MCP Joint Synovectomy & Extensor Tendon Centralization in Inflammatory Arthritis: A Masterclass

Key Takeaway
Join us in the OR for a masterclass on metacarpophalangeal (MCP) joint synovectomy and extensor tendon centralization. This immersive guide details patient selection, comprehensive anatomy, meticulous surgical technique, and crucial pearls for managing inflammatory arthritis-induced ulnar deviation. Learn to restore joint mechanics and improve function, ensuring optimal outcomes for your patients.
Comprehensive Introduction and Patho-Epidemiology
Welcome, colleagues and fellows, to the operating theater and to this definitive masterclass on hand reconstruction. Today, we are addressing one of the most common, functionally debilitating, and biomechanically complex manifestations of inflammatory arthropathies: the metacarpophalangeal (MCP) joint deformity. Specifically, we will deconstruct the surgical management of ulnar deviation with extensor tendon subluxation. This procedure, a Metacarpophalangeal Joint Synovectomy combined with Extensor Tendon Centralization, is a joint-preserving operation meticulously designed to restore native joint mechanics, alleviate recalcitrant pain, and improve functional grip in carefully selected patients. It demands absolute surgical precision, an unparalleled understanding of hand anatomy, and an intricate appreciation for the dynamic interplay of vector forces across the hand and wrist.
The epidemiology of inflammatory arthritis, particularly rheumatoid arthritis (RA), dictates that up to 90% of patients will eventually develop hand and wrist involvement over the course of their disease. While the advent of disease-modifying antirheumatic drugs (DMARDs) and biologic therapies has revolutionized the medical management of RA, drastically reducing the incidence of severe, end-stage destructive arthropathy, a significant subset of patients still progresses to soft-tissue failure. In these patients, the synovial hypertrophy outpaces medical control, leading to a mechanical cascade of ligamentous attenuation and tendon subluxation. It is here, in the critical window before irreversible articular cartilage destruction occurs, that our surgical intervention is paramount.
The pathophysiology of this deformity is driven by the proliferative synovitis, or pannus, which acts as a locally destructive tumor. This hypertrophic tissue mechanically distends the joint capsule and enzymatically degrades the stabilizing collateral ligaments and the extensor hood mechanism. As the radial sagittal band attenuates under the pressure of the expanding synovium, the extensor digitorum communis (EDC) tendon slides into the ulnar valleys between the metacarpal heads. Once displaced, the EDC loses its mechanical advantage as a primary extensor and becomes a deforming force, acting as an ulnar deviator and a secondary flexor of the MCP joint. This creates a vicious, self-perpetuating cycle of deformity that medical management alone cannot reverse.
Our goal with this procedure is not merely cosmetic; it is a fundamental biomechanical reset. By meticulously excising the offending synovial tissue and reconstructing the extensor mechanism, we eliminate the primary driver of joint destruction and re-establish the central vector of the extensor tendons. This masterclass will guide you through the exhaustive surgical anatomy, the precise indications for intervention, the step-by-step operative technique, and the rigorous postoperative rehabilitation required to achieve and maintain optimal functional outcomes in these complex patients. Let us scrub in and begin.
Detailed Surgical Anatomy and Biomechanics
Before a single incision is planned, a profound, three-dimensional understanding of the MCP joint's intricate anatomy is absolutely paramount. The MCP joint is a diarthrodial condylar joint, permitting motion in two primary planes: flexion-extension and radial-ulnar deviation, which together allow for circumduction. Normally, the joint arc accommodates approximately 90 degrees of flexion, though the degree of hyperextension can vary significantly depending on individual ligamentous laxity.
Static Stabilizers of the Metacarpophalangeal Joint
The stability of the MCP joint is a complex symphony orchestrated by both static and dynamic elements. The primary static stabilizers are the collateral ligaments, which exhibit a unique biomechanical behavior due to the osseous morphology of the metacarpal head. The metacarpal head possesses a distinct "cam effect"; its diameter increases in both the transverse and sagittal planes from dorsal to volar. Consequently, the collateral ligaments are relatively lax in full extension, permitting maximal radial and ulnar deviation. As the joint flexes, the ligaments are drawn tightly over the expanding condyles, becoming maximally taut at 70 to 90 degrees of flexion, thereby locking the joint and preventing lateral deviation during power grip.
