Advanced Management of Hamate Fractures and Complex Carpal Dynamics
Key Takeaway
Fractures of the hamate, particularly involving the hamulus, present unique diagnostic and therapeutic challenges. This comprehensive guide details the biomechanics, advanced imaging techniques, and surgical management of hamate fractures, alongside complex carpal kinematics. Furthermore, it explores concomitant carpal injuries, including the step-by-step surgical technique for pedicled vascularized bone grafting in scaphoid nonunions, providing orthopedic surgeons with evidence-based protocols for optimal patient outcomes.
INTRODUCTION TO CARPAL TRAUMA AND KINEMATICS
The human carpus is a highly complex biomechanical structure, relying on precise osseous geometry and intricate ligamentous constraints to facilitate fluid motion and load transfer between the hand and the forearm. Among carpal injuries, fractures of the hamate represent a unique subset of trauma that demands a high index of suspicion, advanced diagnostic imaging, and meticulous surgical execution. While hamate fractures are relatively uncommon, missed diagnoses can lead to profound morbidity, including chronic pain, flexor tendon rupture, and ulnar neuropathy.
Furthermore, carpal trauma rarely occurs in isolation. High-energy axial loads, typically sustained during a fall on an outstretched hand (FOOSH), initiate a predictable cascade of intercarpal kinematics that can result in complex fracture-dislocations, such as scaphoid fractures and capitate inversions. When scaphoid fractures progress to nonunion, advanced reconstructive techniques, including pedicled vascularized bone grafting, become necessary. This masterclass provides an exhaustive, evidence-based review of hamate fractures, complex carpal kinematics, and advanced surgical interventions for carpal nonunions.
FRACTURES OF THE HAMATE
Fractures of the hamate can be broadly classified based on their anatomical location: the hamulus (hook), the body, and the various articular surfaces. Each subtype presents distinct biomechanical challenges and requires tailored management strategies.
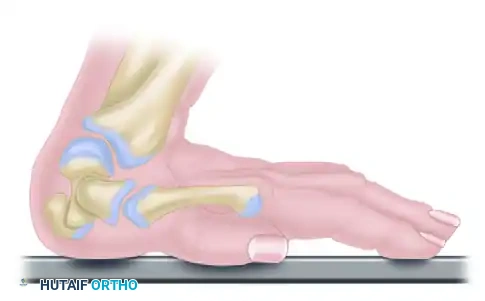
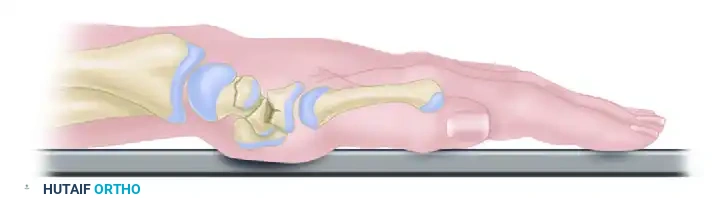
Anatomical Considerations and Biomechanics
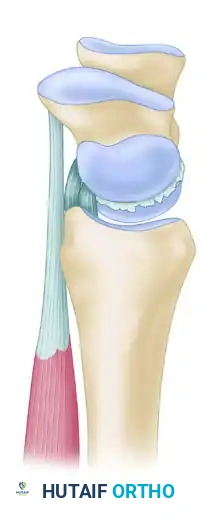
The hamate articulates distally with the fourth and fifth metacarpals, proximally with the triquetrum, and radially with the capitate. The most clinically significant feature of the hamate is its volar projection, the hamulus or "hook."
The hook of the hamate serves several critical biomechanical functions:
* Pulley Mechanism: It acts as a mechanical pulley for the flexor digitorum profundus (FDP) tendons to the ring and small fingers.
* Ligamentous Attachment: It serves as the ulnar attachment site for the transverse carpal ligament (flexor retinaculum) and the pisohamate ligament.
* Neurovascular Proximity: It forms the radial border of Guyon’s canal, intimately associating with the ulnar nerve (specifically the deep motor branch) and the ulnar artery.
Surgical Warning: The deep motor branch of the ulnar nerve curves sharply around the distal aspect of the hook of the hamate. Any surgical approach or aggressive retraction in this area carries a high risk of iatrogenic motor palsy.
