Metacarpophalangeal Arthroplasty: Comprehensive Surgical Techniques and Protocols
Key Takeaway
Metacarpophalangeal (MCP) arthroplasty is a critical surgical intervention primarily indicated for severe rheumatoid arthritis or posttraumatic joint destruction. This procedure utilizes silicone elastomer implants to restore functional kinematics, correct ulnar drift, and alleviate debilitating pain. Success relies on meticulous soft tissue balancing, precise bone resection preserving the metaphyseal flare, and rigorous postoperative rehabilitation to ensure implant longevity and optimal hand function.
INTRODUCTION TO METACARPOPHALANGEAL ARTHROPLASTY
Metacarpophalangeal (MCP) arthroplasty remains a cornerstone in the surgical management of advanced joint destruction, most notably in the context of severe rheumatoid arthritis (RA) and posttraumatic osteoarthritis. The primary goals of this procedure are the alleviation of debilitating pain, the correction of complex deformities (such as ulnar drift and volar subluxation), and the restoration of functional kinematics to the hand.
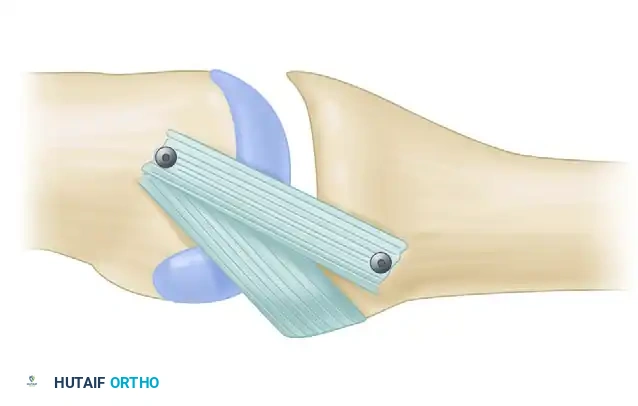
Historically pioneered by Alfred Swanson, the use of silicone elastomer implants acts not as a true joint replacement, but rather as a dynamic spacer. This spacer maintains joint alignment while a fibrous pseudocapsule forms, ultimately providing the necessary stability and mobility. Mastery of this procedure requires a profound understanding of hand biomechanics, meticulous soft tissue handling, and precise osseous preparation.
💡 Clinical Pearl: The Dynamic Spacer Concept
Silicone implant arthroplasty relies on the "encapsulation process." The implant itself does not bear the physiological loads of a normal joint; rather, it acts as an internal mold around which the body forms a new, organized fibrous capsule. Preserving the collateral ligaments and meticulously repairing the extensor mechanism are paramount, as the soft tissues—not the implant—provide ultimate joint stability.
PATHOPHYSIOLOGY AND INDICATIONS
Rheumatoid Arthritis and Joint Destruction
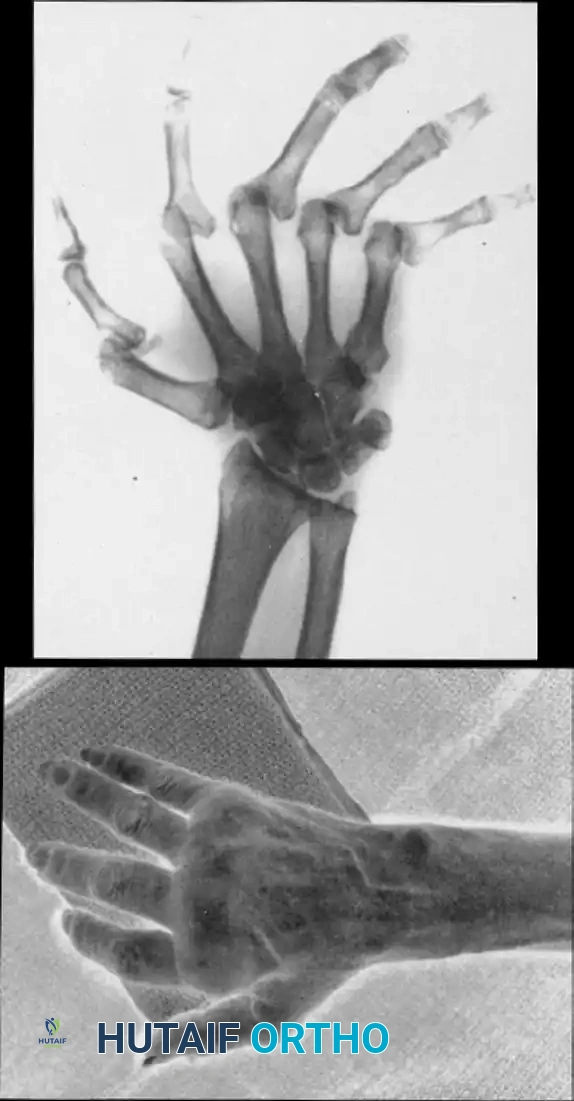
In the rheumatoid hand, chronic synovitis leads to the attenuation of the radial sagittal bands and collateral ligaments, resulting in the characteristic volar subluxation and ulnar deviation of the digits. In the thumb, this often presents as a Type I deformity (boutonnière deformity), characterized by MCP joint flexion and interphalangeal (IP) joint hyperextension.
