Masterclass in Total Wrist Arthrodesis: Principles, Biomechanics, and Surgical Techniques
Key Takeaway
Total wrist arthrodesis remains a cornerstone procedure for end-stage radiocarpal and intercarpal joint pathology. This comprehensive guide details the evolution of rigid internal fixation, precise patient positioning, and step-by-step surgical techniques, including the AO dorsal plating method and the Haddad-Riordan lateral approach. Mastery of these techniques ensures stable fusion, pain relief, and maximal functional grip strength for patients with posttraumatic arthritis, rheumatoid disease, or paralytic deformities.
Introduction and Historical Evolution
Despite the modern trend toward motion-preserving reconstructive surgery and total joint arthroplasty, total wrist arthrodesis remains an indispensable procedure in the armamentarium of the orthopaedic hand and upper extremity surgeon. It is the gold standard salvage procedure for end-stage pancarpal arthritis, providing predictable pain relief and a stable platform for maximal hand function.
The surgical approach to arthrodesis of the radiocarpal and intercarpal joints has evolved significantly over the last half-century, primarily driven by advancements in the biomechanics of internal fixation. Early historical procedures relied heavily on cortical or cancellous bone grafting combined with limited, non-rigid fixation methods such as Kirschner wires, Steinmann pins, or staples. In 1964, Campbell and Keokarn described an inlay bone grafting technique, which was later modified by Haddad and Riordan to be applied through a lateral (radial) approach.
While pin and staple fixation are still occasionally employed—particularly in patients with severe rheumatoid arthritis and poor bone stock—the definitive modern trend has shifted toward rigid plate osteosynthesis. Interestingly, a study by Rehak et al. comparing pin versus plate fixation in 57 rheumatoid arthritis patients found no statistically significant difference in successful fusion rates between the two groups. However, the paradigm shifted permanently in 1970 when the Arbeitsgemeinschaft für Osteosynthesefragen (AO) group introduced a rigid fixation method utilizing a dynamic compression plate (DCP).
Mechanical testing studies have unequivocally proven that dorsal plate fixation provides the most stable biomechanical construct. Today, it is the most favored and commonly utilized technique for wrist arthrodesis. The advantages of the dynamic compression plate are multifold: it yields excellent fusion rates, drastically decreases the incidence of postoperative malposition, and provides sufficient rigidity to allow for early rehabilitation. Furthermore, the AO plating technique requires less structural bone grafting than historical methods; often, an adequate volume of cancellous autograft can be harvested locally from the distal radius metaphysis and the excised carpal bones. Anderson and Thomas even reported a series of 15 patients who achieved successful wrist fusion by 12 weeks using dynamic compression plates without the addition of any supplemental bone graft. Nevertheless, the current academic consensus recommends utilizing iliac crest bone graft if the local cancellous yield from the distal radius is insufficient.
Indications and Contraindications
The decision to proceed with a total wrist arthrodesis must be carefully weighed against motion-preserving alternatives (e.g., proximal row carpectomy, four-corner fusion, or total wrist arthroplasty).
Primary Indications
Posttraumatic arthritis with painful, irreversible destruction of the radiocarpal and midcarpal joints is the most common indication, particularly in the dominant extremity of a young, high-demand manual laborer.
Clinical Pearl: Some authors advocate for immediate primary wrist fusion in the setting of severely comminuted, irreparable intraarticular fractures of the distal radius where anatomic articular restoration is impossible.
Other established indications include:
* Neoplastic Lesions: Joint destruction secondary to aggressive benign or malignant tumor resection.
* Infection: Post-infectious articular destruction (following eradication of the pathogen).
* Kienböck Disease: End-stage (Lichtman Stage IV) with secondary pancarpal arthrosis.
* Rheumatoid Arthritis: Severe carpal collapse, ulnar translocation, and radiocarpal destruction.
* Neurologic Deficits: Stabilization of a paralytic wrist and hand (e.g., brachial plexus injury) to provide a stable post for tendon transfers.
* Spastic Hemiplegia: Correction of severe, fixed wrist flexion deformities to improve hygiene and function.
