Ring Sublimis Opponensplasty with Ulnar Collateral Ligament Reconstruction
Key Takeaway
The Kozin and Ezaki ring sublimis opponensplasty combined with ulnar collateral ligament (UCL) reconstruction is a powerful technique for addressing thumb hypoplasia and the rare abducted thumb deformity. This procedure restores thumb opposition, stabilizes the metacarpophalangeal joint, and deepens the first web space. Utilizing the ring finger flexor digitorum superficialis routed through a flexor carpi ulnaris pulley, surgeons can achieve dual-vector dynamic reconstruction.
Introduction to Ring Sublimis Opponensplasty and UCL Reconstruction
The restoration of thumb opposition and metacarpophalangeal (MCP) joint stability is a cornerstone of reconstructive hand surgery, particularly in the setting of congenital thumb hypoplasia or complex neuromuscular deficiencies. The Kozin and Ezaki Ring Sublimis Opponensplasty with Ulnar Collateral Ligament (UCL) Reconstruction is an elegant, highly specialized procedure designed to address a triad of pathological findings: loss of opposition, severe first web space contracture, and chronic UCL laxity or absence.
By utilizing the ring finger flexor digitorum superficialis (FDS) tendon, routed through a meticulously constructed flexor carpi ulnaris (FCU) pulley, the surgeon can achieve a dual-vector reconstruction. The transferred tendon not only acts as a dynamic motor for opposition but is also routed transosseously through the first metacarpal head to anatomically reconstruct the deficient UCL.
This comprehensive guide details the pathoanatomy, biomechanical principles, and step-by-step surgical execution of this advanced technique, tailored for the postgraduate orthopedic and hand surgeon.
Pathoanatomy: The Abducted Thumb Deformity
To fully appreciate the indications for this procedure, one must understand the underlying pathoanatomy of the hypoplastic thumb, specifically the rare variant known as the abducted thumb (pollex abductus).
First described comprehensively by Tupper in 1969, the abducted thumb deformity presents in patients with mild to moderate thumb hypoplasia. Tupper identified that the deformity is primarily driven by an anomalous insertion of the flexor pollicis longus (FPL) muscle into an otherwise normal extensor pollicis longus (EPL) muscle. This aberrant connection creates a pathological vector that causes marked, rigid abduction of the proximal phalanx of the thumb.
Key Clinical Findings in Pollex Abductus
Surgical exploration of these rare cases typically reveals a consistent constellation of anatomical deficiencies:
* Thenar Musculature Deficiency: Hypoplasia or complete aplasia of the abductor pollicis brevis (APB), opponens pollicis, and superficial head of the flexor pollicis brevis (FPB).
* First Web Space Contracture: Severe adduction contracture of the first metacarpal, resulting in a critically narrowed thumb-index web space.
* Ligamentous Incompetence: Marked laxity or absence of the ulnar collateral ligament of the MCP joint.
* Tendon Displacement: Radial and superficial displacement of the FPL tendon.
* Joint Dysfunction: An inability to actively flex the interphalangeal (IP) joint of the thumb due to the anomalous FPL-EPL tethering.
Historical Treatment Context
Historically, numerous surgical interventions have been proposed for the abducted thumb. These include the release of the bifurcated tendon insertion with reattachment to the metacarpal neck, or distal release with withdrawal at the wrist and reattachment to the distal phalanx. Other approaches involve releasing the anomalous slip to the EPL combined with an ulnarward shift of the EPL at the MCP joint.
Regardless of the specific tendon routing, all successful procedures share a common requirement: release of the radial collateral ligament, reefing or reconstruction of the ulnar collateral ligament, deepening of the web space, and a secondary opponensplasty. The Kozin and Ezaki technique elegantly consolidates these requirements into a single, unified operation.
Biomechanics of the Transfer
The success of the ring sublimis opponensplasty relies on precise biomechanical vectors.
- The Motor (Ring FDS): The FDS of the ring finger is selected due to its expendability, adequate excursion (approximately 3-4 cm), and sufficient length to reach the thumb MCP joint. Its independent muscle belly allows for relatively straightforward cortical re-education postoperatively.
- The Pulley (FCU Loop): To achieve true opposition (abduction, flexion, and pronation of the first metacarpal), the line of pull must originate from the region of the pisiform. By creating a loop from the distal FCU, the FDS tendon is redirected ulnarly and volarly. This vector perfectly mimics the native APB and opponens pollicis.
