DEFINITION
GANGLION CYSTS
Ganglion cysts, although not true cysts, are the most common tumors of the hand and wrist. These fluid-filled cysts are a frequent cause of hand and wrist pain.Ganglion cysts typically arise from either a joint or tendon sheath.Most ganglion cysts occur in the wrist. Dorsal wrist ganglion cysts account for 60% to 70% of all ganglion cysts, with volar wrist ganglion cysts accounting for about 18% to 20%.1Ganglion cysts may also arise from a tendon sheath (volar retinacular cyst) or occur in association with arthritis (degenerative mucous cyst).
GIANT CELL TUMORS
Giant cell tumors of the tendon sheath—also referred to aslocalized nodular synovitis,11fibrous xanthoma, andpigmented villonodular synovitis—are benign, slow-growing soft tissue tumors.After ganglion cyst cysts, these lesions are the second most common tumor in the hand.6
EPIDERMAL INCLUSION CYSTS
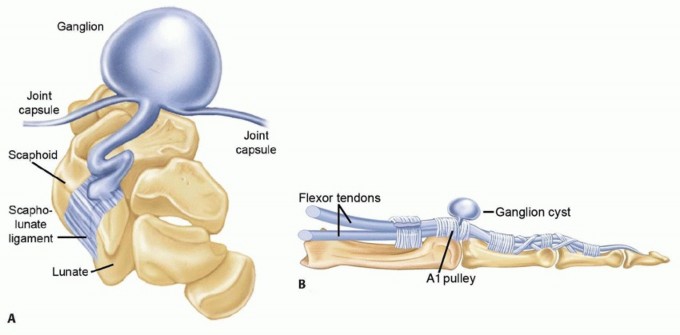
Epidermal inclusion cysts are benign, slow-growing soft tissue tumors. They are the third most common type of hand tumor. FIG 1 • A. Ganglion cyst arising from dorsal scapholunate joint. B. Ganglion cyst arising from flexor sheath.
ANATOMY
GANGLION CYSTS
Ganglion cysts typically consist of a cyst sac that communicates through a stalk to an underlying joint or tendon sheath (FIG 1).The cyst sac may have a single cavity or be multilobulated.Although not a true cyst, lacking an epithelial lining, ganglion cysts are typically filled with a clear, viscous, jelly-like mucinous fluid made up of glucosamine, albumin, globulin, and a high concentration of hyaluronic acid.17
GIANT CELL TUMORS
The tumor is usually a multilobular, well-circumscribed mass, ranging in size from 0.5 to 7 cm.6The color ranges from yellow to deep brown depending on the amount of hemosiderin, histiocytes, and collagen present in the lesion.These lesions have a thin pseudocapsule. Aggressive lesions may invade adjacent soft tissue, tendon, and capsular structures and can envelop neurovascular bundles. A large study showed joint involvement in one-fifth of all cases.7 Long-standing lesions may erode into cortical bone but will not involve cartilage or the medullary canal of bone. Satellite lesions may occur.Histologically, giant cell tumors contain collagen-producing polyhedral-shaped histiocytes, scattered multinucleated giant cells, and hemosiderin deposits.6P.1312
EPIDERMAL INCLUSION CYSTS
Epidermal inclusion cysts are well-circumscribed, firm, and slightly mobile lesions. They are often superficial and adherent to overlying skin.They may be flesh-colored, yellow, or white. They contain a thick, white, keratinous material.Cysts in the fingertip may erode into the distal phalanx, causing a lytic lesion. Histologically, they are cysts filled with keratin and lined with epithelial cells.