* Salvage Procedures: Failed total wrist arthroplasty or failed previous limited intercarpal arthrodesis.
Contraindications
The primary absolute contraindication is an open physis of the distal radius. The distal radial physis contributes approximately 75% of the longitudinal growth of the radius and does not close until approximately 17 years of age. Extreme care must be taken to avoid iatrogenic physeal arrest in pediatric patients.
Surgical Warning: Fusion of the wrist in children is notoriously difficult to secure due to the vast preponderance of unossified cartilage in the carpus. If absolutely necessary, the procedure should be postponed until the patient is at least 10 to 12 years of age. If partial physeal destruction has already occurred due to trauma or disease, the remaining physis may be intentionally excised to prevent asymmetric growth and progressive deformity.
A relative contraindication is an elderly patient with a low-demand, sedentary lifestyle, particularly if the non-dominant wrist is affected. In such cases (often seen in rheumatoid populations), total wrist arthroplasty or targeted tendon transfers may provide a superior quality of life by preserving motion.
Biomechanics and Optimal Positioning
The functional success of a wrist arthrodesis is entirely dependent on the intraoperative positioning of the fusion. The wrist must be fused in a position that minimizes fatigue of the extrinsic musculature while maximizing the grasping strength of the hand.
The Standard Position:
The universally accepted optimal position is 10 to 20 degrees of extension (dorsiflexion), with the long axis of the third metacarpal shaft perfectly aligned with the long axis of the radial shaft. Clinically, this mimics the natural tenodesis position the wrist assumes when a fist is strongly clenched.
Coronal Plane Alignment:
In the coronal plane, neutral to 5 degrees of ulnar deviation is preferred. This slight ulnar deviation optimizes the line of pull for the extrinsic flexors and compensates for the loss of the dart-thrower's motion arc.
Alternative Positions:
* Neutral Position: Several authors advocate for a strictly neutral sagittal position (0 degrees of extension). This allows for full forearm pronation and supination, facilitates personal hygiene (especially perineal care), and still provides sufficient grip strength.
* Slight Palmar Flexion: A minority of surgeons favor slight palmar flexion (up to 25 degrees), though this significantly weakens grip strength and is generally reserved for specific anatomic or neurologic constraints.
* Bilateral Fusions: If bilateral wrist fusions are required, the positions must be tailored to the patient's specific activities of daily living (ADLs). Generally, fusing both wrists in a neutral position is thought to provide the maximal combined functional envelope.
Preoperative Planning and Graft Selection
While modern plating techniques have reduced the reliance on massive structural grafts, biologic augmentation remains critical. The iliac crest is the gold standard donor site for cancellous autograft. However, graft material may also be harvested from the distal radius (Lister's tubercle and the metaphysis), ulna, proximal tibia, or rib.
Sorial et al. reported a highly successful series of 18 patients utilizing a local radial sliding graft fixed with a DCP. Depending on the defect, the graft can bridge from the radius to the proximal carpal row, or extend distally to the base of the third metacarpal.
The Carpometacarpal (CMC) Joint Debate
A critical decision in preoperative planning is whether to include the second and third carpometacarpal joints in the fusion mass.
* Proponents of Inclusion: Haddad and Riordan recommended that the 2nd and 3rd CMC joints always be included. They argued that the altered biomechanical lever arm of a fused wrist places immense stress on these joints, leading to late-onset arthritis and painful micro-motion. Furthermore, inflammatory diseases (like RA) frequently extend into these joints.
* Proponents of Exclusion: Conversely, preserving the CMC joints maintains a small degree of compensatory motion. Nagy and Büchler reported on 81 wrist arthrodeses, 47 of which included the 3rd CMC joint. Shockingly, 43% (20 patients) developed a painful nonunion at the CMC joint, and 23% required revision surgery. In stark contrast, only 1 of the 34 patients in whom the 3rd CMC joint was spared developed postoperative pain at that site. Therefore, unless the CMC joints are frankly arthritic, modern consensus leans toward sparing them.
