Medial Epicondyle ORIF: An Intraoperative Masterclass in Open Reduction and Internal Fixation

Key Takeaway
Master the open reduction and internal fixation of medial epicondyle fractures. This intraoperative guide covers comprehensive surgical anatomy, meticulous step-by-step technique, critical pearls and pitfalls, and robust postoperative management. Gain insights into precise instrument use, neurovascular protection, and advanced strategies for optimal patient outcomes. Perfect for orthopaedic fellows.
Comprehensive Introduction and Patho-Epidemiology
Welcome to the operating theater. Today, we are presented with a highly instructive and technically demanding case: an open reduction and internal fixation (ORIF) of a displaced medial epicondyle fracture in a high-demand, athletic patient. The management of medial epicondyle fractures has historically been a topic of vigorous debate within the orthopedic community. While nonoperative management has traditionally been favored for minimally displaced fractures in sedentary individuals, the modern consensus heavily favors surgical intervention for athletes, overhead throwers, and patients with high functional demands. This paradigm shift recognizes that we are not merely treating a bony avulsion; we are fundamentally restoring the critical medial stabilizing complex of the elbow.
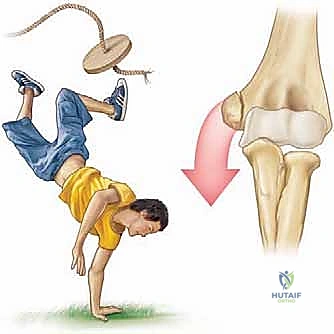
Medial epicondyle fractures represent approximately 11% to 20% of all pediatric elbow fractures, with a peak incidence occurring between the ages of 9 and 14 years. This demographic distribution corresponds directly to the vulnerability of the medial epicondylar apophysis prior to its final radiographic fusion, which typically occurs between 15 and 18 years of age. The pathophysiology of this injury is almost exclusively driven by an indirect, avulsion-type mechanism. During a fall on an outstretched hand (FOOSH) with the elbow in terminal extension, a massive valgus moment is generated. This force translates into extreme tensile stress across the medial structures. The robust flexor-pronator muscle mass and the anterior bundle of the ulnar collateral ligament (UCL) subsequently avulse the weaker apophyseal growth plate.
Direct trauma to the medial aspect of the elbow is a distinctly rare cause of this fracture pattern. Far more commonly, these fractures are intimately associated with an acute elbow dislocation, occurring in up to 50% of displaced medial epicondyle fractures. It is imperative to understand that the elbow may spontaneously reduce prior to the patient's arrival at the emergency department. Consequently, a high index of suspicion for a transient dislocation event must be maintained, as this implies a more extensive soft-tissue injury, including disruption of the lateral collateral ligamentous complex and the anterior capsule.
Clinical presentation is characterized by profound medial-sided ecchymosis, swelling, and point tenderness directly over the medial epicondyle. A meticulous physical examination is paramount, with a specific focus on neurovascular integrity and ligamentous stability. The ulnar nerve is intimately associated with the medial epicondyle, and preoperative documentation of its sensory and motor function is a strict medicolegal and clinical requirement. Furthermore, a careful valgus stress test—ideally performed under fluoroscopy or anesthesia—will unmask occult medial instability. Failure to recognize and address this instability in a high-demand patient will inevitably lead to chronic valgus extension overload, secondary radiocapitellar joint degeneration, and a profound inability to return to pre-injury levels of athletic performance.
Detailed Surgical Anatomy and Biomechanics
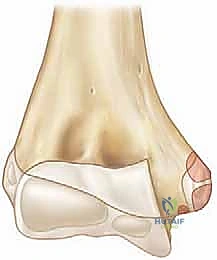
A profound mastery of the medial elbow anatomy is the absolute prerequisite for safe and effective surgical intervention. The medial epicondyle is not merely a bony prominence; it is the critical functional nexus for the medial soft-tissue envelope of the elbow. It serves as the common origin for the flexor-pronator mass (FPM) and the proximal attachment site for the ulnar collateral ligament (UCL). Understanding the vectors of pull from these structures is essential for comprehending fracture displacement patterns and executing a successful reduction.