PATHOGENESIS
GANGLION CYSTS
The true causes of ganglion cysts remain unclear, although multiple theories have been proposed.Some early investigators theorized that ganglion cysts occurred as the result of synovial herniation and others felt that ganglion cysts resulted from mucoid degeneration.A more recent theory proposes that ganglion cysts arise from stress at the synovial capsular interface. This stress, such as stretching of the capsular and ligamentous structures, stimulates the production of mucin from modified synovial, mesenchymal, and fibroblast cells, all of which have been shown to produce hyaluronic acid. The mucin then dissects through the capsular and ligamentous tissues, forming the main cyst. The fluidmay enter the cyst from the capsular ligamentous interface via a one-way valve type of mechanism and then decrease as the water component is resorbed, accounting for the often-fluctuating cyst size.1
GIANT CELL TUMORS
The cause of giant cell tumors is not known. There is a strong association of giant cell tumors with rheumatoid arthritis. There are no clinical studies associating these tumors with trauma.6Although these tumors are histologically similar to the pigmented villonodular synovitis seen in large joints in the lower extremity, they are thought to be clinically distinct lesions.
EPIDERMAL INCLUSION CYSTS
Epidermal inclusion cysts occur as a result of trauma when epithelial cells are introduced into the underlying subcutaneous tissues or bone. These cells slowly grow to produce a cyst lined with epithelial cells and filled with keratin.
NATURAL HISTORY
GANGLION CYSTS
Ganglion cysts typically arise spontaneously and are most common in the second through the fourth decade but may arise in the pediatric population19 as well as the aged.Once present, ganglion cysts tend to fluctuate in size depending on the amount of fluid present in the cyst at any given time. Patients often note that the cyst becomes larger after increased periods of activity and decreases in size with inactivity.Ganglion cysts tend to be self-limiting and do not typically continue to expand in size.If left untreated, ganglion cysts can persist for years. They may resolve or rupture spontaneously. One cannot predict how long that they will persist or if and when they will resolve.Resolution is far more common in the pediatric population.
GIANT CELL TUMORS
The lesion begins as a single nodule, becoming multinodular as it enlarges.Malignant transformation of giant cell tumor of the tendon sheath in the hand has not been reported.6
EPIDERMAL INCLUSION CYSTS
These lesions occur months to years after a traumatic event. They grow slowly to produce a painless mass, most commonly seen in the fingertip.Malignant transformation of these lesions in the hand has not been reported.12
PATIENT HISTORY AND PHYSICAL FINDINGS
GANGLION CYSTS


GIANT CELL TUMORS
Giant cell tumors are most common in the fourth to sixth decade, with a slight predominance in women.Patients typically present with a slow-growing, multilobulated, firm, painless mass present for several months to years.Lesions usually occur in the radial three digits of the hand on the volar surface. Dorsal involvement, particularly around the distal interphalangeal joint, is not uncommon.7These lesions are typically firmer than ganglion cysts and do not transilluminate.Large lesions may limit range of motion or result in neuropathic symptoms as a result of compression of digital nerves.Direct palpation typically reveals a firm, multinodular, nontender lesion.Loss of range of motion may occur when large lesions occur near the interphalangeal joints.Patients may have sensory deficits secondary to digital nerve compression. These can be revealed by testing two-point discrimination.
EPIDERMAL INCLUSION CYSTS
Epidermal inclusion cysts are more common in men than in women and occur in the third to fourth decade.2 Patients commonly present with a painless, slow-growing mass after a laceration, puncture wound, or traumatic amputation of the finger.2These lesions should be suspected in laborers who have a painless mass in the palm.12Erythematous and painful lesions have been reported. One study reported two cases mimicking a collar-button abscess resulting from rupture of the cyst in the palmar soft tissues.20These lesions are typically firmer than ganglion cysts and do not transilluminate. Direct palpation will reveal a lesion that is firm, nontender, superficial, and mobile.Loss of range of motion may occur when large lesions occur near the interphalangeal joints.Two-point discrimination testing may reveal sensory deficits secondary to digital nerve compression.
