Operative Management of Deep Hand Space Infections and Septic Arthritis
Key Takeaway
Infections of the radial and ulnar bursae, alongside septic arthritis of the finger joints, represent acute orthopedic emergencies. Prompt recognition and aggressive surgical intervention are paramount to prevent irreversible cartilage destruction, osteomyelitis, and profound functional loss. This guide details the anatomical principles, diagnostic criteria, and step-by-step operative techniques for incision, drainage, and continuous irrigation of deep hand space infections and septic articulations.
INTRODUCTION TO DEEP SPACE INFECTIONS OF THE HAND
Acute pyogenic infections of the hand, particularly those involving the deep tenosynovial sheaths and articular cavities, are limb-threatening emergencies that demand immediate surgical intervention. The complex, compartmentalized anatomy of the hand facilitates the rapid, predictable spread of purulence along synovial planes. Delayed treatment of infections within the radial and ulnar bursae, or within the interphalangeal and metacarpophalangeal joints, invariably leads to catastrophic outcomes, including tendon necrosis, irreversible articular cartilage destruction, osteomyelitis, and profound functional impairment.
This comprehensive guide delineates the precise anatomical considerations, diagnostic criteria, and step-by-step operative techniques required for the successful incision, drainage, and postoperative management of radial and ulnar bursae infections, as well as septic arthritis of the finger joints.
INFECTIONS OF THE RADIAL AND ULNAR BURSAE
Anatomical and Biomechanical Considerations
The radial and ulnar bursae are the proximal tenosynovial sheaths of the flexor tendons at the level of the wrist and palm. Understanding their anatomical boundaries is critical for effective surgical drainage.
- The Radial Bursa: This structure is the proximal prolongation of the flexor pollicis longus (FPL) tendon sheath. It extends from the distal phalanx of the thumb, passes through the carpal tunnel, and terminates proximally at the level of the pronator quadratus in the distal forearm.
- The Ulnar Bursa: This bursa is formed by the proximal extension of the tenosynovial sheath of the flexor digitorum superficialis (FDS) and flexor digitorum profundus (FDP) tendons of the little finger. Like the radial bursa, it traverses the carpal tunnel and extends into the distal forearm.
- The "Horseshoe Abscess": In approximately 50% to 80% of patients, the radial and ulnar bursae communicate with each other at the level of the proximal palmar crease or within Parona’s space (the potential space deep to the flexor tendons and superficial to the pronator quadratus). This anatomical communication allows a localized pyogenic flexor tenosynovitis of the thumb or little finger to spread rapidly to the contralateral bursa, creating a classic "horseshoe abscess."
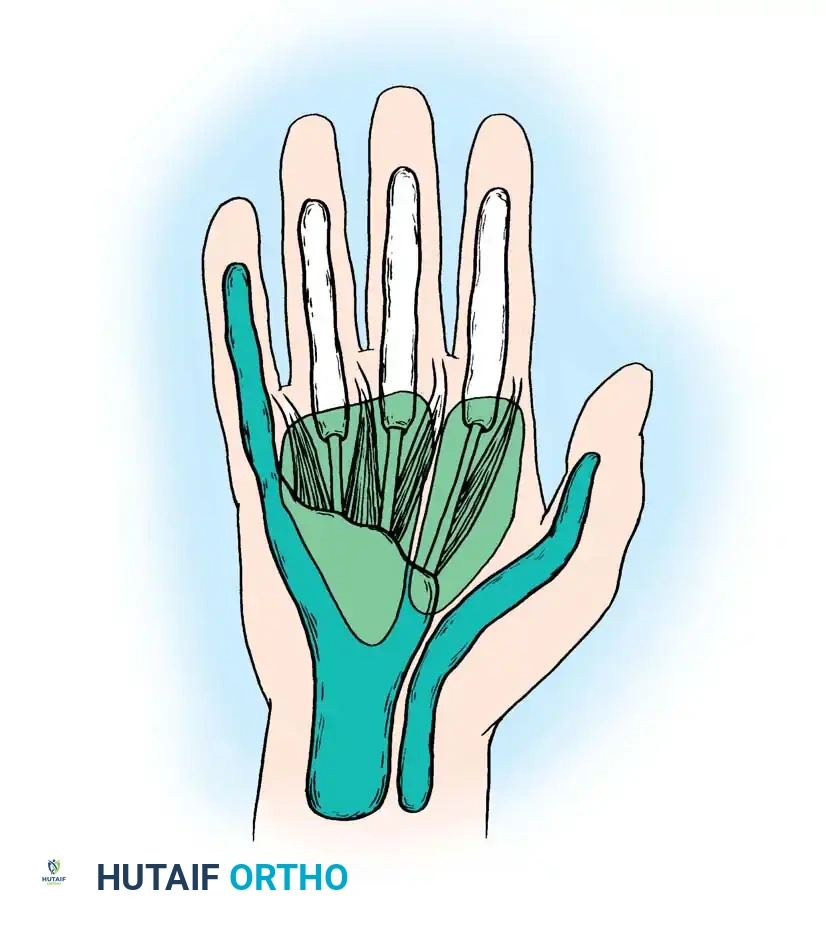
Fig. 75-13 Flexor tendon sheaths and proximal extensions into radial and ulnar bursae, illustrating the potential pathways for a horseshoe abscess. Note the relationship to the midpalmar and thenar spaces.
