, the integrity of the subchondral bone is compromised. As osteonecrosis progresses, the necrotic segment weakens, leading to mechanical collapse of the articular surface. This collapse creates an incongruous joint surface, altering load distribution, accelerating articular cartilage degeneration, and leading to pain and crepitus.
* The
rotator cuff
muscles, particularly the supraspinatus, are vital for centering the humeral head on the glenoid and initiating abduction. Their integrity is critical for successful outcomes in anatomical shoulder arthroplasty (hemiarthroplasty or total shoulder arthroplasty) for ONFH. Severe collapse and associated glenoid wear can further destabilize the joint, sometimes necessitating a reverse shoulder arthroplasty if rotator cuff function is compromised.
*
Neural structures
of significant surgical relevance include the axillary nerve (courses around the surgical neck, susceptible during inferior capsular release or deltoid manipulation), musculocutaneous nerve (pierces the coracobrachialis, providing motor innervation to biceps and brachialis), and radial nerve (lies posterior to the humerus, distal to the surgical neck, particularly vulnerable in distal humeral exposure or fracture fixation). Proximity to the deltopectoral interval, the workhorse approach for most shoulder arthroplasties, requires careful identification and protection of the cephalic vein and branches of the deltoid arteries and nerves.
Indications & Contraindications
The management of ONFH is tailored to the stage of the disease, the patient's symptoms, functional demands, age, and comorbidities. The primary goals are pain relief, preservation of joint function, and prevention of further collapse.
Non-Operative Indications
Non-operative management is typically considered for:
*
Early Stages (Pre-Collapse):
ARCO Stage 0-I, Steinberg Stage I-II, where there is no radiographic evidence of subchondral collapse or articular incongruity. Pain is often mild and intermittent.
*
Asymptomatic Patients:
Even with radiographic evidence of early ONFH, if the patient is pain-free and has full function.
*
Patients with Significant Surgical Contraindications:
Uncontrolled systemic infections, severe cardiovascular or pulmonary disease, or other medical conditions precluding surgery.
*
Low Functional Demand:
Elderly, sedentary patients with minimal pain and acceptable function who wish to avoid surgery.
*
Conservative Measures:
Pain medications (NSAIDs), activity modification, physical therapy for range of motion and strengthening (without stressing the necrotic segment), corticosteroid dose reduction or cessation (if medically feasible), bisphosphonates (off-label use, some evidence for slowing progression), statins.
Operative Indications
Surgical intervention is indicated for:
*
Pre-Collapse Stages (Preservation Procedures):
ARCO Stage I-II, Steinberg Stage I-II.
*
Core Decompression:
To reduce intraosseous pressure and promote revascularization. Often augmented with bone grafting (autograft, allograft, synthetic) or cellular therapies (e.g., concentrated bone marrow aspirate, mesenchymal stem cells). This is most effective when performed before the "crescent sign" or subchondral collapse appears.
*
Post-Collapse Stages (Reconstruction/Replacement Procedures):
ARCO Stage III-IV, Steinberg Stage III-VI.
*
Osteotomy:
While common in hip ONFH, less frequently used for the shoulder due to complex anatomy and unpredictable outcomes. May be considered in very specific cases of focal, contained lesions.
*
Humeral Head Resurfacing Arthroplasty:
For relatively young patients with preserved glenoid cartilage and a contained necrotic lesion, where only the articular surface of the humeral head is replaced.
*
Hemiarthroplasty:
For patients with significant humeral head collapse, intact glenoid articular cartilage, and a functional rotator cuff. This replaces only the humeral head with a prosthetic component.
*
Total Shoulder Arthroplasty (TSA):
For patients with advanced ONFH involving both humeral head collapse and symptomatic glenoid articular cartilage degeneration, with an intact and functional rotator cuff.
*
Reverse Total Shoulder Arthroplasty (rTSA):
Indicated for patients with advanced ONFH, particularly when associated with massive, irreparable rotator cuff tears, severe glenoid erosion, or as a salvage procedure for failed previous arthroplasty.
Contraindications
General contraindications for shoulder surgery include:
* Active local or systemic infection.