The MCP joint collateral ligaments are inherently asymmetric, a critical factor in understanding the natural tendency toward ulnar drift. The ulnar collateral ligament (UCL) is typically thicker and aligned more parallel to the longitudinal axis of the phalanx, whereas the radial collateral ligament (RCL) is thinner and more oblique. This anatomical asymmetry contributes to a subtle but distinct supination of the proximal phalanx during normal MCP joint flexion. Furthermore, the accessory collateral ligaments connect the true collateral ligaments to the volar plate, ensuring the volar plate remains intimately apposed to the volar aspect of the metacarpal head throughout the entire arc of motion.
The volar plate itself is a robust, fibrocartilaginous structure distally, transitioning to a more membranous, pliant tissue proximally. It acts as the primary checkrein against MCP joint hyperextension. The A-1 pulley of the digital flexor tendon sheath is firmly integrated into the volar plate, linking flexor tendon mechanics directly to joint stability. Connecting the volar plates of adjacent MCP joints is the deep transverse metacarpal ligament, a stout fibrous band that provides critical inter-metacarpal stability and serves as an anatomical landmark, separating the volar lumbrical muscles from the dorsal interossei.
Dynamic Stabilizers and the Extensor Mechanism
The dynamic stabilizers comprise the musculotendinous units that actively govern joint position and counteract external deforming forces. The Extensor Digitorum Communis (EDC) tendon is the central protagonist in our reconstructive procedure. Crucially, the EDC has no direct, robust insertion into the base of the proximal phalanx; instead, it extends the MCP joint via a complex sling mechanism known as the sagittal bands. These transverse fibers originate from the extensor tendon and sweep volarly to insert onto the volar plate and the deep transverse metacarpal ligament.
The sagittal bands function to maintain the EDC tendon centralized over the apex of the metacarpal head during flexion and extension. Anatomically, the ulnar sagittal band is generally thicker, denser, and biomechanically stronger than its radial counterpart. This inherent imbalance is a primary reason why, when the joint is subjected to the symmetric distension of inflammatory synovitis, the weaker radial sagittal band is the first to fail, inevitably leading to ulnar subluxation of the extensor tendon.
Further complicating the dynamic balance are the intrinsic muscles of the hand. The lumbrical muscles originate from the flexor digitorum profundus tendons, pass volar to the deep transverse metacarpal ligament, and insert into the radial lateral bands of the extensor mechanism, acting as primary flexors of the MCP joints and extensors of the interphalangeal joints. The interossei muscles (three volar adductors and four dorsal abductors) pass dorsal to the deep transverse metacarpal ligament. Their variable insertions into the proximal phalanx and extensor hood mean that any alteration in MCP joint alignment dramatically shifts their vector of pull, often exacerbating established deformities.
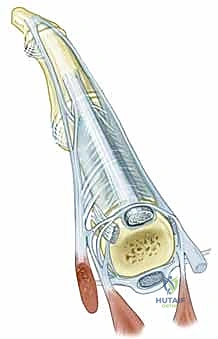
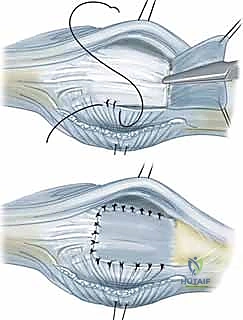
Figure 1: Normal anatomy of the metacarpophalangeal joint. Note the precise central position of the extensor tendon maintained by the symmetric tension of the sagittal bands.
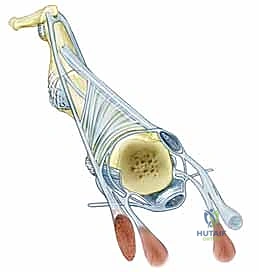
Figure 2: Abnormal anatomy characteristic of inflammatory arthritis, illustrating the profound ulnar subluxation of the extensor tendon secondary to radial sagittal band attenuation.
