Abductor Digiti Quinti Opponensplasty & Thumb Reconstruction
Key Takeaway
The abductor digiti quinti (Huber) opponensplasty is a highly effective tendon transfer utilized to restore thumb opposition, particularly in congenital hypoplasia. By mobilizing the abductor digiti quinti on its neurovascular pedicle and transferring it to the thenar eminence, surgeons can reconstruct the functional mechanics of the abductor pollicis brevis. This guide details the surgical technique, neurovascular preservation, and postoperative protocols essential for optimal outcomes.
INTRODUCTION TO THUMB OPPOSITION RECONSTRUCTION
The restoration of thumb opposition is a cornerstone of reconstructive hand surgery. Opposition is a complex, multi-planar movement requiring abduction, flexion, and pronation of the first metacarpal, primarily driven by the abductor pollicis brevis (APB), opponens pollicis, and superficial head of the flexor pollicis brevis (FPB). In cases of congenital thumb hypoplasia (e.g., Blauth Types II and IIIA) or severe median nerve palsy, the intrinsic thenar musculature is often absent or profoundly deficient.
The Abductor Digiti Quinti (ADQ) Opponensplasty, originally described by Huber in 1921 and later refined by Littler and Cooley, represents a uniquely elegant solution. Unlike traditional tendon transfers (such as the flexor digitorum superficialis or extensor indicis proprius transfers), the Huber procedure transfers a fully vascularized, innervated muscle belly. Because the ADQ is anatomically and biomechanically a mirror image of the APB, transferring it to the thenar eminence not only restores the critical vector of opposition but also reconstructs the aesthetic bulk of the deficient thenar cone.
This comprehensive guide details the operative execution of the ADQ opponensplasty, the management of the severely deficient "floating thumb" (pouce flottant), and the staged reconstruction of severe first web space contractures.
ABDUCTOR DIGITI QUINTI OPPONENSPLASTY (HUBER; LITTLER AND COOLEY)
Indications and Patient Selection
The ADQ opponensplasty is primarily indicated for:
* Congenital Thumb Hypoplasia: Specifically Blauth Type II and Type IIIA, where the carpometacarpal (CMC) joint is stable, but thenar intrinsic muscles are absent or severely hypoplastic.
* Severe Median Nerve Palsy: Cases where restoration of thenar bulk is desired alongside functional opposition, particularly in younger patients or those with significant cosmetic concerns regarding thenar atrophy.
* Traumatic Thenar Loss: Reconstruction following severe crush injuries or tumor resections that obliterate the thenar compartment.
Surgical Anatomy and Biomechanics
The abductor digiti quinti originates from the pisiform bone and the tendon of the flexor carpi ulnaris (FCU). It inserts distally via two tendinous slips: one into the ulnar base of the proximal phalanx of the small finger, and the other into the ulnar lateral band of the extensor expansion.
The muscle is supplied by the deep branch of the ulnar nerve and vascularized by branches of the ulnar artery. The neurovascular hilum enters the deep surface of the muscle in its proximal third. Biomechanically, by releasing the pisiform origin but retaining the FCU fascial origin, the FCU acts as a stable proximal anchor. When the muscle is folded 170 degrees and tunneled to the thumb, the line of pull perfectly replicates the APB, providing palmar abduction and pronation.
💡 Clinical Pearl: The "Mirror Image" Concept
The ADQ is the hypothenar mirror image of the thenar APB. By rotating the muscle 170 degrees on its longitudinal axis (like turning the page of a book), the deep surface becomes superficial. This maneuver not only aligns the muscle fibers to replicate the APB's vector but also safely positions the neurovascular pedicle without kinking or excessive tension.
Preoperative Preparation and Positioning
- Anesthesia: General anesthesia or regional brachial plexus block.
- Positioning: Supine with the operative arm extended on a radiolucent hand table.
- Tourniquet: A well-padded pneumatic upper arm tourniquet is applied and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
- Loupe Magnification: Essential (typically 2.5x to 3.5x) for meticulous dissection of the neurovascular pedicle.
