Comprehensive Introduction and Patho-Epidemiology
Midfoot amputations represent a critical, highly nuanced juncture in lower extremity limb salvage, offering a functional, energy-preserving alternative to below-knee amputations (BKA) for patients suffering from severe trauma, intractable infection, ischemia, or advanced Charcot neuroarthropathy. The preservation of the native knee joint and a weight-bearing heel pad profoundly impacts the patient’s postoperative ambulatory capacity, metabolic energy expenditure, and overall quality of life. Amputations through the middle of the foot primarily include the transmetatarsal amputation (TMA), the Lisfranc amputation (at the tarsometatarsal joints), the Chopart amputation (at the transverse tarsal joints), and the historically significant Pirogoff amputation. Historically, midfoot disarticulations were developed during the Napoleonic wars for rapid management of battlefield crush injuries and frostbite. Today, the epidemiology has shifted dramatically, with the vast majority of these procedures performed in the setting of diabetic foot complications and peripheral arterial disease (PAD).
The pathophysiology driving the need for midfoot amputations is largely dominated by the triad of neuropathy, ischemia, and altered biomechanics, particularly in the diabetic population. Progressive collapse of the midfoot and hindfoot, often accompanied by a profound loss of bony architecture, is a hallmark of Charcot arthropathy in elderly patients with diabetes mellitus. This neurogenic destruction of the osseous and ligamentous architecture leads to a "rocker-bottom" deformity, which subsequently causes focal pressure points that the insensate foot cannot detect. Deep plantar space abscesses, osteomyelitis, or neuropathic periostitis frequently follow this collapse deformity, leading to recalcitrant ulceration that threatens the entire limb. In these scenarios, ablative surgery must be meticulously balanced with limb salvage principles to eradicate infection while preserving maximal functional length.
While midfoot procedures preserve the heel pad and allow for direct end-bearing, they fundamentally alter the biomechanics of the lower extremity. The loss of the anterior lever arm, combined with the sacrifice of key dorsiflexor insertions, creates a profound muscle imbalance. This is not merely a theoretical concern; it is the primary reason midfoot amputations historically fell out of favor. If this biomechanical disruption is not meticulously addressed during the index procedure through aggressive tendon balancing and soft tissue management, the imbalance inevitably leads to severe equinus or equinovarus deformities. These deformities result in anterior stump ulceration, intractable pain, and eventual failure requiring proximal revision to a Syme or transtibial level.
The decision to proceed with a midfoot amputation over a more proximal level requires a sophisticated understanding of the patient's vascular status, ambulatory potential, and the local soft tissue envelope. The metabolic cost of walking increases inversely with the length of the preserved limb. A patient with a well-balanced Chopart or Lisfranc amputation will expend approximately 10% to 15% more energy during ambulation compared to a non-amputee, whereas a transtibial amputee may expend 25% to 40% more energy. In a vasculopathic or elderly patient with compromised cardiopulmonary reserve, this difference in energy expenditure can mean the difference between independent community ambulation and permanent wheelchair reliance. Therefore, mastering the intricacies of midfoot amputations is an essential competency for the modern orthopedic and limb salvage surgeon.
Detailed Surgical Anatomy and Biomechanics
The surgical anatomy of the midfoot is an intricate confluence of osseous keystones, robust ligamentous complexes, and dynamic tendinous insertions that collectively maintain the longitudinal and transverse arches of the foot. The Lisfranc joint complex, or tarsometatarsal articulation, involves the articulations between the three cuneiforms and the cuboid proximally, and the bases of the five metatarsals distally. The base of the second metatarsal is recessed proximally between the medial and lateral cuneiforms, creating a rigid osseous keystone that provides inherent stability to the midfoot. The transverse tarsal joint, or Chopart's joint, consists of the talonavicular and calcaneocuboid articulations. This joint line represents the functional division between the hindfoot and the midfoot and is the site of the Chopart disarticulation, leaving only the talus and calcaneus as the remaining osseous structures of the foot.