- The Dual-Tail Insertion: Unlike standard opponensplasties that insert solely onto the APB insertion or radial proximal phalanx, this technique routes the tendon through the metacarpal head. The radial fixation provides the pronation/abduction moment for opposition, while the continuation of the tendon to the ulnar base of the proximal phalanx reconstructs the UCL, preventing the MCP joint from collapsing into radial deviation during pinch.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia or regional brachial plexus block.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg (or 100 mm Hg above systolic pressure) after exsanguination.
- Equipment: Loupe magnification (2.5x to 3.5x), mini-C-arm fluoroscopy, 0.45-inch (1.14 mm) Kirschner wires, and a Jurgan Pin Ball system.
⚠️ Surgical Warning
Thoroughly assess the presence and independent function of the flexor digitorum profundus (FDP) to the ring finger prior to harvesting the FDS. Harvesting the FDS in the presence of an incompetent FDP will result in a devastating loss of active proximal interphalangeal (PIP) and distal interphalangeal (DIP) joint flexion.
Surgical Technique: Step-by-Step
Step 1: Incisions and Web Space Deepening
The procedure begins with addressing the adduction contracture of the first metacarpal.
To widen the narrow thumb-index web space, design a four-flap Z-plasty. The central limb of the Z-plasty is placed along the crest of the contracted web space. Extend the radial limb proximally to expose the ulnar collateral ligament and the metacarpophalangeal joint.
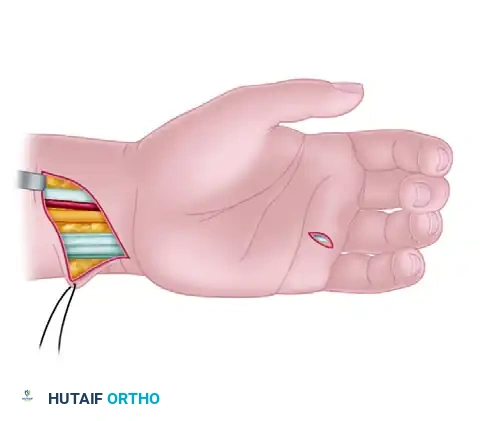
Make a short oblique incision at the volar base of the ring finger to access the FDS tendon. Next, create a zigzag or oblique incision along the ulnar portion of the volar forearm, extending proximally from the wrist crease, to isolate the flexor carpi ulnaris (FCU) tendon and retrieve the FDS. Finally, make an additional longitudinal skin incision along the radial side of the thumb MCP joint to expose the site for the FDS tendon attachment.

Step 2: Ring Finger FDS Harvest
Identify the ring finger FDS tendon at the base of the finger through the short oblique incision. Carefully dissect the tendon, ensuring the underlying FDP tendon is protected.
Tag the FDS with a core suture (e.g., 3-0 Prolene or braided non-absorbable suture) and transect it as distally as possible at the base of the ring finger, proximal to Camper's chiasm.
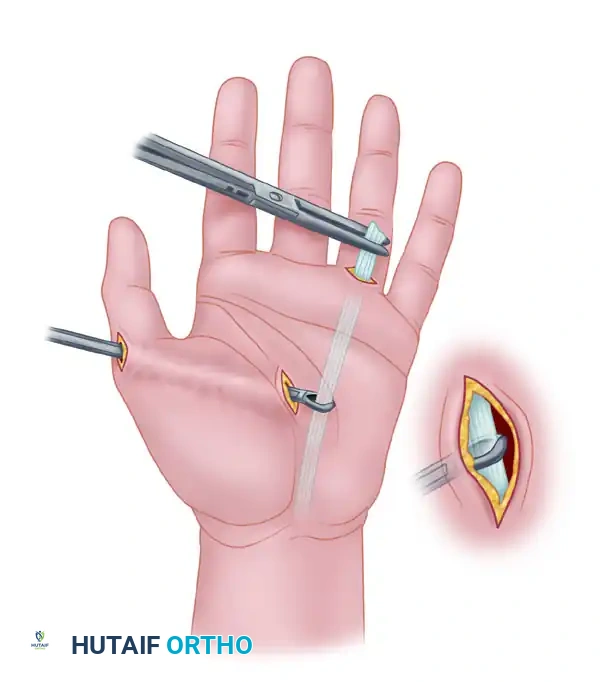
Move to the forearm incision. Identify the ring FDS muscle belly and tendon within the distal forearm. Place a curved hemostat or forceps around the FDS tendon in the forearm and use it to gently roll and withdraw the tendon proximally through the carpal tunnel and into the forearm wound.