Surgical Approaches and Techniques
The AO Dorsal Plating Technique (Technique 4-13)
The AO technique, heavily championed by Heim, Pfeiffer, Wright, and McMurtry, provides unparalleled internal fixation, effectively eliminating the need for prolonged postoperative cast immobilization.
Implant Selection:
The AO Hand Study Group designed specific titanium low-profile dynamic compression plates (Synthes) for this procedure.
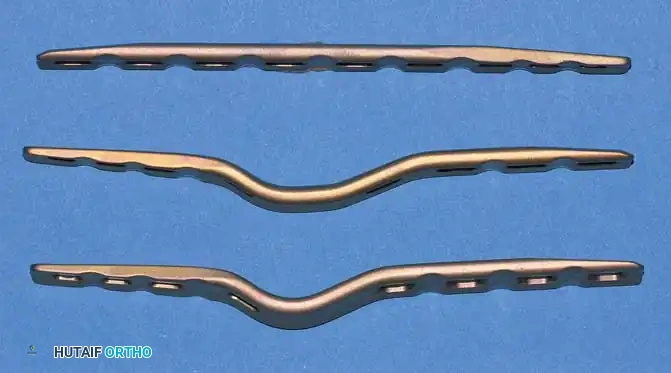
Fig. 4-19: Three types of AO wrist arthrodesis plates: straight plate, long carpal bend, and short carpal bend. All utilize three 2.7-mm metacarpal screws, one 2.7-mm capitate screw, and four 3.5-mm radius screws.
- Straight Plate: Employed when a large intercalary structural graft is required (e.g., post-tumor resection or massive traumatic bone loss).
- Short Carpal Bend: Utilized in smaller wrists or when the proximal carpal row has been previously resected (e.g., Proximal Row Carpectomy).
- Long Carpal Bend: The standard choice for large wrists with intact carpal rows.
These plates feature tapered edges and recessed screw holes to minimize dorsal soft-tissue irritation. Despite this low-profile design, the lack of dorsal subcutaneous fat means hardware removal is still required in approximately 15% of cases due to symptomatic prominence. Biomechanical studies by Morelli et al. confirmed that while DCP fixation is vastly superior to Steinmann pins, there is no significant biomechanical difference in stability between a standard 3.5-mm DCP and the precontoured low-profile plates. If a standard 3.5-mm reconstruction or DCP is used, it must be meticulously contoured intraoperatively to match the dorsal wrist anatomy.
Step-by-Step Surgical Procedure
- Incision and Exposure: Make a longitudinal, curvilinear skin incision beginning 2 cm proximal to the distal radioulnar joint (DRUJ), extending ulnarly, and terminating over the midshaft of the third metacarpal.
- Nerve Protection: Meticulously identify, mobilize, and protect the dorsal sensory branches of the superficial radial nerve and the dorsal branch of the ulnar nerve.
- Extensor Retinaculum: Make a longitudinal incision through the extensor retinaculum between the tendons of the extensor digitorum communis (EDC) and the extensor pollicis longus (EPL). Retract the EDC ulnarly and the EPL radially.
- Capsulotomy: Perform an I-shaped or T-shaped incision in the dorsal radiocarpal capsule, exposing the radiocarpal and midcarpal joints down to the carpometacarpal joints.
- Bone Preparation: Using a sharp osteotome or rongeur, excise Lister’s tubercle. Remove the dorsal cortices of the scaphoid, lunate, capitate, and the base of the third metacarpal to create a flat, bleeding cancellous bed that allows flush apposition of the precontoured plate.
- Cartilage Denudation: Systematically denude all articular cartilage from the radiocarpal and intercarpal joints down to bleeding subchondral bone. Fill all resulting gaps with cancellous bone graft harvested from the excised dorsal cortices and the distal radial metaphysis.
- Provisional Fixation: A 3.5-mm cortical lag screw may be placed from the radial styloid obliquely into the capitate. This pulls the carpus tightly against the radius and helps prevent ulnar translation and impingement of the DRUJ.
- Plate Application: Apply the selected precontoured plate to the dorsal aspect of the third metacarpal. Crucial Step: Ensure the distal end of the plate is perfectly centered on the diaphysis of the third metacarpal to prevent eccentric loading or cortical blowout.