IMAGING AND OTHER DIAGNOSTIC STUDIES
GANGLION CYSTS
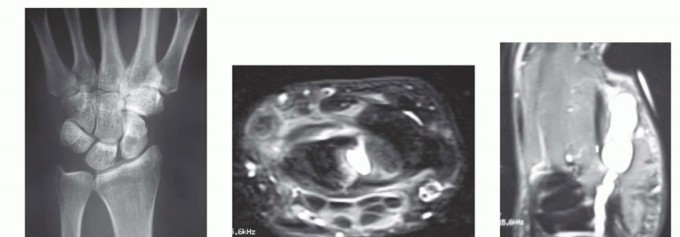
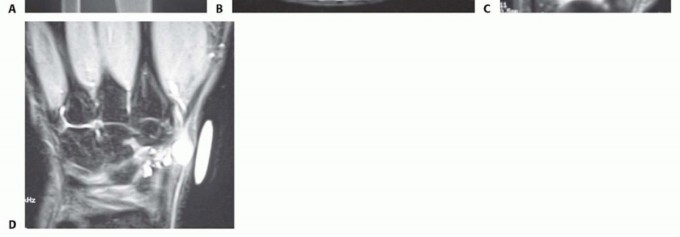
FIG 3 • A. Radiograph showing an intraosseous ganglion cyst within the scaphoid. B. MRI of a dorsal wrist ganglion cyst extending into the scapholunate joint. C. MRI of a ganglion cyst arising from the scaphotrapezial joint and extending into the thenar eminence. D. MRI of a ganglion cyst in the snuffbox but arising from the dorsal scapholunate ligament. MRI can also be used to better localize the site of origin as part of preoperative planning in ganglion cysts that occur in atypical locations (FIG 3C,D).Ultrasound can also be used to diagnose ganglion cysts, but this test is examiner dependent and lesssensitive and specific than MRI.Computed tomography (CT) scans are generally obtained only for preoperative planning to better localize and evaluate the bony architecture of intraosseous ganglion cysts.
GIANT CELL TUMORS
Plain radiographs show a soft tissue mass. Juxtacortical lesions may show bony erosion.MRI demonstrates a benign-appearing encapsulated mass, with decreased signal on T1- and T2-weighted images.
EPIDERMAL INCLUSION CYSTS
Plain radiographs show a soft tissue mass.A lytic lesion may be seen in the distal phalanx if it erodes into bone.
DIFFERENTIAL DIAGNOSIS
GANGLION CYSTS
Epidermoid inclusion cystGiant cell tumor of tendon sheath LipomaSynovial cyst
GIANT CELL TUMORS
Fibroma of the tendon sheath, synovial chondromatosis, synovial hemangioma, tophaceous gout, foreign body granuloma, periosteal chondroma
EPIDERMAL INCLUSION CYSTS
Tophaceous gout, foreign body granuloma, giant cell tumor, ganglion cyst, sebaceous cystBony destruction may mimic a malignant or infectious process.11 Some patients with these lesions have been treated with primary amputation before pathologic diagnosis.6
NONOPERATIVE MANAGEMENT
Of the three tumors discussed in this chapter, only ganglion cysts can be managed without surgery.Ganglion cysts are benign cysts that may resolve spontaneously. Treatment often depends on the level of a patient’s symptoms. Many patients seek medical care because they are concerned about the presence of asoft tissue mass and possibility of malignancy.21 Once a diagnosis of a ganglion cyst is made, with proper counseling as to the nature of these lesions, many patients will be satisfied with a course of observation.In patients who are symptomatic, typical nonoperative treatments include rest and immobilization, oral analgesics such as nonsteroidal anti-inflammatories and acetaminophen, and aspiration of the cyst with or without injection.3,13,14,21P.1315In wrist ganglion cysts, the results of aspiration have variable cure rates in the literature, ranging from 15% to89%.12 Various agents have been injected into the ganglion cyst after aspiration, including hyaluronidase and methylprednisolone.15On average, injection does not seem to increase the cure rate after aspiration, and we now typically perform aspiration alone. We generally inform patients that aspiration has about a 50% cure rate. The use ofsclerosing agents is frowned on because these agents may cause articular damage.10Traditional methods of traumatic rupture of the cyst from a direct blow with an object such as a large book (hence the termBible cyst) are mostly of historical significance.Ganglion cysts of tendon sheath (volar retinacular cysts) when symptomatic often respond to aspiration and injection and rarely require surgery when not associated with stenosing tenosynovitis. When they occur in association with stenosing tenosynovitis (trigger finger, de Quervain tendinitis), they often resolve with successful treatment of the underlying tendinitis.We typically do not aspirate ganglion cysts of tendon sheath but have had great success by injecting these cysts with local anesthetic and a small amount of corticosteroid (1.5 to 2 mL of 1% lidocaine and 10 mg of Depo-Medrol). The cyst is entered with a 25-gauge needle and then distended to the point of rupture. The remaining fluid in the syringe is then injected into the tendon sheath. If necessary, gentle digital massage can be used to rupture the cyst after injection if the cyst fails to rupture with distention.