Step 3: FCU Pulley Construction
To establish the correct vector for opposition, a pulley must be constructed at the ulnar aspect of the wrist.
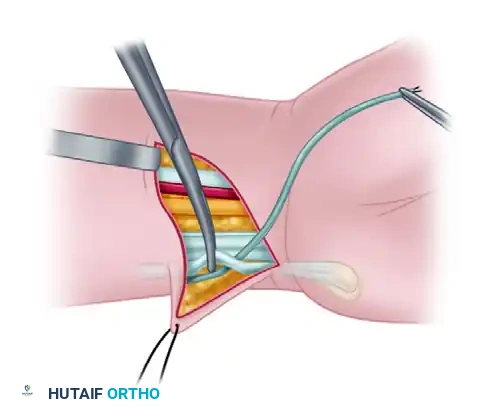
Isolate the distal 2 to 3 cm of the FCU tendon. Longitudinally split the tendon, harvesting one-half of its width while meticulously preserving its distal attachment to the pisiform. Pass the harvested, proximally based half through the retained, intact FCU tendon just proximal to the pisiform to create a robust loop. Suture the tendon weave onto itself using a nonabsorbable braided suture (e.g., 3-0 Ethibond or Ticron) to secure the pulley.
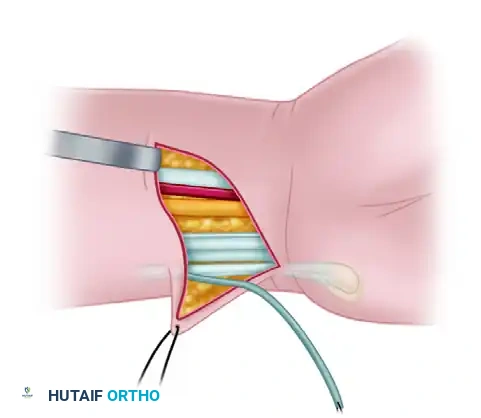
Once the pulley is secure, pass the tagged end of the ring finger FDS tendon through the newly constructed FCU loop. Ensure the FDS glides smoothly without catching.
Step 4: Subcutaneous Tunneling
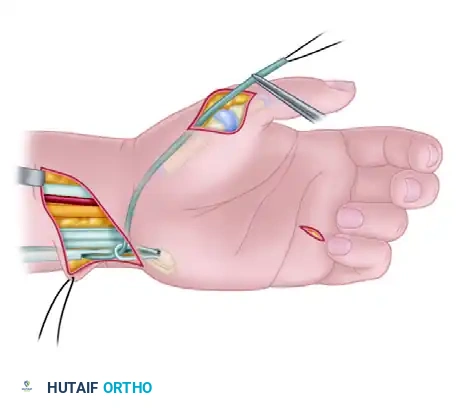
Create a wide subcutaneous tunnel connecting the volar forearm incision to the radial side of the thumb incision. This tunnel must be superficial to the flexor retinaculum but deep to the subcutaneous fat to prevent bowstringing or skin tethering.
Pass the FDS tendon through this subcutaneous tunnel, directing it from the FCU pulley to the radial aspect of the thumb MCP joint.
Step 5: Metacarpal Preparation and Joint Stabilization
Attention is now turned to the thumb MCP joint. Isolate the first metacarpal head, elevating the periosteum minimally to preserve vascularity.
Using a 0.45-inch (1.14 mm) Kirschner wire, drill a transverse hole across the metacarpal head, parallel to the joint surface. Utilize mini-fluoroscopy to ensure precise intraosseous placement. Direct the wire from the volar aspect of the radial side of the metacarpal to the ulnar and dorsal aspects. Enlarge this pilot hole with a cannulated drill bit or a slightly larger drill to allow smooth passage of the FDS tendon.

Before passing the tendon, reduce the MCP joint into neutral alignment. Stabilize the joint by driving a longitudinal 0.45-inch Kirschner wire antegrade from the tip of the thumb, across the IP and MCP joints, into the first metacarpal shaft. Cut the wire short outside the skin and apply a Jurgan Pin Ball (RFO Medical, London, UK) to prevent migration and protect the patient.