Pathomechanics of Ulnar Drift and Volar Subluxation
The pathogenesis of the classic rheumatoid hand deformity is a multi-factorial cascade initiated by proliferative synovitis. As the inflammatory pannus expands, it mechanically stretches the joint capsule and the stabilizing ligaments. The radial collateral ligament and the radial sagittal band are particularly vulnerable to this distension. Once the radial sagittal band stretches beyond its elastic limit, the equilibrium of forces shifts irrevocably.
With the loss of radial restraint, the stronger ulnar sagittal band pulls the EDC tendon into the ulnar gutter between the metacarpal heads. Once subluxated, the mechanical axis of the EDC falls volar to the center of rotation of the MCP joint. The tendon ceases to function as an extensor and instead becomes a powerful ulnar deviator and a secondary flexor. This abnormal vector forces the proximal phalanx into ulnar deviation and volar subluxation.
Simultaneously, the distension of the volar capsule and the membranous portion of the volar plate creates ligamentous laxity on the volar aspect of the joint. This laxity grants the powerful flexor tendons a mechanical advantage, exponentially increasing their flexion force across the joint and further driving the volar subluxation of the proximal phalanx. The normal ulnar and volar slope of the metacarpal condyles provides an osseous "slide" that facilitates this progressive displacement. As the deformity worsens, the intrinsic muscles, particularly the ulnar interossei, undergo myostatic contracture, converting a passively correctable dynamic deformity into a rigid, fixed contracture.
Neurovascular Considerations in the Dorsal Approach
While the major neurovascular bundles of the digits are located volarly and are generally safe during a dorsal approach to the MCP joints, the surgeon must remain acutely aware of the dorsal sensory anatomy. The dorsal digital nerves, terminal branches of the superficial radial nerve and the dorsal sensory branch of the ulnar nerve, course through the dorsal subcutaneous tissues. These nerves are highly susceptible to iatrogenic injury during the initial transverse skin incision and subsequent flap elevation.
Injury to these dorsal sensory nerves can result in debilitating neuromas, which can severely compromise the functional outcome of an otherwise technically perfect joint reconstruction. Meticulous blunt dissection and careful retraction are essential. Furthermore, the dorsal venous network is extensive and fragile in patients with chronic inflammatory disease, particularly those on long-term corticosteroid therapy. Preserving the major longitudinal venous channels is critical to preventing postoperative venous congestion, massive edema, and subsequent wound healing complications, which can delay the initiation of crucial early rehabilitation.
Exhaustive Indications and Contraindications
The success of an MCP joint synovectomy and extensor tendon centralization hinges entirely on rigorous patient selection. This is not a salvage procedure for a destroyed joint; it is a prophylactic and reconstructive intervention designed for a joint that is mechanically compromised but biologically viable. The ideal candidate presents with progressive ulnar deviation and extensor tendon subluxation that is refractory to optimal medical management, yet retains well-preserved articular cartilage.
Patient Selection Criteria
The primary indication for this procedure is a patient with inflammatory arthritis who exhibits a passively correctable ulnar deviation deformity at the MCP joints, accompanied by extensor tendon subluxation. Crucially, the patient must have intact, functioning flexor and extensor musculotendinous units. If the extensor tendons have ruptured (a common complication in RA at the level of the distal radioulnar joint), tendon transfers or grafts must be incorporated into the surgical plan.
Radiographic evaluation is the ultimate arbiter of surgical candidacy. High-quality, multi-planar radiographs must demonstrate Larsen Grade 1 or 2 changes—specifically, periarticular osteopenia and marginal erosions, but with preservation of the joint space and an absence of significant architectural destruction or fixed volar subluxation. If the joint space is obliterated or if there is severe, uncorrectable volar subluxation with bone-on-bone articulation, soft tissue realignment will inevitably fail. In such advanced cases (Larsen Grades 3-5), the surgeon must pivot to joint arthroplasty (e.g., silicone interpositional arthroplasty) or arthrodesis.