FIGURE 73-34 A and B: Preoperative clinical and radiographic presentation of a Type I thumb deformity, demonstrating fixed finger metacarpophalangeal joint subluxations with severe degenerative changes and ulnar translocation of the wrist, alongside a relatively preserved midcarpal joint.
Primary Indications
- Rheumatoid Arthritis: Severe, fixed deformities with unremitting pain and loss of function.
- Osteoarthritis: Advanced degenerative changes unresponsive to conservative management, particularly in older, lower-demand patients.
- Posttraumatic Arthritis: Joint destruction following intra-articular fractures or chronic dislocations.
Contraindications
- Active or recent local infection.
- Inadequate bone stock to support the implant stems.
- Irreparable soft tissue coverage or absent motor units (unless concurrent tendon transfers are planned).
- High-demand, heavy manual laborers (due to the risk of premature silicone implant fracture or subsidence).
PREOPERATIVE PLANNING AND BIOMECHANICS
Radiographic Templating
Standard posteroanterior (PA), lateral, and oblique radiographs of the hand and wrist are mandatory. Templating is utilized to estimate the size of the medullary canals of the metacarpal and proximal phalanx. The surgeon must assess the degree of bone loss, the presence of cystic changes, and the overall alignment of the carpus, as proximal instability (e.g., ulnar translocation of the carpus) can compromise distal surgical outcomes.
Biomechanical Considerations
The MCP joint is a condyloid joint allowing flexion, extension, abduction, adduction, and circumduction. During arthroplasty, the center of rotation is often slightly altered. The silicone implant must be seated perfectly flush against the resected bone ends to prevent sheer stresses that lead to implant fracture. If the bony surfaces are irregular or cystic, titanium grommets may be utilized to shield the silicone hinge from sharp osseous edges, thereby reducing the risk of abrasive wear and subsequent silicone synovitis.
SURGICAL TECHNIQUE: THUMB METACARPOPHALANGEAL ARTHROPLASTY
The following step-by-step technique details the approach for a thumb MCP arthroplasty, addressing the specific anatomical nuances of the extensor pollicis longus (EPL) and extensor pollicis brevis (EPB).
1. Positioning and Exposure
- Anesthesia: Regional block (supraclavicular or axillary) or general anesthesia.
- Positioning: Supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the upper arm and inflated to 250 mm Hg after exsanguination.
- Incision: Expose the metacarpophalangeal joint through a longitudinal dorsal oblique or gently curved incision centered over the joint. This approach avoids scar contracture directly over the flexion crease and provides excellent access to the extensor mechanism.
2. Extensor Mechanism Release
- Carefully dissect the subcutaneous tissues, preserving the dorsal sensory branches of the radial nerve.
- Identify the extensor apparatus. Release the extensor pollicis longus (EPL) from the extensor expansions on each side.