Step 6: Tendon Passage and UCL Reconstruction
Pass the FDS tendon through the prepared transosseous drill hole in the metacarpal head, routing it from the radial side to the ulnar side of the thumb.
💡 Clinical Pearl
If the FDS tendon is too bulky to pass through the metacarpal head without risking an iatrogenic fracture, one of the two FDS slips can be excised longitudinally to reduce the tendon's diameter while maintaining adequate tensile strength.

Setting the Tension:
Place the wrist into slight extension (approximately 20 to 30 degrees). Apply traction to the FDS tendon until the thumb is drawn into full opposition (abduction and pronation). Utilize the tenodesis effect to assess the resting tension: passive wrist flexion should relax the thumb, while passive wrist extension should drive the thumb into opposition.
Once the correct tension is achieved, suture the FDS tendon securely to the surrounding bone and robust periosteum at the radial entry point of the metacarpal head. This critical maneuver sets the primary tension for the opponensplasty.
UCL Reconstruction:
Take the remaining length of the FDS tendon exiting the ulnar side of the metacarpal head and direct it distally toward the base of the proximal phalanx. This segment will reconstruct the incompetent UCL.
Suture the tendon directly onto the ulnar base of the proximal phalanx using strong nonabsorbable sutures or a micro-suture anchor. In most cases, there is adequate tendon length to pass the extra FDS tendon back onto itself, creating a double-stranded, highly stable ligamentous repair.
Step 7: Closure
Deflate the tourniquet and achieve meticulous hemostasis. Close the four-flap Z-plasty in the web space, ensuring no tension on the skin flaps. Close the forearm and finger incisions with absorbable sutures (e.g., 4-0 or 5-0 Monocryl or chromic gut).
Apply sterile, non-adherent dressings and immobilize the limb in a well-molded, long-arm thumb spica cast. Ensure the wrist is positioned in slight flexion to relieve tension on the transfer, and the thumb is held in wide abduction and opposition.
Postoperative Care and Rehabilitation Protocol
The success of a tendon transfer relies heavily on strict adherence to postoperative rehabilitation.
- Weeks 0-3: The patient remains strictly immobilized in the long-arm thumb spica cast. Elevation and digital motion of the uninvolved fingers are encouraged to prevent stiffness and reduce edema.
- Week 3: The long-arm cast is removed. The longitudinal Kirschner wire stabilizing the MCP joint is extracted in the clinic. A custom-molded, short-arm thumb spica splint is fabricated.
- Weeks 3-6: Active range of motion (AROM) and tendon transfer re-education therapy are initiated. The patient is instructed to actively flex the ring finger to initiate thumb opposition. The splint is worn at all times between exercise sessions and at night.
- Weeks 6-8: Passive range of motion (PROM) is cautiously introduced if joint stiffness is present, though care must be taken not to stretch the UCL reconstruction.
- Weeks 8-12: Progressive strengthening and pinch-grip exercises are commenced. The splint is gradually weaned for light activities.
- Months 3+: Return to unrestricted activities, though heavy gripping or high-impact loading of the thumb should be avoided until 4 to 6 months postoperatively.
Complications and Pitfalls
- Over-tensioning or Under-tensioning: Incorrect tensioning is the most common cause of transfer failure. Over-tensioning leads to a fixed flexion/adduction contracture, while under-tensioning results in a weak, lagging opposition. Relying on the tenodesis effect intraoperatively is vital.
- Pin Tract Infection: The longitudinal K-wire crossing the MCP joint is a conduit for infection. Meticulous pin care and the use of a Jurgan Pin Ball reduce this risk. If erythema develops, early oral antibiotics are indicated.
- Web Space Contracture Recurrence: Inadequate release of the adductor pollicis fascia or failure of the Z-plasty flaps can lead to recurrent narrowing. Ensure the Z-plasty flaps are designed with adequate length and angles (typically 60 to 90 degrees) to maximize web space deepening.
- Pulley Failure: If the FCU loop is not sutured securely, the FDS tendon can bowstring ulnarly, altering the vector of pull and severely diminishing the mechanical advantage of the opponensplasty. Ensure a robust tendon weave is utilized.
You Might Also Like