Differential Diagnosis: Rheumatoid Arthritis Versus Systemic Lupus Erythematosus
While RA is the most common etiology, understanding the nuances of other inflammatory arthropathies, such as Systemic Lupus Erythematosus (SLE), is critical for operative planning. In SLE, the profound hand deformities (Jaccoud's arthropathy) are primarily driven by systemic collagen abnormalities and severe ligamentous/tendinous imbalances, rather than the aggressive, erosive synovitis seen in RA.
Consequently, SLE patients often present with dramatic, sweeping ulnar deviation and severe subluxation, yet their articular cartilage remains remarkably pristine even after decades of disease. Because the cartilage is preserved, soft tissue realignment procedures remain highly viable and effective in SLE patients, even in long-standing cases that would typically require arthroplasty in an RA patient. However, the surgeon must be warned: SLE patients are highly prone to "shifting" deformities. Over-correction or aggressive intrinsic release in an SLE patient can easily convert an ulnar drift into a rigid, iatrogenic radial deviation deformity postoperatively.

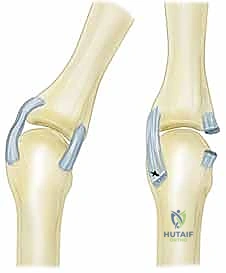
Figure 3: Preoperative radiograph demonstrating classic extensor tendon subluxation and ulnar deviation of the MCP joints, notably with well-maintained joint spaces, making this an ideal candidate for soft tissue reconstruction.

Figure 4: Radiograph depicting extensor tendon subluxation and ulnar deviation with reducible MCP joint subluxation of the index and middle fingers. The lack of severe erosive changes is the key indicator for synovectomy and centralization over arthroplasty.
Indications and Contraindications Table
| Parameter | Absolute Indications | Relative Indications | Absolute Contraindications |
|---|---|---|---|
| Clinical Presentation | Passively correctable ulnar drift; Extensor tendon subluxation | Mild, early fixed contracture amenable to intrinsic release | Rigid, fixed, non-correctable deformity; Active joint infection |
| Radiographic Findings | Larsen Grade 1-2; Preserved joint space; Minimal marginal erosions | Moderate erosions without loss of central articular cartilage | Larsen Grade 3-5; Obliterated joint space; Severe bone loss; Fixed volar subluxation |
| Tendon Status | Intact flexor and extensor tendons | Extensor tendon rupture (requires concurrent tendon transfer) | Irreparable tendon loss precluding active motion post-reconstruction |
| Systemic Status | Medically optimized; Controlled systemic inflammation | SLE with Jaccoud's arthropathy (requires cautious balancing) | Uncontrolled, fulminant systemic disease; Poor soft tissue envelope |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough preoperative planning is the bedrock of a successful surgical outcome. The evaluation must extend far beyond the isolated MCP joints to encompass the entire upper extremity biomechanical chain. A localized approach to the hand without considering the wrist or the proximal interphalangeal (PIP) joints will inevitably lead to recurrent deformity and surgical failure.
Clinical and Radiographic Evaluation
The surgeon must meticulously evaluate the alignment of the wrist. In rheumatoid arthritis, the carpus frequently collapses into radial deviation and supination. This radial deviation of the wrist creates a compensatory, zigzag mechanical moment that forcefully drives the metacarpals into ulnar deviation. If a severe, fixed radial deviation deformity of the wrist is present, performing an isolated MCP joint centralization is futile; the uncorrected wrist vectors will quickly tear through the MCP soft tissue reconstruction. In such cases, wrist realignment (via limited arthrodesis or total wrist arthroplasty) must be staged prior to, or concurrently with, the MCP joint surgery.