- Identify and release the extensor pollicis brevis (EPB) from its insertion at the base of the proximal phalanx. Tag the EPB with a non-absorbable suture for later reattachment.
3. Joint Preparation and Bone Resection
- Perform a dorsal capsulotomy to expose the articular surfaces.
- Metacarpal Resection: Resect the metacarpal head perpendicular to the long axis of the metacarpal shaft. It is critical to leave the metaphyseal flare of the metacarpal intact to provide a broad, stable base for the implant hinge.
- Ligament Preservation: Meticulously preserve the collateral ligaments. Unlike some aggressive resections in the past, modern techniques emphasize retaining these structures to ensure postoperative coronal plane stability.
🚨 Surgical Warning: Managing Flexion Contractures
If a severe flexion contracture persists after the initial metacarpal head resection, do not simply resect more bone. Instead, partially release the collateral ligaments proximally from their metacarpal origins and perform a sequential release of the volar plate. Excessive bone resection compromises the metaphyseal flare and leads to implant subsidence.
- Proximal Phalanx Preparation: Leave the base of the proximal phalanx intact whenever possible. However, if additional space is required to accommodate the hinge of the prosthesis without buckling, remove a minimal portion of the articular cartilage and subchondral bone using an oscillating saw or rongeur.
4. Canal Preparation and Trialing
- Utilize specialized broaches and reamers to prepare the medullary canals of both the metacarpal and the proximal phalanx.
- Insert temporary trial prostheses to determine the optimal size. The goal is to select the largest size that the metacarpal shaft will comfortably accept without causing cortical fracturing. The implant stems should fit snugly, and the central hinge should sit flush against the resected bone surfaces.
5. Preparation for Soft Tissue Reconstruction
- Before inserting the final implant, prepare the proximal phalanx for the reattachment of the EPB.
- Drill small osseous holes in the dorsal base of the proximal phalanx.
- Pass a robust, non-absorbable suture (e.g., 2-0 FiberWire or Ethibond) through these holes so that it is pre-positioned for the reattachment of the EPB after the prosthesis has been seated.
6. Implant Insertion
- Thoroughly irrigate the medullary canals to remove bone debris and marrow fat.
- Insert the final silicone implant using a "no-touch" technique with smooth forceps to avoid scratching the elastomer, which can create stress risers and lead to premature failure.
- Optional: If needed due to irregular, sharp, or cystic bony surfaces, insert metal sleeve "grommets" into the canals prior to the silicone implant. These titanium shields protect the silicone hinge from abrasive shear forces.
7. Soft Tissue Reconstruction and Closure
- EPB Reattachment: Reattach the extensor pollicis brevis to the pre-drilled holes in the proximal phalanx. Ensure this is done under sufficient tension to allow robust proximal phalangeal extension.
- Extensor Expansion Repair: Repair the extensor expansion meticulously over the insertion of the EPB tendon.
- EPL Advancement: Advance and repair the extensor pollicis longus tendon, ensuring it is perfectly centered over the extensor expansion to prevent postoperative subluxation.
- Distal Joint Management: Assess the interphalangeal (IP) joint. If severe hyperextension or instability is present (common in Type I deformities), pin the distal joint with a smooth Kirschner wire, or perform a concurrent IP joint arthrodesis.