🔪 Surgical Technique: Step-by-Step
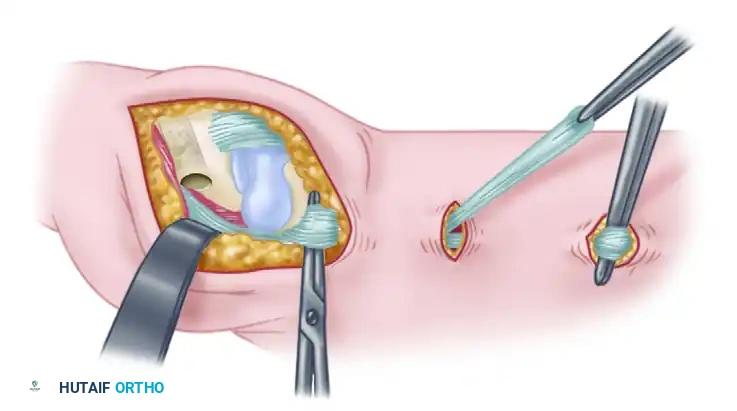
1. Hypothenar Incision and Exposure
- Make a curved palmar incision along the radial border of the abductor digiti quinti muscle belly.
- The incision should extend from the proximal side of the pisiform proximally, curving gently to the ulnar border of the little finger distally at the level of the metacarpophalangeal (MCP) joint.
- Elevate the skin flaps carefully, preserving the superficial sensory branches of the ulnar nerve.
2. Distal Release of the ADQ
- Identify the distal insertions of the ADQ.
- Free both tendinous insertions of the muscle: release one slip from the extensor expansion (hood) and the other from the ulnar base of the proximal phalanx.
- Tag the distal tendons with a 4-0 non-absorbable suture for later manipulation. Securing both slips ensures adequate length for the transfer.
3. Muscle Mobilization and Neurovascular Isolation
- Lift the muscle belly from its hypothenar fascial compartment.
- Proceed with extreme caution during the elevation of the proximal third of the muscle to expose its neurovascular bundle.
- Isolate the neurovascular bundle entering the deep, radial aspect of the muscle.
- CRITICAL STEP: Take meticulous care not to damage the delicate venae comitantes. Venous congestion is a primary cause of failure in muscle belly transfers.
4. Proximal Release
- Free the origin of the muscle from the pisiform bone using sharp dissection.
- Retain the origin on the flexor carpi ulnaris (FCU) tendon. This retained fascial attachment provides the necessary proximal counter-tension and acts as the new functional origin for the transferred muscle.
- Once the pisiform origin is released, the muscle can be mobilized sufficiently for its distal insertion to reach the thumb without tension.
5. Thenar Preparation and Subcutaneous Tunneling
- Make a separate curved incision on the radial border of the thenar eminence, exposing the insertion site of the deficient abductor pollicis brevis at the radial base of the thumb proximal phalanx.
- Create a wide subcutaneous pocket across the palm to receive the transfer.
- The tunnel must be capacious; a tight tunnel will compress the muscle belly, leading to ischemia, venous congestion, and subsequent fibrosis or necrosis.
6. Muscle Transfer and Fixation
- Fold the abductor digiti quinti muscle over approximately 170 degrees (described classically as turning a "page of a book").
- Pass the muscle subcutaneously through the palmar tunnel to the thumb.
- Assess the tension. The thumb should be held in full palmar abduction and opposition.
- Suture the transferred ADQ tendons of insertion to the anatomical insertion of the abductor pollicis brevis (and the radial lateral band of the extensor mechanism, if necessary to assist with interphalangeal joint extension). Use 3-0 or 4-0 non-absorbable braided sutures.
⚠️ Surgical Warning: Pedicle Tension
Throughout the entire procedure—especially during the tunneling and fixation phases—avoid any compression of, or undue tension on, the muscle belly and its neurovascular pedicle. Verify that the pedicle is not twisted or kinked after the 170-degree rotation. Deflate the tourniquet prior to final skin closure to confirm robust perfusion of the transferred muscle belly.