Clinical Presentation and Diagnosis
Patients presenting with infections of the radial or ulnar bursa typically exhibit severe, throbbing pain, massive swelling of the involved digit, and exquisite tenderness along the course of the flexor sheath. Kanavel's four cardinal signs of flexor tenosynovitis are usually present:
1. Fusiform swelling of the digit.
2. Flexed resting posture of the digit.
3. Exquisite tenderness along the entire course of the flexor tendon sheath.
4. Severe pain on passive extension of the digit (the most sensitive early sign).
If a horseshoe abscess has developed, swelling and tenderness will be evident in both the thumb and the little finger, accompanied by profound swelling in the proximal palm and volar wrist (Parona's space).
Surgical Warning: Do not mistake the dorsal swelling of the hand for the primary site of infection. The rich lymphatic drainage network of the hand courses dorsally, causing massive dorsal edema even when the primary abscess is located entirely within the volar bursae. Incising the dorsal hand in these cases is a critical error.
Operative Technique: Incision and Drainage of Radial and Ulnar Bursae
The goal of surgery is to completely decompress the involved synovial sheaths, evacuate all purulence, obtain cultures, and establish a system for continuous postoperative irrigation.
Preoperative Preparation:
* Anesthesia: General anesthesia or a regional brachial plexus block is required. Local anesthesia is strictly contraindicated due to the risk of spreading the infection and the inability to achieve adequate pain control in an acidic, infected environment.
* Tourniquet: Apply a pneumatic tourniquet to the proximal arm.
* Exsanguination: Crucial Step: Elevate the arm for 3 to 5 minutes to allow gravity exsanguination. Do not use an Esmarch bandage or elastic wrap to exsanguinate the limb. Mechanical compression can force purulence proximally into unaffected fascial planes or systemically into the bloodstream, causing bacteremia.
Step-by-Step Surgical Approach:
- Distal Radial Bursa Incision: To drain the radial bursa, make a midaxial or volar-lateral incision along the proximal phalanx of the thumb. Carefully dissect through the subcutaneous tissue to expose the flexor tendon sheath. Open the bursa at its most distal end (distal to the A1 pulley).
- Proximal Propagation: Introduce a blunt surgical probe or a pediatric feeding tube into the distal opening of the sheath. Gently advance it proximally along the course of the FPL tendon toward the wrist.
- Proximal Radial Bursa Incision: Palpate the end of the probe in the proximal palm or distal volar forearm. Make a second longitudinal incision directly over the end of the probe, taking care to protect the palmar cutaneous branch of the median nerve. Open the proximal extent of the radial bursa.
- Distal Ulnar Bursa Incision: If the ulnar bursa is involved, make a midaxial incision on the ulnar side of the little finger. Expose and open the distal flexor sheath.
- Proximal Ulnar Bursa Incision: Similar to the radial bursa, pass a blunt probe proximally to the wrist. Make a longitudinal incision over the volar-ulnar aspect of the distal forearm/proximal palm to open the proximal ulnar bursa. Protect the ulnar neurovascular bundle.
- Clinical Pearl: If both bursae are involved (a true horseshoe abscess), a single proximal ulnar incision in the distal forearm may occasionally be sufficient to drain the proximal extent of both bursae, as they communicate widely in Parona's space in most patients. However, direct visualization and thorough irrigation of both pathways are mandatory.