* Uncontrolled medical comorbidities (e.g., unstable angina, recent MI, severe diabetes, uncontrolled hypertension).
* Neuropathic joint (Charcot arthropathy).
* Significant deltoid dysfunction (absolute contraindication for rTSA, relative for TSA).
* Poor bone stock precluding implant fixation.
* Irreparable brachial plexus injury or other severe neurologic deficits affecting shoulder function.
* Patient unwillingness to comply with post-operative rehabilitation protocols.
Table 1: Operative vs. Non-Operative Indications for ONFH
| Management Strategy | Indications | Contraindications / Considerations |
|---|---|---|
| Non-Operative | - Asymptomatic ONFH | - Progressive pain and functional limitation despite conservative measures |
| - Early stage ONFH (ARCO 0-I, Steinberg I-II) without subchondral collapse | - Rapid radiographic progression | |
| - Mild, intermittent symptoms | - Significant subchondral collapse (crescent sign) | |
| - Significant surgical contraindications (e.g., active infection, severe comorbidities) | - High functional demands in younger patients where joint preservation is a priority | |
| - Low functional demand (e.g., sedentary elderly patients) | ||
| Operative | ||
| Preservation | ||
| Core Decompression | - Early stage ONFH (ARCO I-II, Steinberg I-II) with pain, before subchondral collapse | - Subchondral collapse (crescent sign) or frank articular cartilage collapse (ARCO III-IV) |
| (+ Grafting/Biologics) | - Small to medium-sized lesions (usually <30-50% of humeral head) | - Diffuse lesions involving a large portion of the humeral head |
| - Young, active patients where joint preservation is critical | - Active infection | |
| Arthroplasty | ||
| Hemiarthroplasty | - Advanced ONFH (ARCO III-IV, Steinberg III-V) with significant humeral head collapse | - Significant glenoid erosion/arthrosis (relative contraindication, favors TSA) |
| - Intact and functional glenoid articular cartilage | - Massive, irreparable rotator cuff tear (absolute contraindication, favors rTSA) | |
| - Intact and functional rotator cuff | - Very high functional demand (consider resurfacing in highly selected young patients, or TSA for more predictable motion) | |
| - Younger, active patients with glenoid preservation as a goal | ||
| Total Shoulder Arthroplasty (TSA) | - Advanced ONFH (ARCO III-IV, Steinberg IV-VI) with both humeral head collapse and symptomatic glenoid arthrosis | - Massive, irreparable rotator cuff tear with superior humeral head migration (absolute contraindication, favors rTSA) |
| - Intact and functional rotator cuff | - Significant deltoid dysfunction | |
| - Older patients or patients with lower functional demands where predictable pain relief and moderate function are desired | - Severe bone loss precluding stable glenoid component fixation | |
| Reverse Total Shoulder Arthroplasty (rTSA) | - Advanced ONFH (ARCO III-IV, Steinberg IV-VI) with concurrent massive, irreparable rotator cuff tear and superior humeral migration | - Functional axillary nerve palsy (deltoid innervation) |
| - Failed prior anatomical arthroplasty (hemi/TSA) for ONFH, especially with rotator cuff deficiency | - Active glenohumeral infection (contraindication for primary procedure, requires staged management if prior infection) | |
| - Significant glenoid bone loss precluding baseplate fixation (relative, may require bone grafting) | - Patient's inability to comply with post-operative restrictions or rehabilitation | |
| - Older patients with limited active forward flexion due to cuff deficiency, seeking pain relief and improved active elevation |
Pre-Operative Planning & Patient Positioning
Meticulous pre-operative planning is essential for optimizing outcomes and mitigating complications in ONFH surgery.
Workup
- Clinical History: Detailed history of shoulder pain (onset, character, aggravating/alleviating factors), functional limitations, corticosteroid use (dose, duration, indication), alcohol intake, comorbidities (sickle cell, lupus, transplant history), and prior shoulder interventions.
- Physical Examination: Assessment of active and passive range of motion (forward flexion, abduction, external rotation, internal rotation), rotator cuff strength, deltoid function, neurovascular status, and identification of pain provocation. Crepitus, grinding, and tenderness over the humeral head are common.