Fig. 4-20: Dorsal view of wrist fusion with AO wrist fusion plate (low-contact dynamic compression plate).
- Distal Fixation: Mark the position of the most distal hole. Remove the plate, drill a 2.0-mm hole in a dorsal-to-volar direction (centered in the metacarpal), tap, and insert a 2.7-mm cortical screw.
- Compression: Fill the remaining metacarpal holes with 2.7-mm screws. Next, apply axial compression across the radiocarpal and intercarpal joints by placing a 3.5-mm screw in the compression mode (eccentric drilling) through the second-most distal hole in the radius.
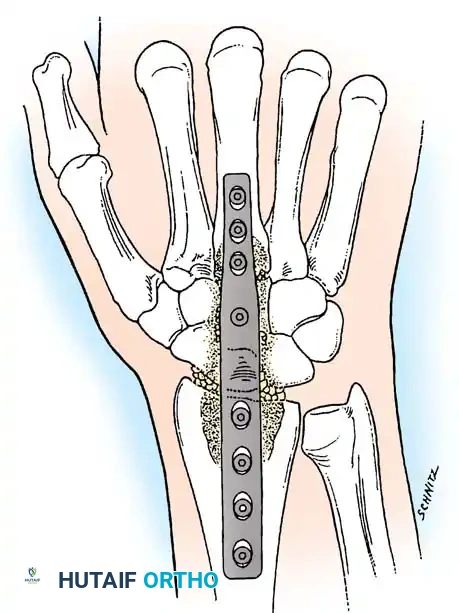
Fig. 4-21: Lateral radiographic view of wrist fusion with AO plate, demonstrating excellent contouring and hardware placement.
- Final Fixation and Closure: Fill the remaining radial holes with 3.5-mm screws. Insert the dedicated capitate screw if the plate design allows. Thoroughly irrigate the wound, place a small closed-suction drain, and meticulously close the extensor retinaculum (often leaving the EPL transposed subcutaneously to prevent attrition rupture) and skin.
Postoperative Protocol (AO Technique):
A bulky, well-padded short-arm splint is applied in the operating room. At 10 to 14 days, sutures are removed, and the patient is transitioned to a short-arm cast or a removable thermoplastic splint, depending on bone quality and fixation rigidity. Because of the rigid plate fixation, early digital range of motion is encouraged immediately to prevent tendon adhesions. Clinical and radiographic fusion is typically solid by 10 to 12 weeks.
Wrist Arthrodesis with Proximal Row Carpectomy (Technique 4-14)
In cases of severe proximal carpal row necrosis (e.g., advanced Kienböck disease) or when converting a failed proximal row carpectomy (PRC) to a fusion, a radiocapitate fusion is indicated. Louis et al. described a highly successful technique combining PRC with radiocapitate arthrodesis.
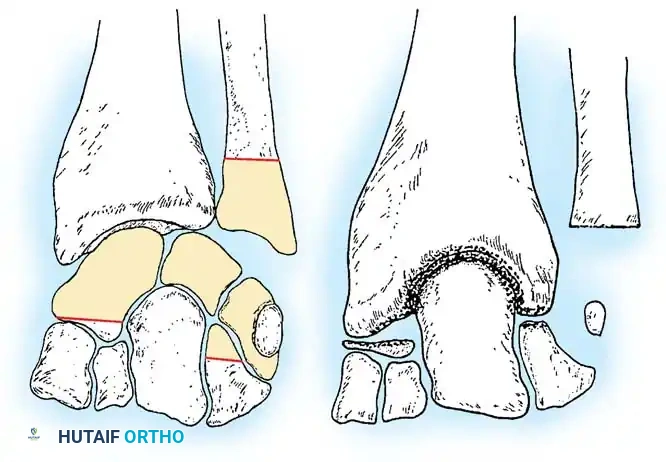
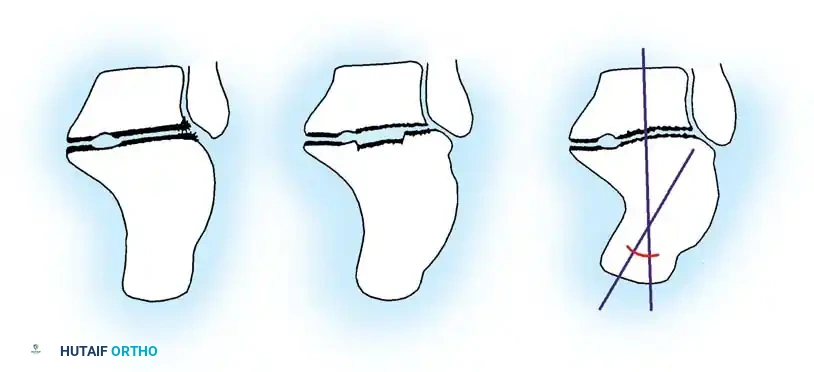
Fig. 4-22: (A) Schematic diagram depicting the bone to be resected to accomplish capitate-radius arthrodesis. (B) Postoperative schematic. The proximal pole of the capitate and the distal surface of the radius have been denuded of cartilage. A portal is established in the distal radius, and the congruous trabecular surfaces are apposed.
