Malunions of the Tibial and Fibular Shafts
The surgical correction of tibial and fibular shaft malunions represents a formidable challenge in reconstructive orthopaedics. While the precise degree of deformity that mandates surgical intervention remains a subject of ongoing debate, it is an established biomechanical principle that angular and rotational deformities of the tibial diaphysis profoundly alter the contact pressures within the knee and ankle joints. Over time, these aberrant load-bearing mechanics predispose the patient to the development of premature secondary osteoarthritis, gait dysfunction, and severe chronic pain.
Pathomechanics and the Development of Osteoarthritis
The relationship between diaphyseal malalignment and adjacent joint arthrosis is complex. Historically, it has been widely believed that angular deformities of the tibial shaft directly cause deleterious alterations in joint contact pressures. However, clinical series with long-term follow-up have yielded nuanced, and sometimes conflicting, results regarding this hypothesis.
Some studies have indicated that the ankle joint is more susceptible to arthritic degeneration than the knee following a tibial malunion, noting that the location of the fracture plays a significant role. In these series, poorer functional ankle scores correlated directly with the severity of the malalignment and the proximity of the deformity to the ankle joint. Furthermore, varus deformities were generally found to be more poorly tolerated than valgus deformities due to the medialization of the mechanical axis and subsequent medial ankle overload.
Conversely, subsequent investigations have found the exact opposite: that symptomatic presentation at the knee correlated strongly with radiographic arthritic changes, whereas symptoms at the ankle did not. These studies failed to demonstrate a definitive relationship between the location of the fracture and the subsequent development of osteoarthritis in either the knee or the ankle. Furthermore, isolated rotational deformities were not independently associated with arthritic changes.
A landmark study by Milner et al. provided critical clarity, determining that fracture malunion did not inherently cause a higher incidence of ankle and subtalar arthritis ipsilateral to the fracture. However, their data revealed a distinct trend toward a higher prevalence of medial compartment osteoarthritis of the knee in patients presenting with varus malalignment of the lower limb. Additionally, limb shortening of 10 mm or more was strongly correlated with subjective complaints of knee pain. While osteoarthritis occurred more frequently on the side of the fracture, the consensus suggests that factors beyond simple mechanical malalignment—such as initial articular cartilage damage at the time of injury, altered neuromuscular control, and changes in gait kinematics—contribute significantly to the development of post-traumatic osteoarthritis.
Clinical Evaluation and Indications for Surgical Intervention
The threshold for "acceptable" deformity varies considerably among authors and institutions. However, strict biomechanical parameters have been established to guide surgical decision-making.
Surgical correction is generally recommended for deformities exceeding the following parameters:
* Valgus deformity: Greater than 12 degrees.
* Varus deformity: Greater than 6 degrees.
* External rotation deformity: Greater than 15 degrees.
* Internal rotation deformity: Greater than 10 degrees.
* Leg-Length Discrepancy (LLD): Shortening of 2 cm or less is usually well tolerated with conservative measures such as shoe lifts and orthotic modifications. However, shortening exceeding 2.5 cm typically causes significant functional disability, pelvic obliquity, and secondary lumbar spine pathology, warranting surgical lengthening.
When evaluating a patient for the correction of a tibial malunion, the surgeon must synthesize multiple variables: the absolute degree of the deformity, the patient’s subjective symptoms, the biological condition of the injured extremity, and the functional demands of the patient.
Disability from tibial shaft malunion is primarily driven by rotational deformity, lateral and posterior bowing, and shortening. Frequently, a compensatory contracture of the Achilles tendon develops, resulting in a rigid equinus deformity of the foot. Clinical symptoms may manifest as ankle, knee, or back pain; severe gait disturbances; and a cosmetically unacceptable appearance.
Clinical Pearl: A thorough evaluation of the soft tissue envelope is paramount. The limb must be meticulously assessed for a history of neurological or vascular injury, the adequacy of soft tissue coverage, and the presence of subclinical or active infection.