The Flexor-Pronator Mass and Ulnar Collateral Ligament
The flexor-pronator mass originates from the anterior and inferior aspects of the medial epicondyle. This robust muscle group comprises the pronator teres, flexor carpi radialis, palmaris longus, flexor digitorum superficialis, and flexor carpi ulnaris. When the apophysis is avulsed, the resting tone and active contraction of these muscles displace the fragment distally, anteriorly, and often internally rotate it. The UCL, specifically its anterior bundle, is the primary restraint to valgus stress at the elbow, providing over 50% of the valgus stability from 20 to 120 degrees of flexion. The anterior bundle originates from the anteroinferior surface of the medial epicondyle and inserts onto the sublime tubercle of the proximal ulna. Because the UCL remains attached to the avulsed epicondylar fragment, the fracture inherently represents a functional UCL rupture. Restoring the bony anatomy is therefore synonymous with restoring the ligamentous stability of the joint.
The Ulnar Nerve and Cubital Tunnel
The ulnar nerve is the most critical structure at risk during both the initial injury and the subsequent surgical approach. The nerve courses distally through the posterior compartment of the arm, piercing the medial intermuscular septum at the arcade of Struthers, before entering the cubital tunnel. The cubital tunnel is bordered anteriorly by the medial epicondyle, laterally by the elbow joint capsule and the posterior band of the UCL, and medially by the Osborne ligament (cubital tunnel retinaculum). In the setting of a medial epicondyle fracture, the normal anatomical boundaries of the cubital tunnel are disrupted. The nerve can be stretched by the initial valgus force, compressed by fracture hematoma, or even directly incarcerated within the elbow joint along with the bony fragment. Surgical dissection must proceed with extreme caution, utilizing meticulous hemostasis to identify and protect the nerve before any fracture manipulation occurs.
Osseous Landmarks and Ossification Centers
For pediatric and adolescent patients, a thorough understanding of the radiographic appearance of the secondary ossification centers is crucial. The mnemonic CRITOE (Capitellum, Radial head, Internal/medial epicondyle, Trochlea, Olecranon, External/lateral epicondyle) dictates the chronological order of appearance. The medial epicondyle typically ossifies between ages 4 and 6 and fuses to the distal humeral shaft between ages 15 and 18. Because the apophysis is largely cartilaginous in younger patients, plain radiographs may grossly underestimate the true size of the avulsed fragment and the extent of the soft-tissue disruption. Furthermore, the surgeon must be acutely aware of the olecranon fossa, located immediately posterior and lateral to the medial epicondyle. Any hardware traversing the epicondyle must be directed anteriorly to avoid breaching the fossa, which would result in a catastrophic mechanical block to terminal elbow extension.
Exhaustive Indications and Contraindications
The decision-making process for operative versus nonoperative management of medial epicondyle fractures requires a nuanced synthesis of patient age, activity level, fracture displacement, and associated injuries. While conservative management (immobilization for 1 to 3 weeks followed by progressive range of motion) is acceptable for minimally displaced fractures in low-demand individuals, the threshold for surgery drops significantly in athletic populations.
| Parameter | Absolute Indications for ORIF | Relative Indications for ORIF | Contraindications for ORIF |
|---|---|---|---|
| Fragment Position | Intra-articular incarceration of the fragment | Displacement > 5 mm in general population | Minimally displaced (< 2 mm) in low-demand patient |
| Athletic Demand | Overhead throwing athlete with any displacement | Displacement > 2 mm in high-demand athlete | Sedentary lifestyle with acceptable alignment |
| Neurological Status | Progressive or acute severe ulnar neuropathy | Mild, non-progressive ulnar nerve symptoms | Normal neurovascular status (if other criteria unmet) |
| Joint Stability | Gross valgus instability on stress examination | Suspected UCL incompetence | Stable joint under dynamic fluoroscopic stress |
| Associated Injuries | Open fracture | Concomitant elbow dislocation requiring stabilization | Polytrauma precluding safe operative intervention |
| Patient Factors | Symptomatic nonunion from previous injury | Need for early, aggressive rehabilitation | Active local infection or severe medical comorbidities |
Intra-articular incarceration of the medial epicondyle is an absolute surgical emergency. This typically occurs following an elbow dislocation; as the joint reduces, the epicondyle and its attached soft tissues are sucked into the ulnohumeral articulation. Attempting closed extraction via joint manipulation is fraught with risk, including iatrogenic ulnar nerve injury and further cartilaginous damage, making open extraction and fixation the standard of care.
In the context of overhead athletes, the indications for surgery are aggressively expanded. Even minimal displacement (2-3 mm) can result in a functionally elongated UCL, leading to subtle valgus instability. During the late cocking and early acceleration phases of throwing, the medial elbow experiences extraordinary valgus loads. A non-anatomically healed medial epicondyle will fail to withstand these forces, inevitably leading to chronic pain, decreased throwing velocity, and secondary injuries such as ulnar neuritis or radiocapitellar chondromalacia. Therefore, ORIF in this demographic is viewed not just as fracture care, but as a mandatory joint-preserving stabilization procedure.