- Catheter Placement for Irrigation: Insert small 16-gauge or 18-gauge polyethylene drainage tubes (or pediatric feeding tubes) into the proximal incisions, directing them distally into the sheaths. Insert small rubber drains (e.g., Penrose drains) or leave the distal incisions open to allow for fluid egress.
- Closure: The incisions are left open. Do not attempt primary closure of an infected tenosynovial sheath.
- Dressing: Apply a bulky, non-compressive sterile dressing and a volar splint holding the wrist in slight extension, the metacarpophalangeal (MCP) joints in 70 degrees of flexion, and the interphalangeal (IP) joints in full extension (the intrinsic-plus or "safe" position).
FINGER JOINT INFECTIONS (SEPTIC ARTHRITIS)
Etiology and Pathogenesis
Septic arthritis of the interphalangeal or metacarpophalangeal joints is a highly destructive process. The etiology typically falls into three categories:
1. Direct Penetration: Human bites (clenched-fist injuries or "fight bites"), animal bites, or puncture wounds directly inoculating the joint space.
2. Contiguous Spread: Extension of an adjacent infection, such as a severe flexor tenosynovitis, deep space abscess, or osteomyelitis of the adjacent phalanx.
3. Hematogenous Spread: Less common in the hand than in large joints, but can occur in immunocompromised patients, intravenous drug users, or patients with systemic bacteremia. When hematogenous spread is suspected, a rigorous systemic workup to identify the primary source (e.g., endocarditis, pneumonia) is mandatory.
Once bacteria enter the joint space, the synovial membrane mounts a profound inflammatory response. The influx of polymorphonuclear leukocytes (PMNs) leads to the release of proteolytic enzymes, matrix metalloproteinases (MMPs), and cytokines. This toxic, purulent exudate rapidly degrades articular cartilage glycosaminoglycans and collagen. If left untreated, irreversible cartilage destruction can occur within 24 to 48 hours, followed by extension into the subchondral bone, resulting in osteomyelitis.
Diagnostic Evaluation
The involved joint presents as swollen, erythematous, warm, and exquisitely tender. The finger is typically held in slight flexion to maximize joint volume and minimize capsular tension. Active and passive range of motion is severely restricted by pain. Careful palpation will reveal a fluctuant joint effusion.
Synovial Fluid Analysis:
Definitive diagnosis is achieved via joint aspiration. The aspirate must be sent immediately for cell count, Gram stain, aerobic and anaerobic cultures, and crystal analysis (to rule out gout/pseudogout).
* Macroscopic Appearance: Turbid, opaque, or grossly purulent.
* White Blood Cell (WBC) Count: Typically > 50,000 cells/mm³.
* Differential: > 75% polymorphonuclear leukocytes (PMNs).
* Glucose: Synovial fluid glucose is usually severely depressed (≤ 40 mg/dL) compared to serum glucose.
Microbiology:
Staphylococcus aureus is the most frequently isolated organism in septic hand and wrist joints. However, Streptococcus species, Gram-negative bacilli, and anaerobes (especially in bite wounds) must be considered. Empiric antibiotic therapy should cover MRSA and common Gram-negative organisms until culture sensitivities are finalized.
Operative Technique: Open Drainage of Septic Finger Joints
Septic arthritis of the hand is an absolute surgical emergency. Needle aspiration alone is insufficient for the small, complex joints of the hand; formal open arthrotomy and thorough irrigation are required.
Preoperative Preparation:
* Anesthesia and tourniquet application are identical to the protocol for bursal infections. Do not wrap the arm with an Esmarch bandage. Elevate the arm for gravity exsanguination to prevent proximal seeding of the pathogen.
Approach to the Metacarpophalangeal (MCP) Joint:
1. Incision: Make a longitudinal dorsal incision on either the radial or ulnar side of the metacarpal head.
2. Exposure: Carefully dissect through the subcutaneous tissue. Identify and retract the extensor expansion (sagittal band) distally and laterally to expose the underlying joint capsule.
3. Arthrotomy: Open the joint capsule dorsal to the collateral ligament. The incision must be sufficient to allow free egress of purulence and thorough visualization of the articular surfaces.
4. Debridement: Obtain fluid and tissue for aerobic and anaerobic cultures. Irrigate the joint copiously with normal saline. Debride any frankly necrotic synovium, but preserve the collateral ligaments to maintain joint stability.