Step-by-Step Surgical Procedure
- Approach the wrist dorsally as described in Technique 4-13.
- Perform a proximal row carpectomy: Excise the entire lunate and triquetrum. Remove approximately 80% of the proximal scaphoid and a portion of the proximal hamate.
> Clinical Pearl: It is vital to retain the distal portion of the scaphoid and hamate to maintain the structural integrity of the distal carpal row and prevent proximal migration or destabilization of the remaining carpus. - Aggressively denude the articular cartilage from the lunate fossa of the distal radius and the proximal pole of the capitate.
- Appose the capitate directly into the prepared fossa of the distal radius.
- Fixation can be achieved with a short-bend AO dorsal plate, or alternatively, with crossed Kirschner wires/staples supplemented with abundant cancellous bone graft.
Postoperative Protocol:
If rigid plate fixation is not used, the wrist must be strictly immobilized in a long-arm or short-arm cast for 12 to 16 weeks until trabecular bridging is radiographically confirmed.
Cortical Strut Autograft: The Haddad and Riordan Lateral Approach (Technique 4-15)
Haddad and Riordan pioneered a lateral (radial) approach utilizing a cortical strut graft. They theorized that the traditional dorsal approach leads to excessive scar tissue formation, restricting extensor tendon gliding. The lateral approach offers distinct advantages: it completely avoids the distal radioulnar joint, minimizes disturbance to the digital extensor tendons, and preserves the dorsal contour of the wrist. Carlson and Simmons later reported excellent results using this technique with bulk fresh-frozen femoral head allograft to salvage failed wrist arthroplasties.
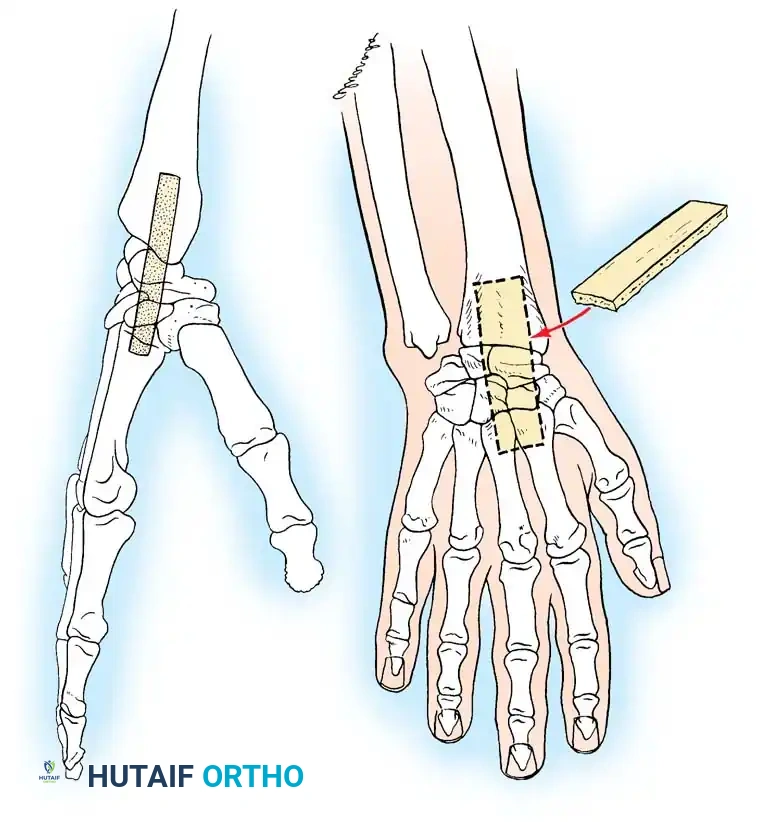
Fig. 4-23: Haddad and Riordan arthrodesis of the wrist. (A) Radial view showing the slot cut into the distal radius, carpal bones, and the bases of the second and third metacarpals. (B) Dorsal view showing the shape of the graft and its final position (broken line) within the slot.