Pre-Operative Planning, Templating, and Patient Positioning
Meticulous preoperative planning is the foundation of a smoothly executed surgical procedure. The planning phase begins with a comprehensive radiographic evaluation. Standard anteroposterior (AP) and true lateral radiographs of the elbow are mandatory. However, because the medial epicondyle sits posteromedially on the distal humerus, standard AP views often obscure the true magnitude of displacement. Therefore, an internal oblique view is highly recommended to profile the medial column. Furthermore, a gravity valgus stress radiograph can be utilized to dynamically assess medial collateral ligament competence and occult fracture displacement.
In cases of significant comminution, suspected intra-articular incarceration that is ambiguous on plain films, or when evaluating a chronic nonunion, advanced imaging is warranted. A non-contrast Computed Tomography (CT) scan with 3D reconstructions provides invaluable information regarding the precise size, geometry, and rotational orientation of the fracture fragment, as well as the available bone stock in the distal humeral metaphysis for screw purchase. Magnetic Resonance Imaging (MRI) is less commonly required for acute fractures but is exceptionally useful for evaluating the integrity of the UCL and the flexor-pronator origin in subacute or chronic presentations.
Operating Room Setup and Patient Positioning
Optimal patient positioning is critical to facilitate both surgical access and unhindered fluoroscopic imaging. The patient is placed in the supine position on a standard operating table. The affected upper extremity is draped free and positioned on a radiolucent hand table. The arm is abducted to 90 degrees at the shoulder, and the forearm is externally rotated to present the medial aspect of the elbow directly to the surgical team.
The surgeon is typically positioned in the axilla, facing the medial elbow, which provides the most ergonomic angle for dissection, reduction, and hardware insertion. The C-arm fluoroscopy unit is brought in from the head or the contralateral side of the table, depending on the specific room configuration. It is imperative to perform a "dry run" with the C-arm prior to prepping and draping to ensure that perfect AP and lateral orthogonal views of the elbow can be obtained seamlessly without moving the patient's arm.
A sterile pneumatic tourniquet is applied high on the brachium. Exsanguination is achieved with an Esmarch bandage, and the tourniquet is inflated to approximately 250 mmHg (or 100 mmHg above the patient's systolic blood pressure). A completely bloodless field is not merely a convenience in this procedure; it is an absolute necessity for the safe identification and mobilization of the ulnar nerve, as well as for the precise anatomical reduction of the apophyseal fragment.
Step-by-Step Surgical Approach and Fixation Technique
With the patient positioned, prepped, and draped, and the tourniquet inflated, we commence the operative intervention. The surgical approach must be deliberate, respecting the delicate soft-tissue envelope and prioritizing the safety of the ulnar nerve at every stage.
1. Incision and Superficial Dissection
A longitudinal incision, approximately 4 to 6 centimeters in length, is made centered directly over the medial epicondyle. The incision can be slightly curved posteriorly to avoid crossing the flexion crease of the elbow at a right angle, which can lead to restrictive scar contracture. The dissection is carried sharply through the skin and subcutaneous tissues down to the investing fascia. Hemostasis is maintained using bipolar electrocautery to avoid thermal injury to cutaneous nerve branches, particularly the medial antebrachial cutaneous nerve, which arborizes in the distal aspect of the incision.

2. Ulnar Nerve Identification and Management
Before any attempt is made to identify or mobilize the fracture fragment, the ulnar nerve must be definitively localized. The fascia overlying the cubital tunnel is carefully incised. Using blunt dissection with a small hemostat or a peanut sponge, the ulnar nerve is identified proximal to the epicondyle and traced distally as it passes between the two heads of the flexor carpi ulnaris. Once identified, the nerve is gently mobilized and protected with a vessel loop.
The management of the ulnar nerve during medial epicondyle ORIF is a subject of debate. Routine anterior transposition is generally discouraged, as it requires more extensive dissection, devascularizes a segment of the nerve, and introduces the risk of iatrogenic compression at the fascial slings. In situ decompression and protection are preferred unless the nerve is frankly unstable, under excessive tension following fracture reduction, or if the patient presented with profound preoperative ulnar neuropathy.
3. Fracture Bed Preparation
With the ulnar nerve safely retracted posteriorly, the fracture site is exposed. The avulsed medial epicondyle is typically displaced distally and anteriorly, tethered by the robust flexor-pronator mass. The fracture bed on the distal humeral metaphysis is often obscured by organized hematoma, periosteal debris, and interposed muscle fibers.