-
Imaging Studies:
-
Plain Radiographs:
Anteroposterior (AP) in internal and external rotation, scapular Y view, and axillary lateral view are standard. Early signs include subtle changes in trabecular pattern, sclerosis, and cystic lesions. The classic "crescent sign" (subchondral radiolucent line) indicates subchondral collapse. Later stages show flattening of the humeral head, joint space narrowing, osteophytes, and secondary glenohumeral osteoarthritis.
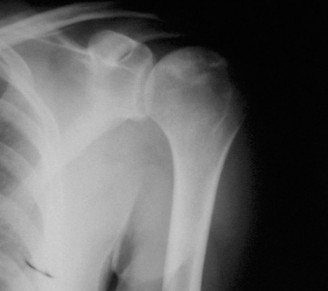
Fig 1: Advanced ONFH with significant humeral head collapse and secondary glenohumeral arthrosis evident on plain radiograph. - Magnetic Resonance Imaging (MRI): The most sensitive imaging modality for early diagnosis of ONFH, often detecting lesions before radiographic changes. T1-weighted images typically show low signal intensity, while T2-weighted images show high signal intensity (edema). The characteristic "double-line sign" (a low signal intensity line surrounded by a high signal intensity line on T2-weighted images) is highly specific for ONFH. MRI also helps assess lesion size, extent, and integrity of the rotator cuff and glenoid cartilage.
- Computed Tomography (CT) Scan: Particularly useful in advanced stages to delineate the extent of subchondral collapse, assess the precise bony architecture of the humeral head, quantify glenoid bone loss or erosion, and aid in templating for arthroplasty components. 3D reconstructions are invaluable for understanding complex deformities.
- Bone Scintigraphy: Technetium-99m bone scans can show increased uptake in the periphery of the necrotic lesion (reparative phase) and decreased uptake centrally (ischemic area). While sensitive, it is not specific and has largely been supplanted by MRI for early diagnosis.
-
Plain Radiographs:
Anteroposterior (AP) in internal and external rotation, scapular Y view, and axillary lateral view are standard. Early signs include subtle changes in trabecular pattern, sclerosis, and cystic lesions. The classic "crescent sign" (subchondral radiolucent line) indicates subchondral collapse. Later stages show flattening of the humeral head, joint space narrowing, osteophytes, and secondary glenohumeral osteoarthritis.
Templating & Pre-operative Planning
- Core Decompression: Requires fluoroscopic guidance; planning involves identifying the necrotic zone and appropriate entry points to avoid articular cartilage and neurovascular structures.
-
Arthroplasty (Hemi, TSA, rTSA):
- Humeral Side: Assess humeral canal size and geometry for stem selection (cemented vs. press-fit). Determine humeral head size, version, and inclination. Consider osteotomy options for version correction in certain cases.
- Glenoid Side: For TSA, assess glenoid bone stock, erosion, and version. Plan for reaming and component size/fixation (pegged vs. keeled, cemented vs. biologic). For rTSA, precisely plan glenoid baseplate position and fixation to optimize stability and prevent scapular notching. Software-based 3D planning using CT scans is becoming standard for complex glenoid deformities.
- Patient Consent: Comprehensive discussion of the surgical procedure, potential benefits, risks (infection, nerve injury, dislocation, loosening, continued pain), alternatives, and anticipated recovery. Emphasize the possibility of revision surgery.
- Medical Optimization: Coordinate with primary care physicians or specialists to optimize any underlying medical conditions (e.g., blood glucose control in diabetes, cardiac optimization). Manage corticosteroid use; abrupt cessation is contraindicated, but a stress dose may be required perioperatively.
Patient Positioning
The choice of patient positioning depends on the planned surgical approach and surgeon preference.
1.
Beach Chair Position:
*
Advantages:
Allows for easy access to the superior, anterior, and posterior aspects of the shoulder. Facilitates intraoperative assessment of range of motion and stability. Surgeon operates standing upright, ergonomic.