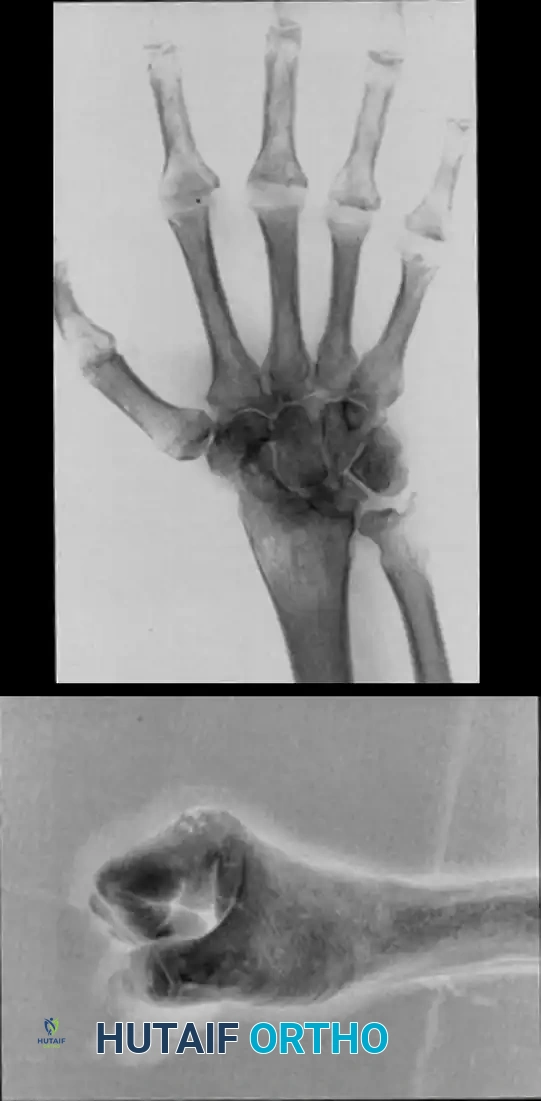
FIGURE 73-34 C and D: Postoperative radiographic appearance demonstrating successful radioscapholunate fusion, metacarpophalangeal implant arthroplasty with excellent implant seating, and concurrent thumb interphalangeal joint fusion to correct complex rheumatoid deformities.
- Closure: Deflate the tourniquet, achieve meticulous hemostasis, and close the skin with non-absorbable sutures.
- Immobilization: Apply a bulky, sterile compressive dressing and a volar splint to immobilize the hand and thumb, ensuring the metacarpophalangeal joint is held securely in extension.
POSTOPERATIVE CARE AND REHABILITATION
The success of an MCP arthroplasty is heavily dependent on a rigorous, well-supervised postoperative rehabilitation protocol. The goal is to guide the formation of the encapsulating scar tissue while preventing recurrent deformity.
Phase I: Immediate Postoperative (Days 1 to 14)
- Strict elevation of the operative extremity to minimize edema.
- The initial surgical splint remains intact.
- Suture Removal: Sutures are removed when the wound permits, typically between 10 to 14 days postoperatively.
Phase II: Early Mobilization (Weeks 2 to 4)
- Following suture removal, a custom thermoplastic splint is applied over the metacarpophalangeal joint to hold it in extension.
- The metacarpophalangeal joint is continuously splinted in extension for 3 to 4 weeks to protect the extensor mechanism repair and allow the volar capsule to heal, preventing recurrent flexion contractures.
- Interphalangeal Motion: Active and passive interphalangeal joint motion is highly encouraged during this phase to prevent tendon adhesions and maintain distal glide.
Phase III: Strengthening and Weaning (Weeks 4 to 8)
- The rigid extension splint is gradually weaned, often transitioning to a dynamic extension splint during the day to allow active flexion while assisting extension.
- Night splinting in extension is continued for up to 12 weeks.
- Forceful, strenuous activities, heavy lifting, and tight gripping are strictly avoided for at least 6 to 8 weeks to prevent implant fracture or subsidence before the fibrous capsule has fully matured.
TRAPEZIOMETACARPAL LIGAMENT RECONSTRUCTION
While MCP arthroplasty addresses the distal aspect of the thumb ray, proximal pathology at the trapeziometacarpal (TMC) joint frequently requires concurrent or isolated management.
Indications and Patient Selection
Trapeziometacarpal soft tissue reconstruction (such as the Eaton-Littler ligament reconstruction using the flexor carpi radialis tendon) is primarily utilized for posttraumatic ligamentous laxity related to recurrent dislocation.
Reconstruction of the trapeziometacarpal volar beak ligament in patients with hypermobile, prearthritic joints may provide significant pain relief and reduce the chance of future progression of trapeziometacarpal osteoarthritis. By stabilizing the base of the metacarpal, the abnormal shear forces across the articular cartilage are mitigated.