Postoperative Care and Rehabilitation
- Immediate Postoperative Phase: Apply a carefully formed, light compression dressing. Immobilize the extremity in a well-padded volar plaster splint or a thumb spica cast. The thumb must be held in maximum palmar abduction and opposition, with the wrist in slight flexion (approximately 20 degrees) to relieve tension on the transfer.
- Immobilization Period: The rigid plaster splint is maintained for exactly 4 weeks.
- Rehabilitation Phase (Weeks 4-12): At 4 weeks, the splint is removed. Active motion and active-assisted range of motion (ROM) exercises are initiated under the guidance of a specialized hand therapist.
- Orthotic Support: A custom-molded, removable thermoplastic thumb spica splint is fabricated. This splint is worn between exercise sessions and strictly for 3 months during sleep to prevent attenuation of the transfer.
FLOATING THUMB (POUCE FLOTTANT)
Pathoanatomy and Clinical Presentation
The term "floating thumb" (pouce flottant) corresponds to a Blauth Type IV congenital thumb hypoplasia. It refers to a small, slender, severely hypoplastic thumb that appears to dangle uselessly from the radial border of the hand.
Anatomical characteristics include:
* Presence of two hypoplastic phalanges and a fingernail.
* Complete absence of the metacarpophalangeal (MCP) joint.
* Complete absence of the first metacarpal.
* The trapezium and scaphoid are also frequently absent or severely dysplastic.
* The thumb originates much more distally than a normal thumb, often attached only by a narrow skin pedicle containing a rudimentary neurovascular supply.
* There is an absolute absence of both extrinsic and intrinsic muscle function.
Treatment Strategy: Amputation and Pollicization
The definitive treatment for a Blauth Type IV floating thumb is amputation of the vestigial digit, followed by index finger pollicization.
Despite valiant historical attempts by surgeons to restore stability and function to these severely deficient and useless thumbs (using non-vascularized bone grafts, complex microvascular joint transfers, and multiple tendon transfers), the results have universally not been rewarding. Reconstructed floating thumbs remain stiff, insensate, and functionally inferior, often getting in the way of the patient's adaptive side-to-side pinch between the index and long fingers.
💡 Clinical Pearl: Parental Counseling
Recommending amputation of a child's digit is highly distressing for parents. The surgeon must clearly articulate that the "floating thumb" lacks the foundational skeletal and neuromuscular architecture required for function. Index pollicization does not merely remove a useless appendage; it fundamentally reorganizes the hand to provide a highly functional, sensate, and mobile thumb, dramatically improving the child's lifelong grip and pinch kinematics.
SEVERE WEB SPACE CONTRACTURE AND STAGED RECONSTRUCTION
In cases of severe thumb hypoplasia (such as Blauth Type II or III) where the thumb is salvageable, a profound adduction contracture of the first web space is frequently present. This contracture is driven by fascial tightness, a deficient skin envelope, and an unopposed adductor pollicis.
Addressing this contracture is paramount; an opponensplasty will fail if the thumb cannot be passively brought into full palmar abduction. For severe web space contractures, Bayne recommended a meticulous staged procedure.
Stage 1: Web Space Release and Stabilization
The initial surgery focuses entirely on releasing the contracture and expanding the skin envelope.
* Soft Tissue Release: The web space is released using a combination of Z-plasties, four-flap Z-plasties, or dorsal rotational advancement flaps. Deep fascial bands and, if necessary, the origin of the adductor pollicis or the first dorsal interosseous muscle are released.
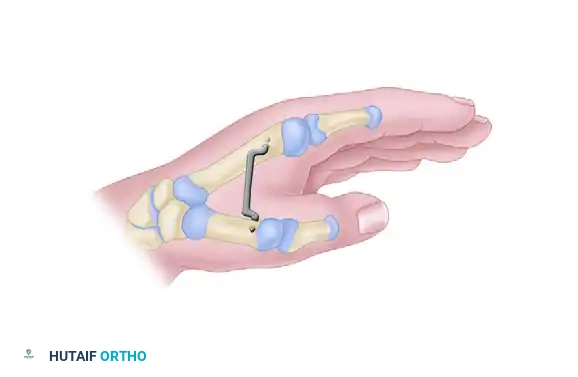
* Skeletal Stabilization: Once the thumb is mobilized into full abduction and pronation, the position is rigidly maintained with a stout Kirschner wire (K-wire) driven transversely from the first metacarpal into the second metacarpal.