The primary biomechanical challenge in midfoot amputations is the preservation of a plantigrade, braceable stump in the face of massive musculotendinous disruption. The normal foot functions as a complex, dynamic lever system during the stance phase of gait. Amputating distal to the transverse tarsal or tarsometatarsal joints removes the distal insertion points of the anterior tibial tendon (medial cuneiform and first metatarsal base), the extensor hallucis longus (EHL), the extensor digitorum longus (EDL), the peroneus brevis (fifth metatarsal base), and the peroneus longus (medial cuneiform and first metatarsal base). The loss of these crucial dorsiflexors and evertors creates an immediate, profound mechanical disadvantage.
Consequently, the powerful triceps surae complex (gastrocnemius and soleus), acting through the Achilles tendon, is left completely unopposed. This unopposed plantarflexion force rapidly drives the hindfoot into a rigid equinus deformity. Furthermore, the unopposed pull of the tibialis posterior (which inserts broadly across the navicular, cuneiforms, and cuboid) can introduce a severe varus component. This combination results in a rigid equinovarus posture where the patient is forced to bear weight on the vulnerable, thinly padded anterolateral aspect of the distal stump, rather than the robust, specialized glabrous skin of the plantar heel pad. This abnormal weight-bearing inevitably leads to skin breakdown, recurrent ulceration, osteomyelitis, and amputation failure.
To counteract this predictable and devastating biomechanical cascade, the orthopedic surgeon must intervene surgically to restore equilibrium. To prevent equinus deformity after midfoot amputations, two critical biomechanical interventions are mandatory: the transfer of one or more dorsiflexors of the ankle to the remaining tarsal bones to restore active dorsiflexion, and the absolute weakening of the plantarflexors. A simple Z-lengthening of the Achilles tendon is often insufficient in the setting of a midfoot amputation, as the tendon frequently heals and re-tethers, leading to recurrent equinus. Tenectomy of the Achilles tendon—involving the frank removal of 2 to 3 cm of the tendon—is strongly recommended to permanently de-tension the posterior lever arm and neutralize the deforming forces.
Exhaustive Indications and Contraindications
The selection of the appropriate amputation level is a complex clinical decision that must synthesize the extent of tissue necrosis, the presence of infection, the patient's vascular perfusion, and their baseline functional status. Midfoot amputations are primarily indicated for patients with gangrene, severe trauma, or recalcitrant osteomyelitis that involves the toes and distal metatarsals but spares the proximal midfoot and hindfoot heel pad. The overarching goal is to excise all non-viable and infected tissue while preserving the maximal functional length of the limb. A robust, well-vascularized plantar flap is the absolute prerequisite for any midfoot amputation; without it, the procedure is doomed to failure.
Vascular assessment is paramount in determining the viability of a midfoot amputation. Clinical palpation of pulses is insufficient. Non-invasive vascular studies, including Ankle-Brachial Indices (ABI), toe pressures, and transcutaneous oxygen tension (TcPO2), are required. Generally, an ABI greater than 0.45, an absolute toe pressure greater than 30 mm Hg, and a TcPO2 greater than 30 to 40 mm Hg are considered the minimum thresholds for predictable healing of a midfoot amputation in a diabetic patient. If these parameters are not met, formal angiography and potential endovascular or open surgical revascularization must be pursued prior to, or in conjunction with, the amputation.
Contraindications to midfoot amputations can be absolute or relative. Absolute contraindications include extensive ischemic necrosis or deep space infection extending into the plantar heel pad, inadequate arterial perfusion that cannot be bypassed or reconstructed, and profound, uncorrectable malnutrition (e.g., serum albumin < 2.5 g/dL). Relative contraindications include profound sensory neuropathy in a non-compliant patient who will not adhere to postoperative offloading and prosthetic wear, as this will inevitably lead to stump ulceration. Furthermore, a patient with a fixed, uncorrectable equinus contracture that cannot be managed with Achilles tenectomy may be better served with a more proximal amputation level to ensure a braceable stump.