SURGICAL MANAGEMENT
INDICATIONS
Ganglion CystsSurgery is generally indicated in patients who have symptoms and who either have failed nonoperative treatment or choose to proceed directly with surgery.In patients who have been diagnosed with a symptomatic wrist ganglion cyst, we generally describe the nature of the condition and outline the available forms of treatment, allowing the patient to decide which treatment is best for him or her. Some patients will choose observation, others will elect to undergo an aspiration, and some will chose to proceed directly with surgical excision.In the case of symptomatic ganglion cysts of tendon sheath, most of these will resolve with a corticosteroid injection and surgery is reserved for cysts that continue to recur.Degenerative mucous cysts that are draining or have a history of draining should be treated operatively because these cysts are at risk for infection that may extend into the distal interphalangeal joint and result in septic arthritis. If not draining, these cysts can be treated nonoperatively or surgically, depending on the patient’s symptoms and choice of treatment.Intraosseous ganglion cysts that are symptomatic or have resulted in pathologic fracture or may exhibit an impending pathologic fracture are often treated operatively.Giant Cell TumorsIndications for surgery include appearance, neuropathic symptoms, or loss of function. Careful, meticulous marginal excision of the lesion is the treatment of choice.Care must be taken to protect the neurovascular structures.Satellite lesions must be identified and carefully removed to minimize the chance of recurrence.Epidermal Inclusion CystsIndications for surgery include appearance, diagnosis, pain, and loss of function. Marginal excision of the lesion is the treatment of choice.
PREOPERATIVE PLANNING
Ganglion CystsWhen removing ganglion cysts arising in atypical locations, MRI studies can help to identify the cyst origin and plan appropriate surgical exposure.MRI and CT scans, along with plain radiographs, are valuable to determine the ideal exposure and for treating intraosseous ganglion cysts with curettage and bone grafting.Plain radiographs are reviewed before excising degenerative mucous cysts to determine the extent of underlying osteophytes that may need to be addressed.Giant Cell TumorsAlthough the diagnosis of giant cell tumor is primarily made based on history and clinical examination, radiographic studies should be reviewed to rule out other conditions.The patient should be advised that even with careful surgical techniques, the recurrence rate can be as high as 5% to 50%. Risk factors for local recurrence include proximity to the distal interphalangeal joint,degenerative joint disease, and bony erosion.16Temporary digital nerve neurapraxias may also occur after extrication of these tumors during surgery.Epidermal Inclusion CystsAlthough the diagnosis of epidermal inclusion cyst is primarily made based on history and clinical examination, radiographic studies should be reviewed to rule out other conditions.If a lytic lesion is present in the distal phalanx, a biopsy should be considered before surgical removal. The recurrence rate after marginal excision is low.
POSITIONING


FIG 4 • The patient is positioned supine with an arm board attached to the operating table and the upper extremity is prepared and draped in a standard manner. The surgeon is generally seated in the axilla with full access to the hand and wrist.
APPROACH
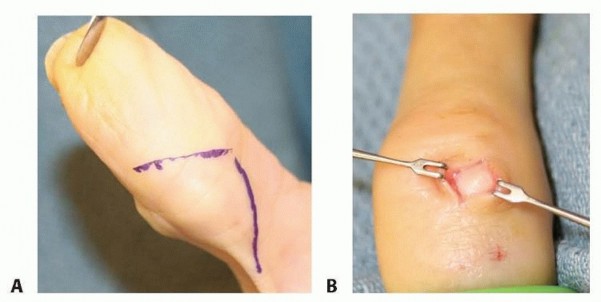



FIG 5 • A. A Brunner incision is made for a volar multilobular mass. B. A dorsal epidermal inclusion cyst is approached through a small longitudinal incision directly over the lesion.