Clinical Presentation and Mechanism of Injury
Fractures of the hook of the hamate are frequently seen in athletes who participate in racquet sports, golf, or baseball. The mechanism typically involves a direct axial blow from the handle of a club, bat, or racquet against the hypothenar eminence during a forceful swing. Alternatively, stress fractures may develop from repetitive microtrauma.
Patients typically present with:
* Vague, deep-seated pain in the hypothenar eminence or the "heel" of the hand.
* Exacerbation of pain with a firm grasp or swinging motion.
* Point tenderness directly over the bony prominence just lateral and slightly distal to the pisiform.
* Occasional transient ulnar nerve motor palsy due to hematoma, edema, or direct osseous compression.
Clinical Pearl: To isolate pain originating from the hook of the hamate, perform the "pull test." With the patient's wrist in ulnar deviation, ask them to actively flex the distal interphalangeal joints of the ring and small fingers against resistance. This engages the FDP tendons against the hamulus, eliciting sharp pain if a fracture is present.
Diagnostic Imaging Protocols
A fracture of the hook of the hamate is notoriously difficult to visualize on standard posteroanterior (PA) and lateral radiographs of the wrist due to osseous overlap.
- Carpal Tunnel View: This specialized radiographic view is essential. It profiles the volar projections of the carpus, including the hook of the hamate and the ridge of the trapezium. However, patient positioning (extreme wrist dorsiflexion) may be limited by acute pain.
- Computed Tomography (CT): High-resolution CT is the gold standard for diagnosing hamate fractures. Axial and sagittal reconstructions provide definitive visualization of fracture displacement and comminution.
When utilizing CT, placing the patient’s hands together in the "praying position" within the gantry is highly recommended. This technique captures both wrists simultaneously, allowing the surgeon to rule out a congenital variation known as os hamuli proprium (a bipartite hamate), which is usually bilateral and features smooth, corticated margins unlike an acute fracture.
Management Strategies
Treatment algorithms are dictated by the anatomical location and the degree of displacement.
1. Fractures of the Body:
Fractures of the body of the hamate are usually stable due to robust intercarpal ligamentous support. They are typically treated conservatively with cast immobilization for 4 to 6 weeks. Surgery is rarely required unless there is significant displacement or associated carpometacarpal fracture-dislocations.
2. Articular Fractures:
Articular fractures, particularly those involving the fourth and fifth carpometacarpal joints, demand anatomical restoration. Open reduction and internal fixation (ORIF) using mini-fragment screws or Kirschner wires (K-wires) is strictly indicated if the displacement or articular step-off is 1 mm or greater.
3. Fractures of the Hook (Hamulus):
* Acute, Non-displaced: Can be trialed with short-arm cast immobilization (including the 4th and 5th digits to neutralize FDP forces) for 6 weeks. However, nonunion rates remain high due to poor vascularity at the base of the hook.
* Acute, Displaced: ORIF with a headless compression screw can be attempted in high-demand athletes to preserve anatomy, though technically demanding.
* Nonunion or Delayed Presentation: Excision of the hook fragment is the gold standard. It yields excellent functional outcomes, rapid return to sport, and eliminates the risk of secondary flexor tendon rupture.
Surgical Technique: Excision of the Hook of the Hamate
Positioning and Preparation:
The patient is placed supine with the arm extended on a hand table. A well-padded proximal tourniquet is applied. Regional or general anesthesia is utilized.
Surgical Approach:
1. Incision: A longitudinal incision is made over the hypothenar eminence, in line with the fourth ray, curving slightly ulnarly as it approaches the distal wrist crease to avoid crossing flexion creases perpendicularly.
2. Superficial Dissection: The subcutaneous tissue is divided, taking care to identify and protect the palmar cutaneous branches of the ulnar nerve.
3. Guyon's Canal Release: The volar carpal ligament is incised to decompress Guyon's canal. The ulnar artery and nerve are identified. The superficial sensory branch and the deep motor branch of the ulnar nerve are meticulously traced.
4. Isolating the Hook: The deep motor branch of the ulnar nerve is gently retracted ulnarly. The transverse carpal ligament is incised along its ulnar border, leaving a small cuff for later repair if necessary.
5. Subperiosteal Dissection: The nonunion site or fracture line is identified. Using a small periosteal elevator or scalpel, the soft tissue attachments (pisohamate ligament, flexor digiti minimi) are sharply dissected off the hook fragment.