Indications and Contraindications Summary Table
| Parameter | Transmetatarsal Amputation (TMA) | Lisfranc Disarticulation | Chopart Disarticulation |
|---|---|---|---|
| Primary Indication | Distal gangrene/infection sparing the metatarsal bases. Crush injury to digits/distal metatarsals. | Trauma strictly localized to the metatarsals. Rarely used for ischemic disease due to high failure rates. | Extensive midfoot trauma or infection sparing the talus, calcaneus, and heel pad. |
| Vascular Requirement | TcPO2 > 30 mmHg at mid-foot level. Palpable or Dopplerable pedal pulses. | TcPO2 > 30-40 mmHg at the mid-tarsal level. | TcPO2 > 30-40 mmHg at the hindfoot level. Robust posterior tibial artery flow. |
| Biomechanical Consequence | Loss of toe-off phase. Mild equinus risk. | Loss of anterior lever arm. High risk of severe equinovarus deformity. | Complete loss of anterior lever arm. Extreme risk of equinovarus and talar plantarflexion. |
| Required Tendon Transfer | Achilles lengthening often sufficient. Tibialis anterior usually preserved natively. | Achilles tenectomy. Tibialis anterior transfer to midfoot. | Radical Achilles tenectomy. Tibialis anterior to talar neck. Peroneus brevis to calcaneus. |
| Absolute Contraindication | Plantar flap necrosis extending proximal to metatarsal heads. | Infection/gangrene involving the cuneiforms or cuboid. | Heel pad necrosis. Osteomyelitis of the talus or calcaneus. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful midfoot amputation. The process begins with a comprehensive medical optimization of the patient. Glycemic control must be strictly managed, aiming for perioperative blood glucose levels between 140 and 180 mg/dL to optimize leukocyte function and wound healing. Nutritional status must be evaluated; a total lymphocyte count (TLC) greater than 1500/mm³ and serum albumin greater than 3.0 g/dL are associated with significantly higher rates of primary wound healing. Any active infection must be aggressively managed with broad-spectrum intravenous antibiotics, tailored to deep tissue cultures, prior to definitive closure.
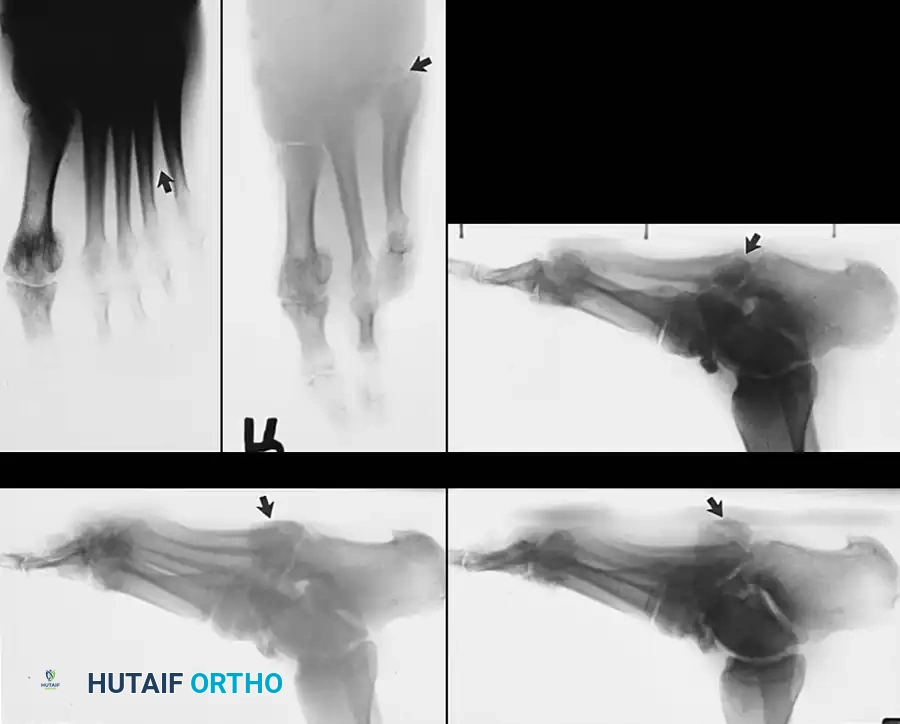
Advanced imaging is crucial for surgical templating. While plain weight-bearing radiographs are standard for assessing global foot architecture and obvious osteomyelitis, Magnetic Resonance Imaging (MRI) with and without contrast is the gold standard for defining the proximal extent of marrow edema, osteomyelitis, and deep soft tissue abscesses. In cases of severe Charcot arthropathy where bone stock is highly distorted, a non-contrast Computed Tomography (CT) scan with 3D reconstructions can be invaluable for planning the precise level of osteotomies and anticipating the required bony resections to achieve a congruent, tension-free closure. The surgeon must meticulously map the viable soft tissue envelope, ensuring that the planned plantar flap is free of infection and possesses adequate perfusion.