Step-by-Step Surgical Procedure
- Incision: Make a J-shaped skin incision beginning 2.5 to 4 cm proximal to the radial styloid on the midlateral aspect of the forearm. Extend it distally across the styloid, curving dorsally to terminate at the base of the second metacarpal.
- Nerve Mobilization: Carefully identify, mobilize, and retract the superficial branch of the radial nerve (usually in a palmar direction).
- Compartment Release: Identify the interval between the first dorsal compartment (APL, EPB) and the second dorsal compartment (ECRL, ECRB). Incise the dorsal carpal ligament in this interval, leaving it attached to the volar aspect of the radius.
- Subperiosteal Dissection: Subperiosteally elevate and retract the abductor pollicis longus, extensor pollicis brevis, and the wrist/finger extensors to expose the radial aspect of the radiocarpal joint.
- Tendon Management: Divide the extensor carpi radialis longus (ECRL) tendon just proximal to its insertion at the base of the second metacarpal. Leave a sufficient distal stump to allow for robust repair during closure.
- Capsulectomy: Excise the capsule overlying the radiocarpal, intercarpal, and second carpometacarpal joints.
- Vascular Control: Identify the dorsal branch of the radial artery. Ligate and divide it to allow full access to the radial column.
- Slot Preparation: Using an oscillating saw and osteotomes, create a precise, continuous longitudinal slot through the radial styloid, across the scaphoid and trapezoid, and into the base of the second (and optionally third) metacarpal.
- Graft Harvesting and Insertion: Harvest a matching cortical strut graft (typically from the inner table of the iliac crest or proximal tibia). Impact the graft firmly into the prepared slot. The graft acts as both a biologic osteogenic scaffold and a mechanical strut.
- Fixation: Supplement the strut graft with crossed Steinmann pins or screws to provide rotational stability. Repair the ECRL tendon and close the wound in layers.
Complications and Salvage Strategies
While total wrist arthrodesis is highly successful, complications can occur:
* Nonunion (Pseudarthrosis): Occurs in 2-5% of cases, most commonly at the carpometacarpal junction (especially the 3rd CMC if included). Treatment requires revision bone grafting and rigid plate fixation.
* Hardware Prominence: The most frequent complication (up to 15%), necessitating plate removal once fusion is solid (typically after 12-18 months).
* Extensor Tendon Irritation/Rupture: Often involves the EPL or EDC due to friction against the dorsal plate. Prevented by meticulous retinacular closure or prophylactic EPL transposition.
* DRUJ Impingement: Caused by ulnar translation of the carpus or over-compression. May require subsequent Darrach procedure or Sauvé-Kapandji procedure if symptomatic.
Conclusion
Total wrist arthrodesis is a highly durable, definitive solution for the painful, arthritic wrist. Mastery of the biomechanical principles of positioning, combined with meticulous execution of rigid AO dorsal plating or specialized lateral grafting techniques, ensures a high rate of successful osteosynthesis. By providing a stable, pain-free radiocarpal pillar, surgeons can reliably restore powerful grip strength and significantly improve the patient's overall quality of life.
You Might Also Like