💡 Clinical Pearl: Rheumatoid vs. Osteoarthritic TMC Joints
Ligament reconstruction is rarely indicated for laxity related to rheumatoid changes. In the rheumatoid patient, the systemic inflammatory destruction of the articular cartilage and subchondral bone makes soft-tissue-only procedures prone to failure. For rheumatoid TMC pathology, excisional arthroplasty (with or without suspensionplasty) or arthrodesis are significantly better, more durable options.
Radiographic Outcomes of Trapeziometacarpal Procedures
When simple trapezium excision is performed without robust ligamentous suspension, proximal migration (settling) of the first metacarpal is a known biomechanical consequence.
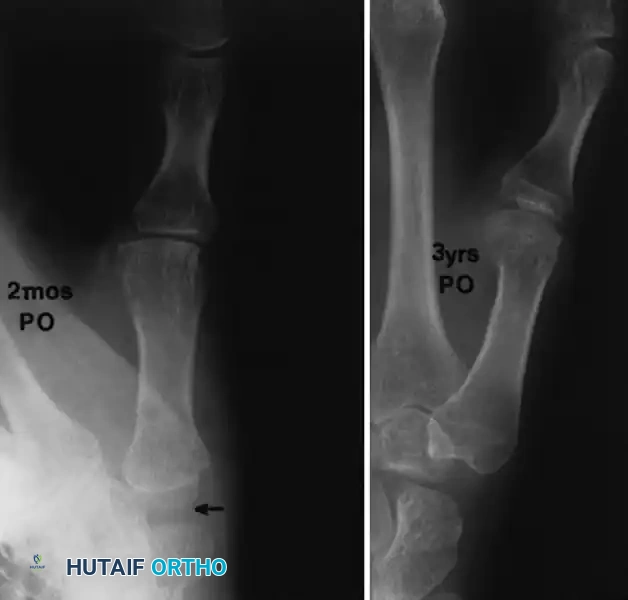
FIGURE 73-35: Radiographic progression at 2 months and at 3 years after simple trapezium excision (arrow). Note the progressive metacarpal settling and resultant scaphometacarpal space narrowing; however, clinically, the thumb often remains functionally stable despite this radiographic appearance.
COMPLICATIONS AND SALVAGE PROCEDURES
Despite meticulous surgical technique, complications in MCP arthroplasty can occur, particularly given the fragile soft tissue envelope and poor bone stock often seen in the rheumatoid population.
- Implant Fracture: Silicone elastomers are susceptible to fatigue failure over time. While modern high-performance silicones have reduced this rate, fractures still occur. Interestingly, a fractured implant does not always correlate with clinical failure, as the mature fibrous pseudocapsule often maintains adequate joint stability. Revision is only indicated if the fracture is accompanied by pain, severe recurrent deformity, or loss of function.
- Infection: Deep periprosthetic infection is a devastating complication requiring immediate implant removal, aggressive surgical debridement, and targeted intravenous antibiotic therapy. Once the infection is eradicated, the joint is typically left as a resection arthroplasty, or a delayed arthrodesis is performed.
- Recurrent Deformity: Ulnar drift or volar subluxation can recur if the initial soft tissue balancing was inadequate, or if the patient fails to adhere to the postoperative splinting protocol. Revision soft tissue reconstruction is technically demanding and yields inferior results compared to the primary procedure.
- Silicone Synovitis: Micro-particulate shedding from the silicone implant can induce a foreign-body giant cell reaction, leading to erosive synovitis and cystic bone destruction. The use of titanium grommets has been shown to decrease the incidence of this complication by protecting the implant hinge from sharp bone edges.
CONCLUSION
Metacarpophalangeal arthroplasty remains a highly effective, life-altering procedure for patients suffering from end-stage joint destruction. By adhering to strict biomechanical principles—preserving the metacarpal metaphyseal flare, meticulously balancing the extensor mechanism, and enforcing a rigid postoperative rehabilitation protocol—the orthopedic surgeon can reliably restore function, correct severe deformities, and provide lasting pain relief. Continuous advancements in implant materials and joint kinematics will further refine this essential technique in the armamentarium of hand surgery.