*
Disadvantages:
Risk of cerebral hypoperfusion (especially with hypotension or excessive head elevation), potential for brachial plexus traction injury, and difficult access to the posterior axilla/distal humerus for extensive exposure.
*
Setup:
Patient is semi-recumbent (30-70 degrees of trunk elevation). Head is supported in a headrest (e.g., "donut" or Mayfield clamp for rTSA). Back is supported. Arm is free-draped to allow full manipulation. Axillary roll placed to prevent brachial plexus compression. Torso secured to the table. Legs slightly flexed.
2.
Lateral Decubitus Position:
*
Advantages:
Excellent exposure of the glenohumeral joint and posterior structures. Less risk of cerebral hypoperfusion.
*
Disadvantages:
More challenging to assess range of motion and stability dynamically. Requires careful patient positioning to prevent nerve compression (ulnar, peroneal) and proper support of the non-operative arm.
*
Setup:
Patient lies on their side with the operative shoulder superior. Bean bag positioner used to secure the patient. Axillary roll placed inferior to the chest wall. Dependent arm is well-padded. Operative arm is suspended in traction (often with weights) or held free for manipulation.
Anesthesia: General anesthesia is standard. An interscalene brachial plexus block is often used as an adjunct for post-operative pain control, either pre-operatively or intraoperatively by the anesthesiologist.
Detailed Surgical Approach / Technique
The surgical technique for ONFH varies significantly depending on the stage of the disease and the chosen intervention.
1. Core Decompression (for Pre-Collapse AVN)
Goal:
Reduce intraosseous pressure and stimulate revascularization to prevent or delay collapse.
*
Approach:
Typically a deltopectoral approach for a medial lesion or a small lateral deltoid split for a more lateral lesion. A small incision (2-3 cm) is sufficient.
*
Technique:
1.
Fluoroscopic Guidance:
Essential for accurate localization of the necrotic zone and ensuring appropriate drill trajectories. An AP view, lateral view, and potentially oblique views are used.
2.
Entry Point:
Typically on the lateral cortex of the humerus, approximately 4-6 cm distal to the articular surface, aiming to avoid the articular cartilage, rotator cuff insertion, and major neurovascular structures.
3.
Drilling:
A guide pin is inserted and advanced under fluoroscopic control into the necrotic zone. The pin should reach within 5-10 mm of the subchondral bone plate without penetrating the articular cartilage.
4.
Cannulation:
A cannulated drill (e.g., 6-8 mm diameter) is advanced over the guide pin. Multiple drilling channels may be created, fanning out into the necrotic zone, to adequately decompress the area.
5.
Debridement/Grafting (Optional):
The necrotic bone may be debrided through the channels. The void can then be filled with bone graft (autogenous cancellous bone from the iliac crest or proximal humerus, allograft, or synthetic bone substitutes) or augmented with concentrated bone marrow aspirate (BMAC) or mesenchymal stem cells (MSCs) to enhance healing and revascularization. The choice of biologic augmentation is surgeon-dependent and based on available evidence.
6.
Closure:
Layered closure of the incision.
2. Hemiarthroplasty (for Collapsed AVN with Intact Glenoid/Cuff)
Goal:
Replace the diseased humeral head while preserving the glenoid.
*
Approach:
Standard deltopectoral approach.
1.
Incision:
A curvilinear incision from the coracoid process extending distally for approximately 10-12 cm.
2.
Internervous Plane:
Dissect between the deltoid muscle (axillary nerve innervation) laterally and the pectoralis major muscle (medial and lateral pectoral nerve innervation) medially. The cephalic vein is identified and typically retracted laterally with the deltoid.
3.
Subscapularis Management:
The anterior capsule and subscapularis tendon are exposed. The subscapularis can be incised either by tenotomy (repaired later) or a lesser tuberosity osteotomy (preferred by some for potentially better healing and exposure, especially in revision cases). Tag sutures are placed for later repair.
4.
Humeral Head Resection:
The arm is externally rotated and extended. The humeral head is dislocated anteriorly. The level of osteotomy is carefully determined, typically at an angle of 30-45 degrees of retroversion and 130-135 degrees of inclination relative to the humeral shaft. An oscillating saw is used to resect the necrotic humeral head.