Fig. 79-70: Staged reconstruction for an abducted thumb in which the severe adduction contracture is released and rigidly maintained with an interposed Kirschner wire. This skeletal stabilization is critical to allow the soft tissue envelope to heal without recurrent contracture.
Stage 2: Tendon Transfer and Ligament Reconstruction
Approximately 6 weeks following the initial release, after the soft tissues have healed and the web space is stable, the second stage is performed. The K-wire is removed, and functional reconstruction commences.
- Riordan Opponensplasty: Bayne advocated for the use of the ring finger flexor digitorum superficialis (FDS) tendon. The FDS is harvested, routed around the FCU (acting as a pulley), and tunneled subcutaneously to the thumb to restore opposition.
- Ulnar Collateral Ligament (UCL) Reconstruction: Because MCP joint instability is a hallmark of these hypoplastic thumbs, the UCL must be reconstructed to provide a stable post for pinch. This is often achieved by utilizing one slip of the transferred sublimis (FDS) tendon, routing it through the metacarpal head and proximal phalanx to recreate the ligamentous restraint.
Alternative Techniques: Flexor Pollicis Longus (FPL) Centralization
In certain hypoplastic thumbs, the FPL tendon is present but inserts abnormally, contributing to a deforming force rather than useful flexion. An alternative reconstructive technique involves:
1. Releasing the FPL from its abnormal, eccentric tendinous insertion.
2. Centralizing the tendon by moving it ulnarward.
3. To complete the transfer and correct the vector, the abductor pollicis brevis musculotendinous junction is divided.
4. The FPL tendon is transferred under the intrinsic muscle.
5. The intrinsic muscle is then reattached over the centralized FPL.
Proponents of this specific FPL centralization technique noted that, in their series, they did not find it necessary to formally reconstruct the ulnar collateral ligament, as the realigned FPL provided sufficient dynamic stability to the MCP joint. However, careful intraoperative assessment of MCP joint laxity remains mandatory.
📚 Medical References
- opponensplasty, J Bone Joint Surg 55A:725, 1973.
- Camitz H: Über die behandlung der oppositionslähmung, Acta Chir Scand 65:77, 1929.
- Carroll RE, Kleinman WB: Pectoralis major transplantation to restore elbow fl exion to the paralytic limb, J Hand Surg 4:501, 1979.
- Chuinard RG, Boyes JH, Stark HH, et al: Tendon transfers for radial nerve palsy: use of superfi cialis tendons for digital extension, J Hand Surg 3A:560, 1978.
- Chuinard RG, Dabezies EJ: Radial nerve palsy, JCE Orthop 16:26, 1978.
- Curtis RM: Fundamental principles of tendon transfer, Orthop Clin North Am 2:231, 1974.
- DeBenedetti M: Restoration of elbow extension power in the tetraplegic patient using the Moberg technique, J Hand Surg 4:86, 1979.
- Ejeskär A: Upper limb surgical rehabilitation in high-level tetraplegia, Hand Clin 4:585, 1988.
- Familla JM, Peimer CA, Sherwin FS: Brachioradialis transfer for digital palsy, J Hand Surg 15B:312, 1990.
- Fischer T, Nagy L, Buechler U: Restoration of pinch grip in ulnar nerve palsies: Extensor carpi radialis longus to adductor pollicis and abductor pollicis longus to fi rst dorsal interosseous tendon transfers, J Hand Surg 28B:28, 2003.
- Foster RJ, Swiontkowski MF, Bach AW, et al: Radial nerve palsy caused by open
You Might Also Like