Patient positioning is critical for optimal surgical exposure and intraoperative efficiency. The patient is placed in the supine position on a radiolucent operating table to facilitate intraoperative fluoroscopy. A bump is placed under the ipsilateral hip to internally rotate the leg, bringing the foot into a neutral, upward-facing position, which greatly assists in addressing the lateral column and performing the Achilles tenectomy. A well-padded thigh tourniquet is applied; however, its use is highly controversial and generally contraindicated in patients with severe peripheral arterial disease or calcified vessels, as tourniquet inflation can cause plaque rupture, acute thrombosis, or profound ischemic reperfusion injury to the already compromised distal flaps. In such cases, the procedure is performed without a tourniquet, relying on meticulous hemostasis.
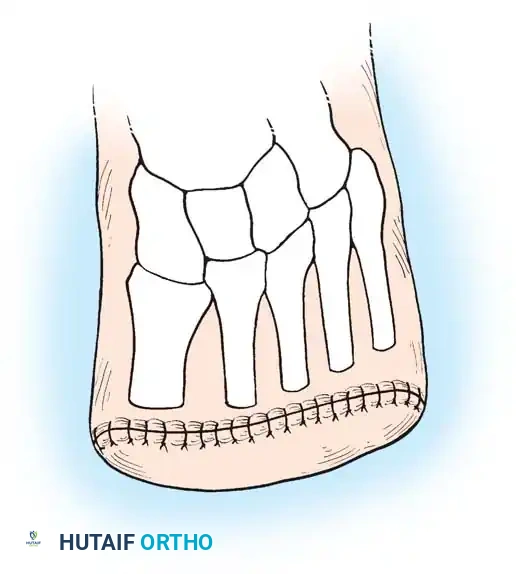
Skin incisions must be templated and marked prior to the incision, utilizing a sterile surgical marker. The golden rule of midfoot amputations is to maximize the length of the plantar flap, as the specialized glabrous skin of the sole is uniquely designed to withstand the shear and compressive forces of weight-bearing. The dorsal incision is typically kept short, just distal to the planned bone cuts, while the plantar incision extends significantly further distally before curving proximally to meet the dorsal incision. This "fish-mouth" design, heavily biased toward the plantar surface, ensures that the final suture line rests dorsally, completely away from the weight-bearing surface of the distal stump.
Step-by-Step Surgical Approach and Fixation Technique
The surgical execution of midfoot amputations requires meticulous soft tissue handling, precise osteotomies, and aggressive biomechanical rebalancing. While slightly distal to the true midfoot disarticulations, the transmetatarsal amputation (TMA) shares similar biomechanical principles and is often the preferred initial salvage procedure before progressing to a Lisfranc or Chopart level.
Transmetatarsal Amputation (TMA) Principles
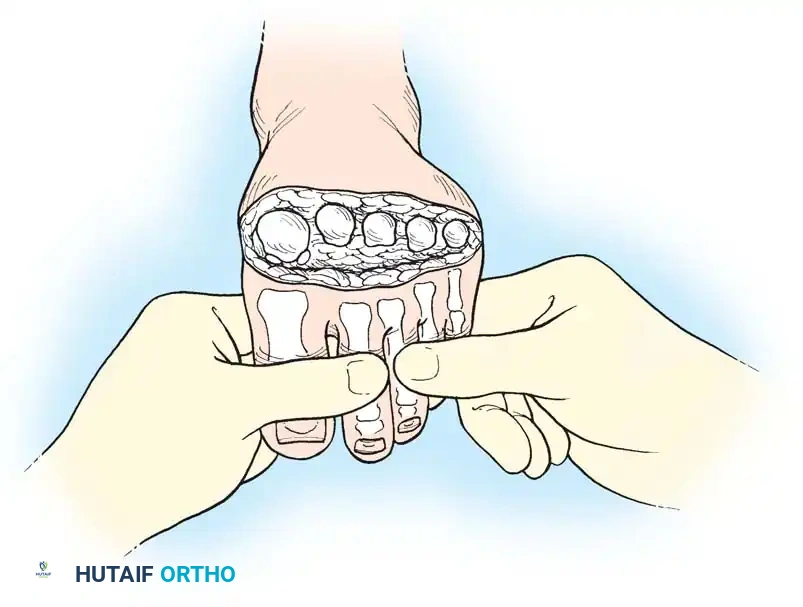
The success of a TMA relies heavily on the creation of a robust, well-vascularized plantar flap. The dorsal incision is made straight across the mid-metatarsal shafts, while the plantar incision extends distally to the metatarsal necks before curving proximally.