Using a small curette, a Freer elevator, and copious irrigation, the fracture bed is meticulously debrided down to bleeding cancellous bone. Crucially, the undersurface of the avulsed epicondylar fragment must also be prepared. In older adolescents and adults, this involves removing clotted blood. In younger patients with a largely cartilaginous apophysis, many high-level surgeons advocate for aggressive curettage of the apophyseal cartilage down to the subchondral bone. This technique converts a potential fibrous nonunion (cartilage-to-bone healing) into a robust, primary osseous union (bone-to-bone healing), which is significantly more resilient to the extreme valgus stresses of overhead throwing.
4. Anatomical Reduction
Achieving an anatomical reduction requires neutralizing the deforming forces of the flexor-pronator mass. This is accomplished by flexing the elbow to 90 degrees and heavily pronating the forearm. With the deforming forces relaxed, a sharp towel clip or a small pointed reduction forceps is used to grasp the epicondylar fragment. The fragment is gently mobilized superiorly and posteriorly, docking it precisely into its anatomical footprint on the distal humerus. The reduction must be visually confirmed, ensuring the cortical margins interdigitate perfectly without any rotational malalignment.
5. Provisional Fixation
Once anatomical reduction is achieved, it is provisionally stabilized using 1.6 mm or 2.0 mm Kirschner wires (K-wires) or the guide pins from a cannulated screw system. The trajectory of these pins is absolutely critical. The starting point is on the anterior-inferior aspect of the medial epicondyle. The pins are directed superiorly, laterally, and anteriorly into the distal humeral metaphysis.


Directing the pins anteriorly is paramount to avoid penetrating the olecranon fossa. A second pin is highly recommended to provide rotational stability during the subsequent drilling and tapping phases. Following pin placement, the reduction and pin trajectory are rigorously evaluated using orthogonal AP and lateral fluoroscopy. The elbow is taken through a gentle range of motion under live fluoroscopy to confirm that the hardware does not impinge on the joint and that the reduction remains stable under dynamic stress.


6. Definitive Fixation
For definitive fixation, a 4.0 mm or 4.5 mm partially threaded cannulated screw is the gold standard. The appropriate screw length is determined using a depth gauge over the primary guide pin. The lateral cortex of the humerus should ideally be engaged to maximize pull-out strength, particularly in older patients or those with osteopenic bone.

The outer cortex of the epicondyle is overdrilled to create a gliding hole, facilitating interfragmentary compression. The screw is then advanced over the guide wire. If the epicondylar fragment is comminuted or if the patient is very young with a soft, cartilaginous apophysis, a spiked ligament washer or a standard low-profile washer should be utilized to distribute the compressive forces and prevent the screw head from burying into the fragment.
Once the primary screw is seated and excellent compression is achieved, the secondary anti-rotation K-wire is typically removed, unless the fragment is highly unstable, in which case it may be exchanged for a smaller secondary screw. Final fluoroscopic images are obtained to verify anatomical reduction, appropriate hardware length, and clearance of the olecranon fossa. The ulnar nerve is inspected one final time to ensure it is free from tension or hardware impingement before the wound is closed in layers.

Complications, Incidence Rates, and Salvage Management
While ORIF of the medial epicondyle is highly successful in restoring elbow stability and function, it is not without potential complications. A thorough understanding of these risks is essential for appropriate preoperative patient counseling and postoperative vigilance.
| Complication | Estimated Incidence | Etiology / Risk Factors | Salvage / Management Strategy |
|---|---|---|---|
| Ulnar Neuropathy | 5% - 15% | Iatrogenic traction, hardware impingement, post-op hematoma, or scarring. | Initial observation and EMG at 6 weeks. If progressive or refractory, requires surgical exploration, hardware removal, and potential submuscular anterior transposition. |
| Symptomatic Prominent Hardware | 10% - 25% | Superficial nature of the epicondyle, inadequate countersinking, patient habitus. | Elective hardware removal after clinical and radiographic union is confirmed (typically > 6-9 months post-op). |
| Loss of Terminal Extension (Stiffness) | 10% - 20% | Prolonged immobilization, hardware breaching the olecranon fossa, capsular contracture. | Aggressive physical therapy, dynamic splinting. If hardware is in the fossa, immediate removal. Late cases may require arthroscopic or open capsular release. |
| Nonunion / Fibrous Union | 2% - 5% | Failure to curette apophyseal cartilage, inadequate fixation, premature return to throwing. | If asymptomatic, observe. If symptomatic (pain, valgus instability), requires revision ORIF with bone grafting or UCL reconstruction using an autograft. |
| Heterotopic Ossification (HO) | 3% - 10% | Severe initial trauma, concomitant elbow dislocation, delayed surgical intervention. | Prophylactic NSAIDs (Indomethacin) or localized radiation in high-risk patients. If mature and restricting ROM, surgical excision is indicated. |
Ulnar neuropathy remains the most feared and heavily scrutinized complication. Transient neuropraxia is relatively common due to the necessary manipulation of the nerve during the exposure. However, persistent motor weakness or severe dysesthesia demands prompt investigation. If hardware impingement is suspected radiographically, immediate revision is mandatory.