If a history of vascular injury exists, preoperative arteriograms or CT angiography are essential to delineate the vascular tree and safely plan the operative approach. If the soft tissues overlying the planned osteotomy site are compromised, a simultaneous local rotation flap or a vascularized free tissue transfer may be required to provide a robust biological environment for bone healing and to prevent catastrophic wound dehiscence.
In patients with a history of open fractures or previous surgical site infections, ruling out active osteomyelitis is critical. Preoperative indium-labeled white blood cell scans, gallium scans, or technetium bone scans can be utilized to determine the metabolic activity of any suspected infection.
Surgical Warning: It is an absolute requirement to definitively treat and eradicate any active infection prior to performing a corrective osteotomy for malunion. Furthermore, any associated equinus contractures should be addressed simultaneously, typically via a percutaneous or open lengthening of the Achilles tendon.
Preoperative Planning and Deformity Analysis
Meticulous preoperative planning is the cornerstone of successful malunion correction. The surgeon must precisely quantify the amount of angular deformity, rotational malalignment, leg-length discrepancy, and translational displacement.
Angular deformities in the frontal (varus-valgus) and sagittal (flexion-extension) planes rarely exist in isolation; they typically combine to form a uniplanar deformity in an oblique plane. The true magnitude of this maximal deformity is always greater than the angular measurements seen on standard orthogonal anteroposterior (AP) or lateral radiographs.
To identify the plane of maximal deformity intraoperatively or during fluoroscopic planning, the leg is rotated under live fluoroscopy until the maximal degree of bowing is visualized. A radiograph taken at exactly 90 degrees to this plane will demonstrate a perfectly straight bone with zero angular deformity. The corrective oblique osteotomy must be executed perpendicular to this identified plane of maximal deformity.
Rotational deformities are best evaluated using computed tomography (CT) scanograms, measuring the tibial torsion angle by comparing the proximal posterior tibial condylar axis to the distal bimalleolar axis. Clinically, this can be estimated by measuring the transmalleolar axis relative to the patella.
Preoperative templating must include detailed drawings of both the injured and contralateral uninjured extremities, pinpointing the Center of Rotation of Angulation (CORA), the exact site and configuration of the planned osteotomy, and the specific internal or external fixation devices to be utilized.
Neurological Monitoring: To prevent iatrogenic neurological complications—particularly peroneal nerve palsy—somatosensory evoked potentials (SSEPs) and motor evoked potentials (MEPs) should be utilized during the correction of severe deformities, especially when acute lengthening or significant valgus correction is performed.
Surgical Approaches and Osteotomy Techniques
The choice of osteotomy depends on the geometry of the deformity, the presence of shortening, and the quality of the local bone and soft tissue.
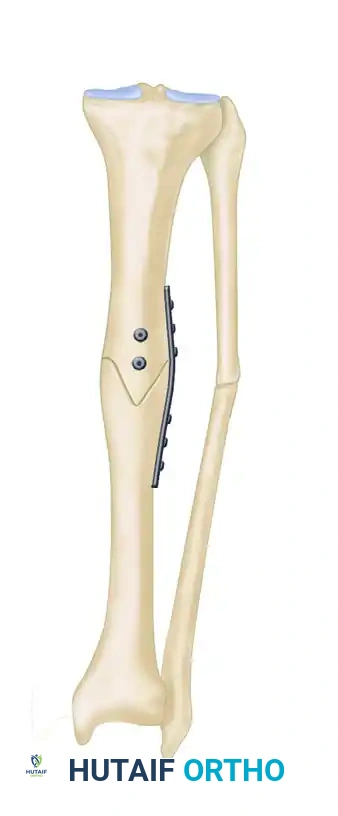
- Simple Wedge Osteotomies: Opening wedge, closing wedge, or dome-shaped osteotomies are highly effective for correcting relatively small degrees of uniplanar malunion. However, closing wedge osteotomies inherently create additional limb shortening, while opening wedge osteotomies almost always require structural autograft or allograft to fill the resulting void and provide stability.
- Oblique Osteotomies: Ideal for multiplanar deformities. These cuts provide a broad, bleeding cancellous surface area for rapid bone healing. Furthermore, limb lengthening can be achieved simultaneously by allowing the distal fragment to slide distally along the oblique osteotomy plane before fixation.