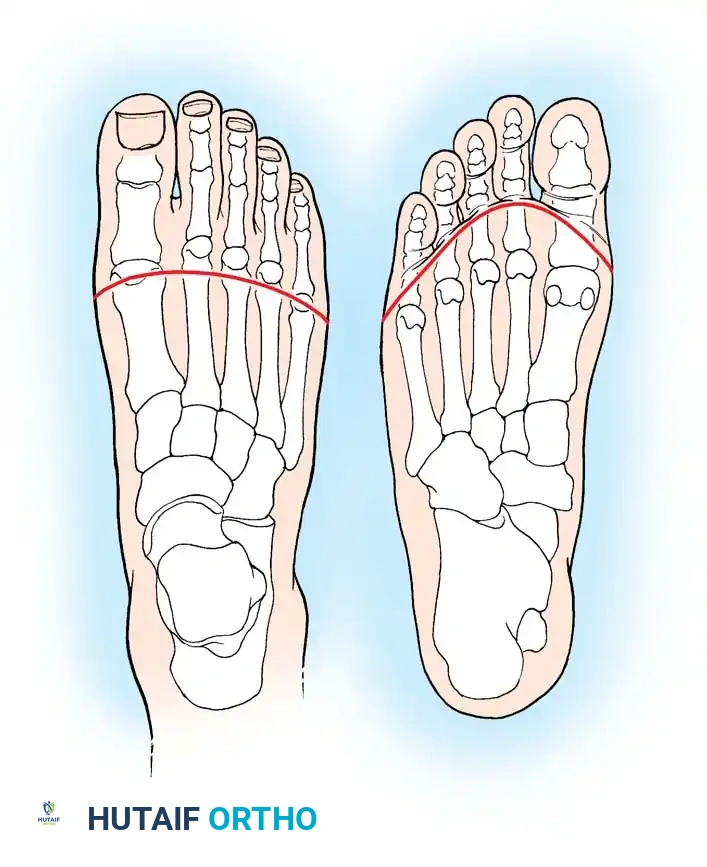
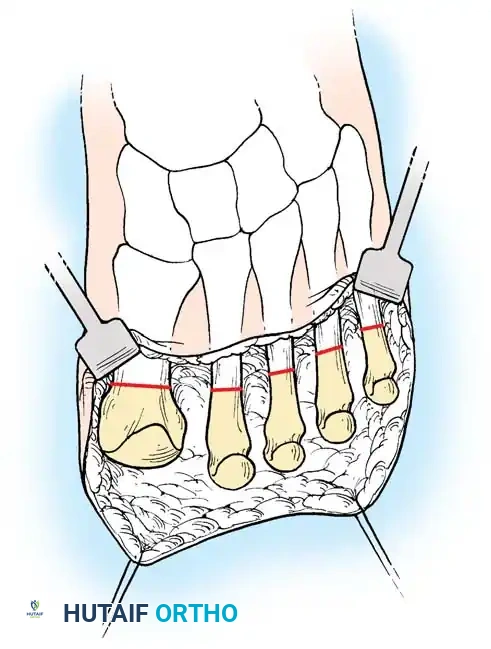
When performing the bone cuts, the level of bone transection must be carefully planned. The osteotomy locations should form a gentle, cascading curve, mimicking the natural transverse arch of the foot. The first metatarsal is left the longest, and each subsequent lateral metatarsal is cut slightly shorter and more proximal than the one medial to it. Crucially, the plantar aspect of each metatarsal stump must be beveled dorsally to prevent prominent bony spikes from creating pressure points against the plantar flap during weight-bearing.
Meticulous soft-tissue handling is paramount during closure. The thick plantar flap, containing the plantar fascia and intrinsic musculature, is brought dorsally to cover the metatarsal stumps. Closure should be performed in a single layer using monofilament nonabsorbable sutures (e.g., 3-0 nylon) to minimize tissue reactivity and ischemia at the wound edges. Deep, multi-layer closures are avoided as they can strangulate the delicate subdermal vascular plexus of the ischemic flap.