6. Excision: The fragment is grasped with a towel clip or rongeur and excised.
7. Base Preparation: The remaining base of the hamate must be aggressively rasped or burred smooth until it is flush with the body of the hamate. Any residual prominence can fray the adjacent FDP tendons, leading to delayed rupture.
8. Closure: The tourniquet is deflated to ensure meticulous hemostasis. The skin is closed with non-absorbable sutures. The transverse carpal ligament is generally left open to prevent postoperative compartment syndrome of the carpal tunnel.
COMPLEX CARPAL KINEMATICS AND CONCOMITANT INJURIES
Understanding the mechanism of carpal fractures is paramount, as the forces that fracture the hamate or scaphoid often propagate through the carpus, creating complex instability patterns. The most common mechanism is a fall on an outstretched hand (FOOSH) with the wrist forced into marked dorsiflexion, ulnar deviation, and intercarpal supination.
The Mechanism of Carpal Fractures (Naviculocapitate Syndrome)
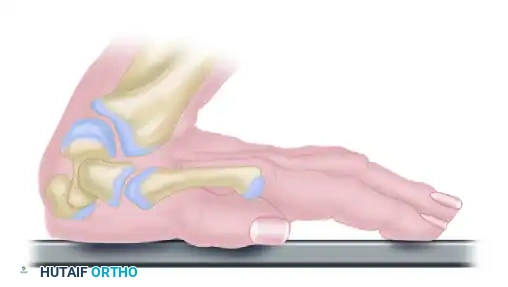
The sequence of events during an extreme dorsiflexion injury can lead to a specific pattern of scaphoid and capitate fractures, illustrating the profound forces transmitted through the midcarpal joint.
A. As the patient falls, the wrist is forced into marked dorsiflexion. The capitate, acting as the keystone of the carpus, is driven into a 90-degree angle relative to the distal radius.
B. The scaphoid, bridging the proximal and distal carpal rows, is subjected to immense bending moments. As dorsiflexion increases at the midcarpal joint, the scaphoid fractures through its waist.
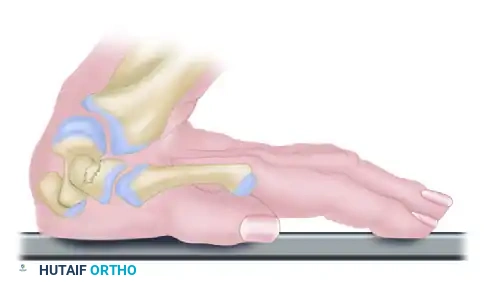
C. With continued axial loading and extreme dorsiflexion, the dorsal lip of the distal radius acts as an anvil. It strikes the neck of the capitate directly, causing a transverse fracture of the capitate.
D. The proximal fragment of the fractured capitate is now devoid of its distal structural support. The ongoing kinetic energy and ligamentous tethering cause the proximal capitate fragment to rotate 90 degrees within the midcarpal space.
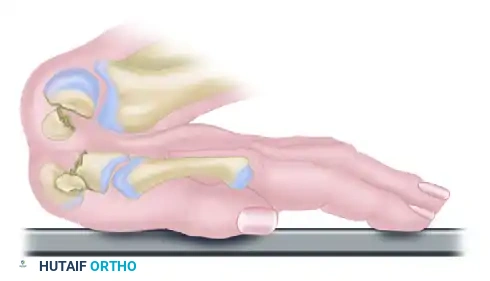
E. As the kinetic energy dissipates and the wrist returns to a neutral resting position, the proximal fragment of the capitate is forced into a complete 180-degree rotation. The articular surface of the capitate head now faces distally, creating a profound mechanical block and requiring complex open reduction.
Pitfall: Failure to recognize a rotated proximal capitate fragment on initial radiographs is a common error. Always scrutinize the lateral radiograph for the "crescent sign" of the capitate head articulating with the lunate.
ADVANCED RECONSTRUCTION: SCAPHOID NONUNION
As demonstrated in the kinematic sequence above, the scaphoid is highly susceptible to fracture during a FOOSH. Due to its tenuous retrograde blood supply—entering distally and flowing proximally—fractures of the scaphoid waist or proximal pole have a notoriously high rate of nonunion and avascular necrosis (AVN).
When conservative management or standard ORIF fails, or when AVN is present, structural and biological augmentation is required. The pedicled vascularized bone graft utilizing the 1,2 intercompartmental supraretinacular artery (ICSRA) has become a cornerstone technique for salvaging scaphoid nonunions.