Equally critical is the assessment of the PIP joints. The presence of a severe boutonnière deformity (PIP flexion, DIP extension) will severely compromise the postoperative rehabilitation of the MCP joints. If the PIP joint is locked in flexion, the patient will be unable to actively flex the MCP joint postoperatively, leading to stiffness and loss of the centralization. Therefore, significant boutonnière deformities must be surgically corrected prior to addressing the MCP joints. Conversely, a swan-neck deformity (PIP hyperextension, DIP flexion) can sometimes be managed concurrently, and a slightly stiff PIP joint in extension can actually facilitate better active MCP joint flexion during the early postoperative phase.

Figure 5: Clinical presentation of the rheumatoid hand, highlighting the necessity of evaluating the entire kinetic chain, including wrist alignment and PIP joint status, prior to surgical intervention.
Anesthesia, Positioning, and Tourniquet Management
The procedure is typically performed under regional anesthesia (supraclavicular or axillary brachial plexus block), which provides excellent intraoperative operating conditions and superior, prolonged postoperative analgesia. General anesthesia is reserved for patients with contraindications to regional blocks or those who cannot tolerate lying still for the duration of the procedure.
The patient is positioned supine on the operating table. The affected upper extremity is extended onto a dedicated, radiolucent hand table. This provides a stable, expansive, and sterile working surface. The arm is comfortably abducted to approximately 45 degrees and externally rotated.
A well-padded pneumatic tourniquet is applied to the proximal brachium. Following meticulous exsanguination of the limb using an Esmarch bandage, the tourniquet is inflated to 250-280 mmHg. A bloodless surgical field is not a luxury; it is an absolute necessity for this procedure. The safe identification and preservation of the delicate dorsal sensory nerves, the fragile venous network, and the attenuated sagittal bands require pristine visualization that is impossible in a bloody field. Standard sterile preparation of the entire hand and forearm is performed, followed by precise draping to isolate the surgical field while allowing full manipulation of the wrist and digits.
Step-by-Step Surgical Approach and Fixation Technique
We are now ready to proceed with the operative intervention. The tourniquet is inflated, the field is bloodless, and our preoperative plan is clearly defined. The surgical sequence must be executed with atraumatic tissue handling and precise anatomical restoration.
Incision, Exposure, and Flap Elevation
When addressing multiple digits simultaneously—the standard scenario in inflammatory arthritis—a transverse dorsal incision is the gold standard. This approach provides panoramic exposure of all involved MCP joints, allows for simultaneous comparison of tendon tension, and minimizes tension on the skin edges during closure, which is critical given the often fragile, steroid-thinned skin of these patients.
Using a #15 scalpel, a transverse incision is made across the dorsal aspect of the MCP joints, typically extending from the radial aspect of the second metacarpal head to the ulnar aspect of the fifth metacarpal head. The incision should be placed slightly proximal to the metacarpal heads to ensure the skin closure does not overlie the reconstructed extensor mechanisms during flexion.
Surgical Pearl: When correcting ulnar deviation across multiple digits, always begin your reconstruction with the radial-most involved digit (typically the index finger) and work ulnarly. Correcting the index finger establishes the foundation and the correct line of pull for the subsequent digits, preventing a cascading failure of the reconstruction.
Flap elevation must be performed with extreme care. Using a combination of sharp dissection with Metzenbaum scissors and blunt spreading, the dorsal skin flaps are elevated in the plane immediately superficial to the extensor paratenon. The surgeon must actively identify and preserve the longitudinal dorsal veins and the fine branches of the dorsal sensory nerves. Retraction of the skin flaps should be achieved with blunt, atraumatic retractors (e.g., Ragnell or Senn retractors) to avoid ischemic necrosis of the wound edges.

Figure 6: The initial transverse dorsal incision and careful elevation of the skin flaps, demonstrating the critical preservation of the dorsal venous network and sensory nerve branches.
Synovectomy and Joint Debridement
Once the extensor mechanism of each joint is exposed, the degree of ulnar subluxation of the EDC tendon is assessed. To access the joint space, a longitudinal incision is made through the attenuated radial sagittal band, parallel to the radial border of the extensor tendon. The EDC tendon is then sharply retracted ulnarly, exposing the underlying dorsal joint capsule.