The Lisfranc Amputation
The Lisfranc amputation involves disarticulation precisely at the tarsometatarsal joints. Historically, this procedure has seldom been performed as a standalone definitive amputation because of the extraordinarily high incidence of equinus deformity that usually develops, which is frequently followed by a severe, unbraceable equinovarus deformity. The surgical approach involves a dorsal incision directly over the TMT joints and a long plantar flap extending to the metatarsal heads. The disarticulation requires sharp division of the robust Lisfranc ligament connecting the medial cuneiform to the base of the second metatarsal. When a Lisfranc amputation is deemed absolutely necessary, it must be accompanied by the same aggressive tendon balancing techniques utilized in the Chopart amputation, including a radical Achilles tenectomy and the transfer of the tibialis anterior to the midfoot (usually the medial cuneiform or navicular) to maintain a plantigrade posture.
The Chopart Amputation (Technique 10-7)
The Chopart amputation is a disarticulation through the transverse tarsal joints (the talonavicular and calcaneocuboid joints). It preserves only the talus and calcaneus, providing an excellent, durable heel pad for weight-bearing. However, it requires the most meticulous surgical technique to prevent the talus from plantarflexing out of the ankle mortise.
Incision and Soft Tissue Management: The skin incision is marked preoperatively, creating a "fish-mouth" flap that is significantly longer on the plantar surface. The incision begins at the transtarsal joints medially and laterally, extending sharply through the skin and subcutaneous tissue. A critical step is nerve management. The superficial peroneal, deep peroneal, sural, and saphenous nerves must be identified, placed under gentle distal traction, transected sharply, and allowed to retract deep into the proximal soft tissue bed. This traction neurectomy is vital to prevent the formation of painful, superficial neuromas at the weight-bearing stump interface. The extensor digitorum longus (EDL) and extensor hallucis longus (EHL) tendons are transected and allowed to retract.
Disarticulation and Bone Preparation: The transverse tarsal joints are identified, and the midfoot is disarticulated by systematically releasing the dorsal, lateral, medial, and plantar ligaments, including the bifurcate ligament and the spring ligament. While some surgeons prefer to leave the articular cartilage intact, best practice often involves shaving the cartilage off the head of the talus and the anterior process of the calcaneus. This promotes soft-tissue adherence, reduces synovial fluid production, and prepares a bleeding bone bed for tendon transfers.
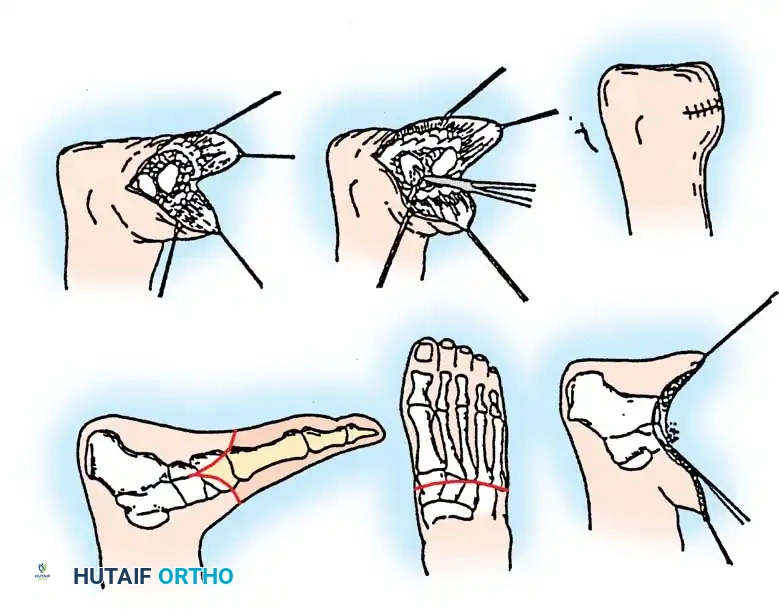
Biomechanical Rebalancing: This is the most critical phase. Make a separate longitudinal posteromedial incision over the distal Achilles tendon. Perform a radical tenectomy, excising a full 2 to 3 cm of the tendon to completely abolish its plantarflexion force. Attempt to preserve the paratenon to aid in organized hematoma formation. Next, transfer the preserved anterior tibial tendon to the neck of the talus. This is achieved by drilling a tunnel through the talar neck or creating a bony trough and securing the tendon with heavy nonabsorbable suture or bone anchors. Advanced balancing often requires transferring the peroneus brevis to the anterior process of the calcaneus to restore eversion balance and counteract the varus pull of the posterior tibial tendon. The wound is then thoroughly irrigated and closed in a single layer with interrupted nonabsorbable monofilament sutures, avoiding any tension that could compromise flap perfusion.