TECHNIQUE
Open Excision of a Dorsal Wrist Ganglion Cyst
The location of the cyst is typically dorsal to the scapholunate interosseous ligament. The incision needs to provide access to this ligament. The scapholunate ligament is found just distal to the tubercle of Lister in the third and fourth extensor compartment interval (TECH FIG 1A).
TECH FIG 1•A.The dorsal scapholunate ligament is found just distal to the tubercle of Lister.EPL, extensor pollicis longus.B.Dorsal ganglion cysts typically arise from the dorsal scapholunate ligament.
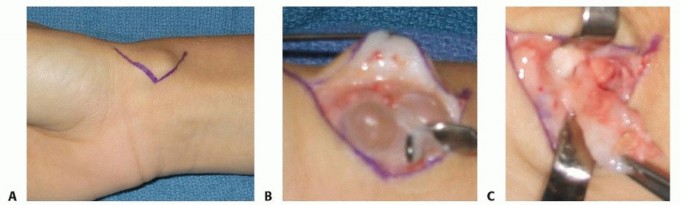
Open Excision of a Dorsal Wrist Ganglion Cyst C. The extensor retinaculum is incised transversely. D. The extensor tendons are retracted, allowing visualization of the cyst. E. Cyst stalk arising from the dorsal scapholunate ligament.(continued)

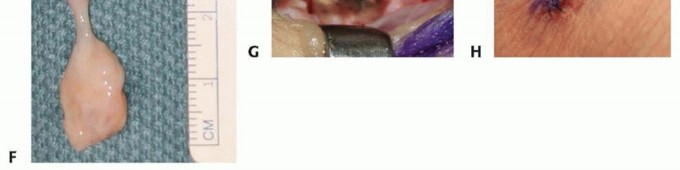
TECH FIG 1 •(continued)F. Excised cyst and stalk. G. The area of origin of the cyst is cauterized, taking care to preserve the ligament and interosseous membrane. H. Closure with running subcuticular suture.
TECH FIG 2 • A. A Brunner type of incision allows for more exposure and avoids contracture associated with straight longitudinal incisions in this location. B. A volar cyst adherent to the radial artery and venae comitantes. C. A volar wrist ganglion stalk arising from the volar radiocarpal ligaments.


TECH FIG 3 • A. Degenerative mucous cyst in the eponychial region resulting in nail plate deformity. B. Aggressive dissection is avoided distally to protect the nail germinal matrix. The cyst is traced proximally to its origin at the distal interphalangeal joint. C. The cyst is excised along with a portion of the joint capsule at its point of origin between the central tendon and collateral ligament. D. A rongeur is used to débride underlying osteophytes.

TECH FIG 4 • Standard arthroscopic setup using a traction tower. The traction tower, which can be sterilized, is typically positioned in this manner on a hand table after standard preparation and draping.