📚 Medical References
- Metacarpophalangeal arthroplasty in rheumatoid arthritis: what determines satisfaction with surgery? J Rheumatol 29:2488, 2002.
- Melone CP, McLoughlin JC, Beldner SM: Surgical management of the hand in scleroderma, Curr Opin Rheumatol 11:514, 1999.
- Nalebuff EA: Surgery of psoriatic arthritis of the hand, Hand Clin 12:603, 1996.
- Nalebuff EA: Surgery of systemic lupus erythematosus arthritis of the hand, Hand Clin 12:591, 1996.
- Nalebuff EA, Feldon PG, Millender LH: Rheumatoid arthritis. In Green DP, ed: Operative hand surgery, New York, 1982, Churchill Livingstone. O’Brien ET: Surgical principles and planning for the rheumatoid hand and wrist, Clin Plast Surg 23:407, 1996.
- Pelligrini VD: Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration: I. Anatomy and pathology of the aging joint, J Hand Surg 16A:967, 1991.
- Pelligrini VD: Osteoarthritis of the trapeziometacarpal joint: the pathophysiology of articular cartilage degeneration: II. Articular wear patterns in the osteoarthritic joint, J Hand Surg 16A:975, 1991.
- Pomerance JF: Painful basal joint arthritis of the thumb: I. Anatomy, pathophysiology, and diagnosis, Am J Orthop 24:401, 1995.
- Rizio L, Belsky MR: Finger deformities in rheumatoid arthritis, Hand Clin 12:531, 1996.
- Savill DL: Assessment of the rheumatoid hand for reparative and reconstructive surgery, J Bone Joint Surg 46B:786, 1964.
- Simmons BP, Nutting JT: Juvenile rheumatoid arthritis, Hand Clin 5:157, 1989.
- Souter WA: Planning treatment of the rheumatoid hand, Hand 11:3, 1979.
- Stein AB, Terrono AL: The rheumatoid thumb, Hand Clin 12:541, 1996.
- Swigart CR, Eaton RG, Glickel SZ, et al: Splinting in the treatment of arthritis of the fi rst carpometacarpal joint, J Hand Surg 24A:86, 1999.
- van Lankveld W, van’t Pad Bosch P, van der Schaaf D, et al: Evaluating hand surgery in patients with rheumatoid arthritis: short-term effect on dexterity and pain and its relationship with patient satisfaction, J Hand Surg 25:921, 2000.
- Walton RL, Brown RE, Giansiracusa DF: Psoriatic arthritis mutilans: digital distraction lengthening: pathophysiologic and current therapeutic review, J Hand Surg 13A:510, 1988.
- Wilgis EF: Digital sympathectomy for vascular insuffi ciency, Hand Clin 1:361, 1985.
- Zancolli EA, Ziadenberg C, Zancolli E Jr: Biomechanics of the trapeziometacarpal joint, Clin Orthop Relat Res 220:14, 1987.
- Arthritis Soft-Tissue Procedures Barbier O, Chryssagi AM, Hugon S, et al: Prospective functional analysis of trapeziectomy combined with intermetacarpal tendon stabilization in trapeziometacarpal arthritis, Acta Orthop Belg 70:410, 2004.
- Bora FW, Osterman AL, Thomas VJ, et al: The treatment of ruptures of multiple extensor tendons at wrist level by a free tendon graft in the rheumatoid patient, J Hand Surg 12A:1038, 1987.
- Boyer MI, Gelberman RH: Operative correction of swan-neck and boutonniere deformities in the rheumatoid hand, J Am Acad Orthop Surg 7:92, 1999.
- Brown FE, Brown ML: Long-term results after tenosynovectomy to treat the rheumatoid hand, J Hand Surg 13A:704, 1988.
- Clayton ML, Ferlic DC: The wrist in rheumatoid arthritis, Clin Orthop Relat Res 106:192, 1975.
- Coons MS, Green SM: Boutonniere deformity, Hand Clin 11:387, 1995.
- De Smet L, Sioen W, Spaepen D, et al: Treatment of basal joint arthritis of the thumb: trapeziectomy with or without tendon interposition/
You Might Also Like