5. Closure: Leave the capsular and skin incisions completely open to allow for continuous drainage.
Approach to the Interphalangeal (PIP/DIP) and Thumb MCP Joints:
1. Incision: Utilize a midaxial incision on either the radial or ulnar side of the affected joint. The midaxial line is determined by connecting the apices of the flexion creases when the finger is flexed.
2. Neurovascular Protection: Carefully dissect through the subcutaneous fat. Identify the neurovascular bundle and retract it volarly (toward the palm).
3. Extensor Mechanism: In the fingers, identify the transverse retinacular ligament. Section it longitudinally to allow the lateral band of the extensor mechanism to be retracted dorsally.
4. Arthrotomy via Accessory Collateral Ligament: Identify the true collateral ligament and the accessory collateral ligament. Make a longitudinal incision parallel to the true collateral ligament, positioned palmar to it, effectively separating the accessory collateral ligament from the true collateral ligament.
5. Window Creation: Excise a small portion of the accessory collateral ligament. This creates a dependent "window" that allows for excellent drainage of the joint space without compromising the primary lateral stability provided by the true collateral ligament.
6. Irrigation: Obtain culture specimens. Irrigate the joint space copiously with sterile saline using a blunt needle or angiocatheter to ensure all recesses are flushed.
7. Closure: Leave the wound open. Apply a bulky, non-adherent dressing and a splint in the safe position.
Advanced Reconstruction and Salvage Procedures
In cases of delayed presentation where the articular cartilage has been completely destroyed and osteomyelitis of the underlying phalanx has developed, simple incision and drainage will not suffice.
- Antibiotic Spacers: If the joint and adjacent bone require radical resection, the use of antibiotic-impregnated polymethyl methacrylate (PMMA) spheres (beads) is a highly effective adjunct. As advocated by Asche, and Freeland and Senter, these beads deliver a massive local concentration of antibiotics while maintaining a dead space for future reconstruction.
- Arthrodesis vs. Bone Grafting: Once the infection is definitively eradicated (often requiring 6 weeks of systemic antibiotics and multiple debridements), the joint can be reconstructed via arthrodesis (fusion) using structural bone graft.
- Amputation: In severe cases involving extensive tissue necrosis, vascular compromise, or systemic sepsis, ray amputation or digit amputation may be required to salvage the rest of the hand and protect the patient's life. A chronically infected, stiff, and painful finger retains little useful function and often impedes the function of the adjacent healthy digits; therefore, amputation should not be viewed as a failure, but rather as a definitive functional salvage procedure.
- Pediatric Considerations: In children, the regenerative capacity of tissue is higher. Aggressive, prolonged courses of intravenous antibiotics, repeated surgical drainage, and extended splinting are pursued much longer than in adults in an attempt to salvage the hand and preserve the physes for future growth.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative management of deep hand infections is as critical as the surgical intervention itself.
- Elevation: The hand must be strictly elevated above the level of the heart for the first 24 to 48 hours to minimize edema, which can compromise microvascular perfusion and exacerbate stiffness.
- Wound Care: The initial bulky bandage is typically taken down at 24 hours. Dressings are changed daily or twice daily.
- Continuous Irrigation: If indwelling catheters were placed for bursal infections, continuous or intermittent irrigation with sterile saline is maintained for 48 to 72 hours, or until the effluent is entirely clear and clinical signs of infection have subsided.
- Early Mobilization: Prolonged immobilization of an infected hand guarantees severe, irreversible stiffness. Active and passive motion exercises are initiated immediately after the first dressing change. Exercise periods in a whirlpool bath or under warm running water are highly beneficial for mechanical debridement of the open wounds and for facilitating tendon glide.
- Wound Closure: The surgical incisions are never closed primarily. Once the infection is clinically eradicated and the wound bed is composed of healthy, clean granulation tissue, the wounds may be closed secondarily (delayed primary closure) or, more commonly, allowed to heal by secondary intention.
- Antibiotic Therapy: Intravenous antibiotics are continued postoperatively. The regimen is tailored based on the final culture and sensitivity results. The duration of therapy depends on the severity of the infection and the presence of osteomyelitis, ranging from 7 to 14 days for soft tissue infections, up to 6 weeks for bone involvement.
You Might Also Like