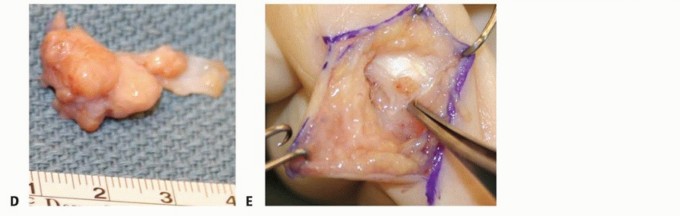
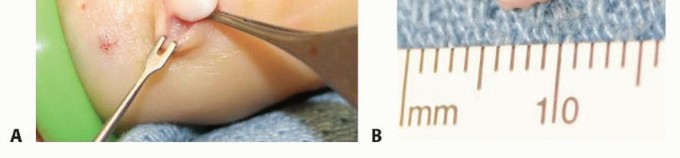
TECH FIG 5 • A. Careful surgical dissection of the subcutaneous tissues through a Brunner incision. B. The digital nerve is identified distal to the lesion and protected throughout the procedure. C. The tumor should be carefully removed from surrounding soft tissues. D. Excision demonstrates a firm, multinodular lesion. E. Any satellite lesions should be carefully identified and removed. Carefully examine the local tissues for satellite lesions, which may be only a few millimeters in size. These lesions need to be completely excised (TECH FIG 5E).If the extensor tendon is involved, surgical excision of a portion of the tendon may be required. In rare cases, tendon reconstruction may be necessary. Lesions eroding into bone may require local curettage.If the tumor appears to arise from an underlying joint, it is important to perform a capsulotomy to inspect the joint and débride any pigmented tissue.11Arthrodesis of the distal interphalangeal joint may be necessary to completely excise some lesions.7. Marginal Excision of an Epidermal Inclusion CystCareful surgical dissection is undertaken under loupe magnification.After initial exposure, isolate the neurovascular bundles in the area of the lesion.Once the capsule is identified, it can be sharply dissected from overlying skin and bluntly dissected from deeper soft tissues (TECH FIG 6). TECH FIG 6 • A. Through a small longitudinal incision directly over the lesion, the cyst is bluntly excised from surrounding soft tissues. B. Excision of the lesion demonstrates a firm, white, encapsulated mass. Take care to remove the entire capsule.Lesions eroding into bone may require local curettage and bone graft.In rare cases with advanced bony destruction, amputation is an alternative.P.1321
PEARLS AND PITFALLS

POSTOPERATIVE CARE
GANGLION CYSTS OF THE WRIST
The splint and sutures are removed about 1 week postoperatively and Steri-Strips applied to the wound.Range-of-motion exercises and light use of the hand are initiated at 1 week, with gradual advancement of activities as tolerated.Scar massage is encouraged at 2 weeks. Ganglion Cyst of Tendon Sheath and Degenerative Mucous Cyst Patients are instructed to remove their postoperative dressing 4 to 5 days after surgery. We prefer to have the patients clean their wound at least twice daily with antibacterial soap and water. The wound is redressed with light gauze or an adhesive bandage.Sutures are generally removed at 1 week and Steri-Strips applied to the wound.Range-of-motion exercises and light use of the hand are initiated, with gradual advancement of activities as tolerated.Scar massage is encouraged at 2 weeks.
INTRAOSSEOUS GANGLION CYSTS
Postoperative dressing and sutures are removed at 1 week and Steri-Strips applied to the wound.We generally apply a short-arm cast for 3 to 5 weeks. The cast is removed and range-of-motion exercises and light hand use are initiated.Incorporation of the bone graft is monitored with use of serial radiographs. If the intraosseous ganglion cyst has weakened the bone, a protective splint may be used once the cast is removed until incorporation of the bone graft. Giant Cell Tumors and Epidermal Inclusion Cysts Patients should be instructed about the high rate of recurrence of giant cell tumors.Range-of-motion exercises and antiedema techniques should be started immediately after surgery.Sutures can be removed at 8 to 10 days.
OUTCOMES
GANGLION CYSTS
Symptomatic relief is often accomplished after excision of most ganglion cysts.Recurrence rates after ganglion cyst surgery have been reported to range from 4% to 40%.18 With adherence to the preceding principles, however, the recurrence rate in our experience is less than 5%.Complications of ganglion cyst removal are infrequent.The recurrence rate of giant cell tumors has varied from 5% to 50%. The high rate of recurrence is due to incomplete excision or satellite lesions.6Recurrence rates are even higher after excision of a recurrent tumor.16In contrast, the recurrence rate after epidermal inclusion cyst excision, even with bony involvement, is low.P.1322
COMPLICATIONS
Wound complications (eg, painful or unsightly scar), infection, digital neurapraxia, or recurrence can occur.Ganglion cyst excision can result in a neurovascular injury. This complication is rare with adherence to good surgical technique and a good understanding of the local anatomy. Volar wrist ganglion cysts are adherent to the radial artery and can be difficult to dissect free from the artery. If necessary, a cuff of the cyst is left attached to the artery. If injury to the artery does occur, a repair should be performed.Stiffness is a complication of ganglion cyst excision. Avoiding direct capsular closure reduces the risk of this complication.Complications associated with degenerative mucous cysts include extensor lag, joint stiffness, infection, nail plate deformity, and distal interphalangeal joint deformity.5
REFERENCES
- Angelides AC. Ganglions of the hand and wrist. In: Green DP, Hotchkiss RN, Pederson WC, eds. Operative Hand Surgery, vol 2, ed 4. New York: Churchill Livingstone, 1999:2171-2183.