Complications, Incidence Rates, and Salvage Management
Despite meticulous surgical technique, midfoot amputations carry a high risk of complications, particularly in the dysvascular and diabetic populations. The most frequent and devastating complications are wound dehiscence, ischemic necrosis of the distal flap, and the development of fixed equinus or equinovarus deformities. Wound healing complications occur in approximately 20% to 40% of cases, often necessitating prolonged local wound care, negative pressure wound therapy (NPWT), or return to the operating room for debridement and proximal revision.
The biomechanical failure of a midfoot amputation—manifesting as a rigid equinus deformity—is the primary reason these procedures fail in the long term. When the Achilles tendon overpowers the weakened or absent dorsiflexors, the anterior aspect of the distal stump is driven into the floor during the stance phase of gait. This creates massive shear forces and pressure on the thin anterior skin, rapidly leading to ulceration, deep space infection, and osteomyelitis of the remaining tarsal bones.
Complications and Management Strategies
| Complication | Estimated Incidence | Etiology | Prevention and Salvage Management |
|---|---|---|---|
| Wound Dehiscence / Ischemic Necrosis | 20% - 40% | Inadequate arterial perfusion, excessive closure tension, multi-layer suturing strangulating tissue. | Prevention: Pre-op vascular optimization (TcPO2 > 30). Single-layer closure. Management: NPWT, strict offloading. If necrosis is deep, revision to proximal level (Syme or BKA) is required. |
| Equinus Deformity | 30% - 50% (if unaddressed) | Unopposed pull of the triceps surae complex due to loss of anterior lever arm and dorsiflexors. | Prevention: Radical Achilles tenectomy (excise 2-3 cm) at index surgery. Management: Salvage tenectomy and serial casting (Burgess technique). |
| Equinovarus Deformity | 15% - 25% | Unopposed pull of Tibialis Posterior and Achilles; failure to transfer peroneals. | Prevention: Transfer Peroneus Brevis to calcaneus; Tibialis Anterior to talus. Management: Soft tissue releases, split anterior tibial tendon transfer (STATT), or revision amputation. |
| Painful Neuroma | 5% - 10% | Failure to adequately resect and bury superficial sensory nerves during index procedure. | Prevention: Aggressive traction neurectomy of deep/superficial peroneal, sural, and saphenous nerves. Management: Surgical excision of neuroma and proximal burying into muscle belly. |
Salvage of the Equinus Stump: In cases where a tarsometatarsal or midtarsal amputation was previously performed without adequate tendon balancing, a fixed equinus deformity frequently develops. The patient presents with severe pain, skin breakdown, and pressure irritation over the distal anterior stump. To salvage these failing amputations, a straightforward but highly effective intervention, popularized by Burgess and Lieberman, is recommended. The surgeon performs a radical division (tenectomy) of the Achilles tendon through a small posterior incision. The equinus deformity is manually corrected, forcefully dorsiflexing the remaining foot. The limb is then placed in a rigid dressing (cast) in slight dorsiflexion for 6 weeks. By this means, the equinus is corrected, and weight is borne—as it biomechanically should be—on the thick plantar skin of the heel. Recurrence of the equinus deformity following this salvage procedure has not been a significant problem, and it effectively eliminates the pressure irritation associated with excessive weight on the end of the stump.
Phased Post-Operative Rehabilitation Protocols
The postoperative management and rehabilitation protocol following a midfoot amputation is as critical to the ultimate success of the limb salvage effort as the surgical execution itself. Premature weight-bearing, inadequate immobilization, or non-compliance with the rehabilitation timeline will inevitably lead to catastrophic failure of the tendon transfers, wound dehiscence, and recurrent deformity. The rehabilitation process must be rigidly structured and divided into distinct, carefully monitored phases.