- Clamshell Osteotomy: Described by Russell et al., this technique is particularly useful for complex nonunions or malunions of the tibial diaphysis characterized by a long, malaligned, and sclerotic segment. It involves a longitudinal osteotomy combined with transverse cuts, allowing the surgeon to "open" the diaphysis, re-establish the medullary canal, and correct the alignment around an intramedullary nail.
- Supramalleolar Osteotomy: While osteotomies are traditionally performed at the apex of the deformity (the old fracture site), a supramalleolar approach may be preferable if the original fracture site exhibits poor healing potential, is covered by a compromised soft tissue envelope, or consists of extremely dense, avascular sclerotic bone.
- Ilizarov Technique: For infected tibial malunions, or those associated with a severely compromised soft tissue envelope, acute correction and internal fixation are contraindicated. These complex cases are best managed via the Ilizarov method, utilizing a minimally invasive corticotomy and gradual, computer-assisted spatial frame correction with a ring and wire fixator.
Step-by-Step Surgical Technique: Oblique Osteotomy for Multiplanar Deformity
Oblique tibial osteotomies stabilized with dynamic compression plates and lag screws have been strongly advocated for the treatment of multiplanar tibial deformities, yielding excellent long-term results. Sanders et al. highly recommended this technique for tibial shaft deformities requiring less than 2.5 cm of simultaneous lengthening.
Indications: Multiplanar diaphyseal malunion requiring angular, rotational, and length correction (<2.5 cm).
Contraindications: Inadequate soft tissue coverage, active osteomyelitis, or severe vascular insufficiency.


- Positioning and Exposure: The patient is positioned supine on a radiolucent table. A standard longitudinal incision is made over the anterior or anteromedial aspect of the tibia, taking care to preserve the periosteal blood supply.
- Identifying the Plane: Under fluoroscopic guidance, the plane of maximal deformity is identified.
- The Osteotomy: An oblique osteotomy is marked perpendicular to the plane of maximal deformity. Multiple drill holes are made along the planned osteotomy line to prevent thermal necrosis and control the propagation of the cut. The osteotomy is completed using a sharp osteotome or an oscillating saw under continuous saline irrigation.
- Correction and Lengthening: The distal fragment is mobilized. Rotational and angular deformities are corrected manually. If lengthening is required, the distal fragment is translated distally along the oblique plane of the osteotomy.
- Temporary Fixation: The corrected position is provisionally held with reduction clamps and Kirschner wires. Fluoroscopy confirms the restoration of the mechanical axis in both the AP and lateral planes.
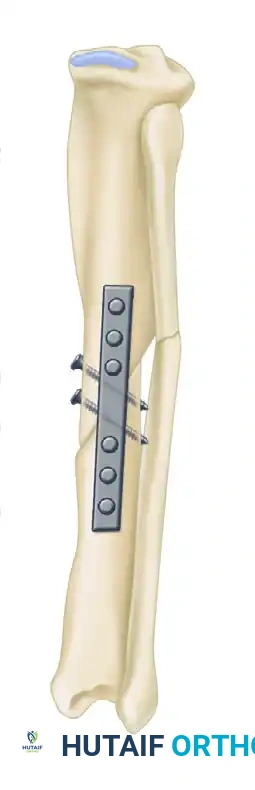
- Definitive Fixation: A heavy-duty dynamic compression plate (or locking compression plate depending on bone quality) is contoured to the corrected anatomy. Interfragmentary lag screws are placed orthogonally across the oblique osteotomy to provide absolute stability and primary bone healing. The plate is then secured with bicortical screws.


Fixation Strategies: Intramedullary Nails and External Fixators
Maintaining satisfactory alignment after an osteotomy is impossible without robust internal or external fixation.
Intramedullary Nailing:
Reamed, locked intramedullary (IM) nailing is a highly effective method for stabilizing osteotomies in the tibial diaphysis. If an IM nail is selected, the sclerotic medullary canal must be meticulously opened at both ends of the old fracture site. Any cortical gaps created by the osteotomy should be packed with autologous cancellous bone graft to stimulate osteogenesis.