- Athanasian EA. Bone and soft tissue tumors. In: Green DP, Hotchkiss RN, Pederson WC, et al, eds. Operative Hand Surgery, vol 2, ed 5. New York: Churchill Livingstone, 2005:2211-2264.
- Burge P. Aspiration of ganglia. J Hand Surg Br 1993;18(3):409-410.
- Dodge LD, Brown RL, Niebauer JJ, et al. The treatment of mucous cysts: long-term follow-up in sixty-two cases. J Hand Surg Am 1984;9(6):901-904.
- Fritz GR, Stern PJ, Dickey M. Complications following mucous cyst excision. J Hand Surg Br 1997;22(2):222-225.
- Glowacki KA. Giant cell tumors of the tendon sheath. J Am Soc Surg Hand 2003;3:100-107.
- Glowacki KA, Weiss AP. Giant cell tumor of the tendon sheath. Hand Clin 1995;11(2):245-253.
- Greendyke SD, Wilson M, Shepler TR. Anterior wrist ganglia from the scaphotrapezial joint. J Hand Surg Am 1992;17(3):487-490.
- Lister GD, Smith RR. Protection of the radial artery in the resection of adherent ganglions of the wrist. Plast Reconstr Surg 1978;61: 127-129.
- Mackie IG, Howard CB, Wilkins P. The dangers of sclerotherapy in the treatment of ganglia. J Hand Surg Br 1984;9(2):181-184.
- Moore JR, Weiland AJ, Curtis RM. Localized nodular tenosynovitis: experience with 115 cases. J Hand Surg Am 1982;9(3):412-417.
- Nahra ME, Bucchieri JS. Ganglion cysts and other tumor related conditions of the hand and wrist. Hand Clin 2004;20:249-260.
- Nield DV, Evans DM. Aspiration of ganglia. J Hand Surg Br 1986;11(2):264.
- Oni JA. Treatment of ganglia by aspiration alone. J Hand Surg Br 1992;17(6):660.
- Paul AS, Sochart DH. Improving the results of ganglion aspiration by the use of hyaluronidase. J Hand Surg Br 1997;22(2):219-221.
- Reilly KE, Stern PJ, Dale A. Recurrent giant cell tumors of the tendon sheath. J Hand Surg Am 1999;24(6):1298-1302.
- Rizzo M, Berger RA, Steinman SP, et al. Arthroscopic resection in the management of dorsal wrist ganglions: results with a minimum 2-year follow-up period. J Hand Surg Am 2004;29(1):59-62.
- Thornburg LE. Ganglions of the hand and wrist. J Am Acad Orthop Surg 1999;7:231-238.
- Wang AA, Hutchinson DT. Longitudinal observation of pediatric hand and wrist ganglia. J Hand Surg Am 2001;26(4):599-602.
- Ward WA, Labosky DA. Ruptured epidermal inclusion cyst in the palm presenting as a collar-button abscess. J Hand Surg Am 1985;10(6 pt 1):899-901.
- Zubowicz VN, Ishii CH. Management of ganglion cysts of the hand by simple aspiration. J Hand Surg Am 1987;12(4):618-620.
SUGGESTED READINGS
Soren A. Pathogenesis and treatment of ganglion. Clin Orthop Relat Res 1996;48:173-179.Westbrook AP, Stephen AB, Oni J, et al. Ganglia: the patient’s perception. J Hand Surg Br 2000;25(6):566-567.