Stiffness, particularly a loss of terminal extension (typically 5 to 15 degrees), is the most frequent functional complaint postoperatively. This underscores the critical importance of a rigid internal fixation construct that permits early, aggressive rehabilitation. Prolonged casting is functionally disastrous for the elbow joint and must be avoided whenever possible.
Phased Post-Operative Rehabilitation Protocols
The ultimate success of a medial epicondyle ORIF is heavily dependent on a meticulously structured, phased rehabilitation program. The goal is to balance the protection of the osteosynthesis with the imperative to prevent debilitating elbow stiffness.
Phase 1: Protection and Early Motion (Days 0 to 14)
Immediately postoperatively, the elbow is immobilized in a long-arm posterior splint at 90 degrees of flexion with the forearm in neutral rotation. This provides soft-tissue rest and protects the incision. At 7 to 10 days, the splint and sutures are removed. The patient is transitioned into a hinged elbow brace locked from 30 to 90 degrees. Active-assisted range of motion (AAROM) for elbow flexion and extension, as well as forearm pronation and supination, is initiated. Valgus stress is strictly prohibited.
Phase 2: Restoring Full Range of Motion (Weeks 2 to 6)
The hinged brace is progressively opened to allow full extension and flexion. The primary goal during this phase is to achieve full, symmetrical range of motion by 6 weeks postoperatively. Gentle passive stretching is incorporated if motion is lagging, but aggressive, painful manipulation is avoided to prevent heterotopic ossification. Isotonic strengthening of the wrist and shoulder is initiated, ensuring no excessive stress is transmitted across the medial elbow.
Phase 3: Progressive Strengthening (Weeks 6 to 12)
Radiographic union is typically evident by 6 to 8 weeks. Once clinical and radiographic union is confirmed, the hinged brace is discontinued. The focus shifts to progressive resistance exercises for the flexor-pronator mass, biceps, triceps, and the entire shoulder girdle. Scapular dyskinesia must be addressed, particularly in throwing athletes, as proximal kinetic chain deficits will transfer abnormal stresses to the healing medial elbow.
Phase 4: Return to Sport and Throwing (Months 3 to 6+)
For the overhead athlete, Phase 4 involves a highly structured, interval throwing program. This program begins with short-distance, flat-ground tossing and progresses gradually in distance, volume, and velocity over several months. Return to competitive pitching is rarely permitted before 5 to 6 months postoperatively, and only when the athlete demonstrates pain-free, full range of motion, symmetrical strength, and perfect throwing mechanics.
Summary of Landmark Literature and Clinical Guidelines
The evolution of treatment algorithms for medial epicondyle fractures is deeply rooted in clinical literature. Historically, studies by Farsetti et al. demonstrated acceptable long-term outcomes with nonoperative management for displaced fractures in the general pediatric population. However, these studies primarily evaluated activities of daily living and did not account for the extreme biomechanical demands of modern overhead athletes.
More recent, high-level evidence has catalyzed the shift toward operative intervention. Kamath et al. and Hines et al. have published landmark papers highlighting the high rates of symptomatic valgus instability and failure to return to sport in throwing athletes treated nonoperatively for displaced medial epicondyle fractures. These authors demonstrated that anatomical reduction and rigid internal fixation significantly restore the structural integrity of the anterior bundle of the UCL, allowing for a predictable return to high-level athletics.
Current clinical guidelines from major orthopedic societies reflect this nuanced understanding. While nonoperative management remains a viable option for low-demand patients with less than 5 mm of displacement, ORIF is now considered the standard of care for high-demand athletes with any degree of displacement that compromises the resting length and tension of the medial collateral ligament complex. The surgical technique detailed in this chapter—emphasizing ulnar nerve protection, meticulous bed preparation, and rigid cannulated screw fixation—represents the current zenith of evidence-based orthopedic practice for this challenging injury.