The dorsal capsule is incised longitudinally, revealing the synovial cavity. In the rheumatoid patient, the joint will be engorged with hyperplastic, friable, and highly vascular pannus. A meticulous synovectomy is performed using a combination of sharp excision with a #15 blade, fine rongeurs, and a motorized synovial shaver if necessary.
The surgeon must systematically clear the pannus from the dorsal pouch, the collateral ligament recesses, and, crucially, the volar pouch beneath the metacarpal head. To access the volar pouch, the proximal phalanx is gently volar-flexed, and a small, curved rongeur is passed volarly to extract the hidden synovial tissue. Extreme care must be taken to avoid scoring or damaging the preserved articular cartilage during this process. The collateral ligaments should be inspected; while often stretched, they are rarely completely ruptured and should be preserved.
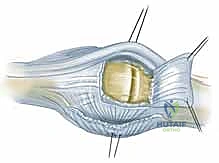
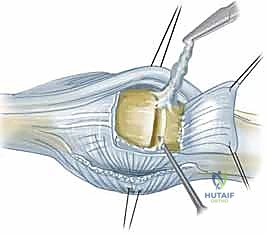
Figure 7: Exposure of the joint space following incision of the radial sagittal band. The hyperplastic synovium (pannus) is visualized prior to meticulous excision.
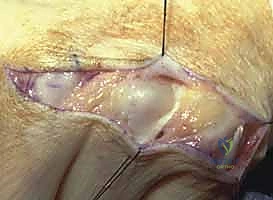
Figure 8: Intraoperative view highlighting the severe ulnar subluxation of the extensor tendons into the intermetacarpal valleys, a hallmark of advanced inflammatory soft-tissue failure.
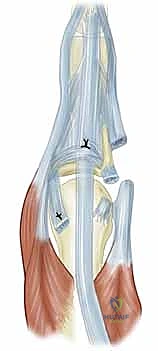
Intrinsic Release and Soft Tissue Balancing
Following the synovectomy, the joint must be assessed for passive correctability. The proximal phalanx is manually manipulated into neutral alignment (zero degrees of radial/ulnar deviation) and full extension. If resistance is encountered, or if the digit springs back into ulnar deviation upon release, an intrinsic muscle contracture is present and must be addressed.
The ulnar intrinsic tightness is evaluated using the intrinsic tightness test (Bunnell test). If the ulnar intrinsic muscles (the volar interossei and the abductor digiti minimi for the small finger) are contracted, an intrinsic release is mandatory. This is performed by identifying the oblique fibers of the ulnar intrinsic wing at the level of the proximal phalanx and sharply dividing them. In severe cases, a release of the ulnar collateral ligament from its metacarpal origin may be necessary to achieve full passive correction, though this should be done judiciously to avoid creating iatrogenic radial instability.

Figure 9: Execution of an ulnar intrinsic release. The oblique fibers of the ulnar intrinsic wing are identified and divided to alleviate the fixed deforming forces.
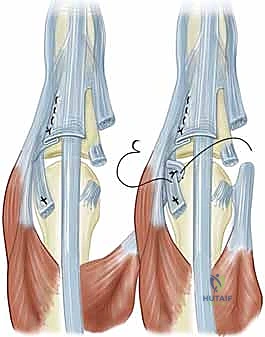
Extensor Tendon Centralization and Sagittal Band Reconstruction
This is the most critical biomechanical step of the procedure. The EDC tendon must be relocated from the ulnar gutter and secured over the exact dorsal apex of the metacarpal head. To achieve this, the ulnar sagittal band—which is tethering the tendon ulnarly—must be completely divided.
Once the ulnar release is complete, the EDC tendon is manually centralized. The attenuated radial sagittal band is then reefed (imbricated) and sutured over the centralized tendon to hold it in place. We utilize non-absorbable, braided sutures (e.g., 4-0 Ethibond or Ticron) in a horizontal mattress
Clinical & Radiographic Imaging Archive