Surgical Technique Tip: We prefer to use statically locked nails initially to maximize the rotational and axial stability of the osteotomy. The limited incisions used for the osteotomy are closed after opening the medullary canals and passing the ball-tipped guidewire, but before the initiation of reaming and nail insertion. This prevents the extrusion of reaming debris into the soft tissues. Static locking can be converted to dynamic locking several weeks postoperatively if dynamization is required to promote callus formation.
It is critical to note that if a massive amount of soft tissue stripping is required to expose and correct the deformity, fixation methods other than IM nailing may be preferable. Intramedullary reaming disrupts the endosteal blood supply; combining this with extensive periosteal stripping can completely devascularize the bone segment, leading to atrophic nonunion.
External Fixation:
A history of previous external fixation, particularly if complicated by pin track infections, is a relative contraindication to immediate intramedullary nailing due to the unacceptably high risk of deep medullary infection. In such scenarios, or when dealing with an active infection or a hostile soft tissue envelope, modern circular external fixation remains the gold standard.


Preoperative AP and Lateral radiographs demonstrating a severe varus malunion of the distal tibia.

Intraoperative radiograph showing the osteotomy of the tibia and fibula, with the anatomical reduction maintained rigidly by a circular external fixator.


Postoperative AP and Lateral radiographs demonstrating solid tibial union with restoration of normal mechanical alignment. An asymptomatic nonunion of the fibular osteotomy persists, which is a common and clinically benign finding.
Management of Distal Tibial and Ankle Malunions
Malunions involving the distal metaphyseal-epiphyseal junction or the ankle mortise require special consideration. Surgery is strictly indicated in the following scenarios:
- Malunited bimalleolar fractures: With or without significant angular deformity, in which radiographs demonstrate definite post-traumatic arthritic changes that are the primary cause of persistent pain and disability.
- Malunited trimalleolar fractures: Specifically those of long duration presenting with posterior and proximal subluxation or dislocation of the talus.
- Unreconstructable Deformities: Malunited fractures in which the deformity is so severe that it cannot be completely corrected by joint-sparing conservative reconstruction, or in which the required surgical exposure would be so extensive that avascular necrosis or rapid arthritic degeneration of the ankle is inevitable.
In cases where joint salvage is impossible, ankle arthrodesis is the treatment of choice.
Surgical Warning: When marked diaphyseal or metaphyseal malalignment is present, it must always be corrected by a concurrent osteotomy at the time of the ankle arthrodesis. Fusing the ankle in a malaligned limb will inevitably lead to severe, disabling foot strain and rapid degeneration of the subtalar and transverse tarsal joints. This additional corrective procedure does not materially complicate the operation or delay overall recovery, but it is vital for long-term functional success.
Postoperative Protocol and Complication Management
Postoperative rehabilitation is dictated by the stability of the fixation and the quality of the host bone. For rigidly plated oblique osteotomies or statically locked IM nails, patients are typically kept non-weight-bearing or touch-down weight-bearing for the first 6 weeks, followed by progressive weight-bearing as radiographic evidence of bridging callus appears.
Surgeons must remain vigilant for potential complications, which include:
* Inability to restore full length: Often due to chronic soft tissue contracture or neurovascular tethering.
* Delayed union or nonunion: Managed with dynamization (for nails), bone grafting, or revision fixation.
* Hardware failure: Plate breakage or screw pullout, typically resulting from premature weight-bearing or inadequate mechanical stability.
* Infection: Ranging from superficial wound dehiscence to deep osteomyelitis, requiring aggressive debridement and targeted antibiotic therapy.
* Vascular injury or Compartment Syndrome: Requiring immediate surgical exploration and fasciotomy.
Through meticulous preoperative planning, respect for the soft tissue envelope, and precise execution of biomechanically sound osteotomies, orthopaedic surgeons can successfully reconstruct tibial and fibular shaft malunions, restoring limb alignment, eradicating pain, and preserving long-term joint function.