Phase I: Immediate Postoperative Immobilization (Weeks 0-2)
Immediately following wound closure in the operating room, the limb must be placed in a well-padded, rigid dressing or a short leg cast. The stump must be held in neutral to slight dorsiflexion. This positioning is critical; it prevents the immediate onset of equinus contracture and removes all tension from the anterior tendon transfers (e.g., tibialis anterior to the talar neck). The patient is made strictly non-weight-bearing (NWB) on the operative extremity. Elevation of the limb above the level of the heart is mandatory to reduce postoperative edema, which can compromise the tenuous microvascular perfusion of the distal flaps.
Phase II: Wound Healing and Suture Removal (Weeks 2-6)
The initial rigid dressing is typically changed at 10 to 14 days postoperatively to inspect the wound. In dysvascular patients, wound healing is significantly delayed. Sutures must be kept in place for an extended period, typically 4 to 6 weeks, to allow for adequate healing of the potentially compromised distal soft tissues. Premature suture removal is a common error that leads to disastrous wound dehiscence. Following the wound check, the patient is recast in slight dorsiflexion and remains strictly NWB. This prolonged immobilization is necessary not only for skin healing but to allow the Achilles tenectomy site to fill with stable, elongated fibrous scar tissue, permanently lengthening the posterior lever arm.
Phase III: Tendon Incorporation and Transition (Weeks 6-8)
By 6 to 8 weeks, solid bony incorporation of the transferred ankle dorsiflexors should be occurring. The cast is removed, and clinical assessment of the stump is performed. If the wound is completely healed and the tendon transfers appear intact (demonstrating active, albeit weak, dorsiflexion), the patient may be transitioned to a removable controlled ankle motion (CAM) boot. Weight-bearing is initiated very gradually, starting with touch-down weight-bearing and progressing to partial weight-bearing under the strict guidance of physical therapy. Edema control remains vital, often requiring the use of custom compressive shrinker socks.
Phase IV: Definitive Prosthetics and Return to Function (Weeks 8+)
Once fully healed and the stump volume has stabilized, the patient is fitted with a specialized definitive prosthesis. The biomechanics of the Chopart and Lisfranc amputations require specific orthotic support to prevent late-onset deformities and protect the distal stump. For a Chopart amputation, this typically involves a custom-molded ankle-foot orthosis (AFO) or a clamshell prosthesis. The prosthesis must feature a rigid sole to prevent bending at the midfoot, a rocker-bottom modification to simulate the lost "toe-off" phase of the gait cycle, and a custom molded toe filler. The toe filler prevents the stump from pistoning or sliding forward within the shoe, which would cause devastating shear injuries to the distal soft tissue envelope.
Summary of Landmark Literature and Clinical Guidelines
The modern approach to midfoot amputations is built upon a foundation of landmark orthopedic literature that systematically identified the causes of historical failures and proposed the biomechanical solutions we rely on today. Historically, midfoot amputations were viewed with extreme skepticism due to the near-universal complication of equinovarus deformity.
The paradigm shift in the management of these amputations can be traced to the seminal work of Burgess and Lieberman, who clearly elucidated the biomechanical necessity of the Achilles tenectomy. Their research demonstrated that simple lengthening of the Achilles tendon was inadequate, as the tendon would inevitably heal and re-contract, overpowering the compromised anterior compartment. Their recommendation for a radical tenectomy, excising a distinct segment of the tendon, remains the gold standard for preventing and salvaging equinus deformities in midfoot amputations.
Further refinement of the surgical technique was provided by Pinzur et al., who extensively published on the management of the diabetic foot. Pinzur highlighted that successful limb salvage at the midfoot level in diabetic patients requires a multidisciplinary approach, strict preoperative vascular criteria (emphasizing the necessity of TcPO2 > 30 mmHg), and aggressive tendon balancing. Pinzur's work underscored that the tibialis anterior transfer to the talar neck is non-negotiable in a Chopart amputation to restore the active dorsiflexion force necessary for a plantigrade foot.
More recent clinical guidelines, including those from the American Orthopaedic Foot & Ankle Society (AOFAS), emphasize the critical role of the peroneus brevis transfer in addition to the tibialis anterior transfer. While early literature focused primarily on correcting the sagittal plane deformity (equinus), modern consensus recognizes that coronal plane deform