5.
Humeral Preparation:
The humeral canal is identified. Progressive reaming and broaching are performed to prepare the intramedullary canal for the humeral stem. Trials are used to determine appropriate stem size, version, and depth.
6.
Component Sizing and Implantation:
A trial humeral head component is selected based on diameter, height, and offset to match the patient's anatomy and restore joint kinematics. Final humeral stem and head components are implanted (cemented or press-fit).
7.
Reduction and Stability:
The joint is reduced. Range of motion and stability are assessed throughout the arc of motion.
8.
Closure:
The subscapularis tendon (or osteotomy fragment) is meticulously repaired to the lesser tuberosity with strong non-absorbable sutures. The capsule is closed if possible. Deltopectoral interval is loosely approximated. Subcutaneous layers and skin are closed.

Fig 2: Intraoperative view during a shoulder arthroplasty, showing preparation of the humeral canal for stem insertion after humeral head resection.
3. Total Shoulder Arthroplasty (TSA - for Collapsed AVN with Glenoid Arthrosis and Intact Cuff)
Goal:
Replace both the humeral head and glenoid articular surface.
*
Approach:
Similar deltopectoral approach and humeral preparation as for hemiarthroplasty.
*
Glenoid Preparation:
1. After humeral head resection, the glenoid is exposed. Care is taken to protect the axillary nerve inferiorly.
2. The glenoid labrum and osteophytes are debrided.
3. Progressive reaming of the glenoid surface is performed to create a flat, concentric surface perpendicular to the scapular neck. Intraoperative fluoroscopy or guides may be used to ensure correct version and inclination.
4. Pilot holes are drilled for the glenoid component keel or pegs.
5. The glenoid component (polyethylene) is implanted, typically cemented, ensuring full seating and stable fixation.
*
Humeral Component:
As described for hemiarthroplasty.
*
Soft Tissue Balancing:
The key to successful TSA is careful soft tissue balancing to achieve full, stable range of motion without impingement. This involves appropriate humeral head component selection (thickness, offset) and capsular management.
*
Closure:
Meticulous repair of the subscapularis and capsular closure as described for hemiarthroplasty.
4. Reverse Total Shoulder Arthroplasty (rTSA - for Collapsed AVN with Massive Cuff Tear/Glenoid Erosion)
Goal:
Medialize the center of rotation and recruit the deltoid for elevation, bypassing a deficient rotator cuff.
*
Approach:
Deltopectoral approach is standard.
*
Humeral Head Resection:
Resection of the humeral head is similar to TSA/hemi.
*
Glenoid Preparation:
1. Glenoid exposure is critical. The surgeon must gain sufficient access to the glenoid face, often requiring partial inferior capsular release, to ensure proper baseplate placement.
2. The glenoid baseplate is prepared by reaming the glenoid to a flat surface.
3. A central peg hole and peripheral screw holes are drilled. The baseplate is secured with locking screws into the scapular vault, ensuring strong fixation. This step is critical for stability and longevity.
4. The glenosphere (hemispherical metallic component) is then locked onto the baseplate.
*
Humeral Preparation:
1. The humeral canal is prepared with reamers and broaches.
2. A humeral stem (often cemented) is inserted.
3. A polyethylene liner is then affixed to the humeral stem.
*
Reduction and Stability:
The humeral liner is articulated with the glenosphere. Stability and range of motion are assessed. Deltoid tensioning is crucial; too much tension can lead to nerve injury, too little can lead to instability.
*
Closure:
The subscapularis is typically not repaired in rTSA as the mechanics bypass its function. Capsule is closed if possible. Deltopectoral interval approximated.
Complications & Management
Complications following surgical interventions for ONFH, particularly arthroplasty, can be significant and require prompt recognition and management.
Table 2: Common Complications, Incidence, and Salvage Strategies in ONFH Surgery
| Complication | Incidence (Approx.) | Salvage / Management Strategy |
|
Core Decompression
| 0-1% direct articular damage; risk of progression is low but variable (20-40% fail over 5 years). |
Clinical & Radiographic Imaging