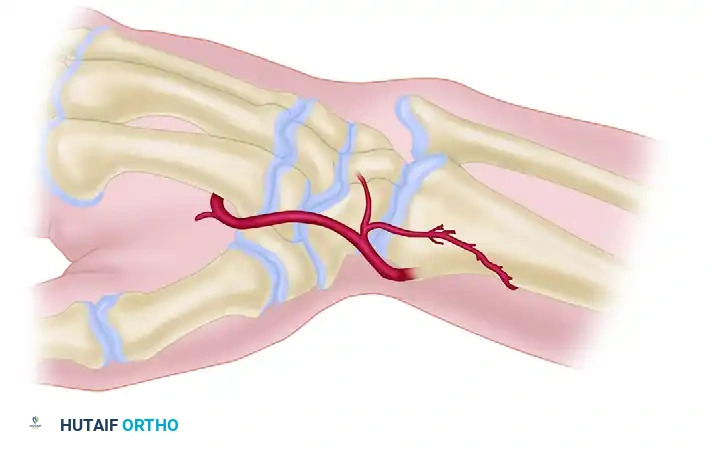
Pedicled Vascularized Bone Grafting (1,2 ICSRA)
The 1,2 ICSRA is a consistent branch of the radial artery that runs longitudinally on the dorsal aspect of the distal radius, precisely between the first extensor compartment (abductor pollicis longus and extensor pollicis brevis) and the second extensor compartment (extensor carpi radialis longus and brevis).
Indications:
* Scaphoid waist or proximal pole nonunions.
* Presence of avascular necrosis of the proximal pole (evidenced by punctate bleeding absence intraoperatively or MRI findings).
* Failed previous non-vascularized bone grafting.
Step-by-Step Surgical Approach
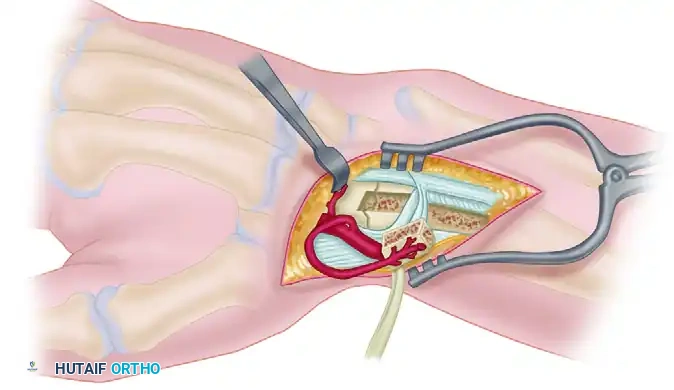
A. Exposure and Vessel Identification:
A curvilinear dorsal incision is made over the radiocarpal joint, extending proximally over the distal radius. The subcutaneous tissues are carefully raised from the extensor retinaculum. The 1,2 intercompartmental supraretinacular artery (ICSRA) is visualized running within the retinacular tissue between the first and second compartments.
B. Nerve Protection and Compartment Release:
Meticulous dissection is required to identify and protect the branches (I, II, III) of the superficial branch of the radial nerve (SBRN). Retraction of these branches must be gentle to prevent postoperative neuropathic pain. Dashed lines indicate the precise incisions made along the borders of the first and second extensor compartments to isolate the vascular pedicle along with a cuff of retinaculum.
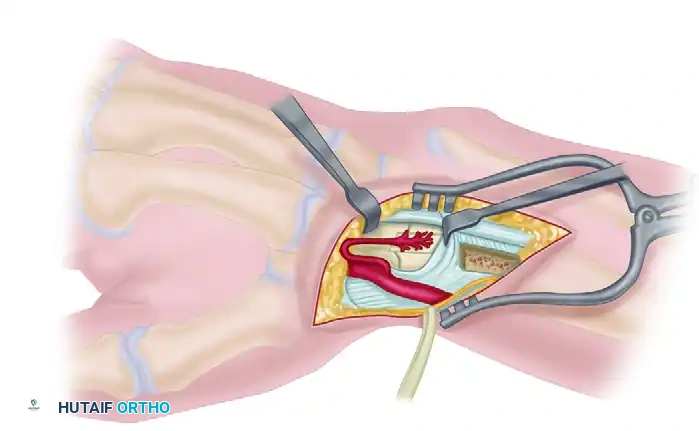
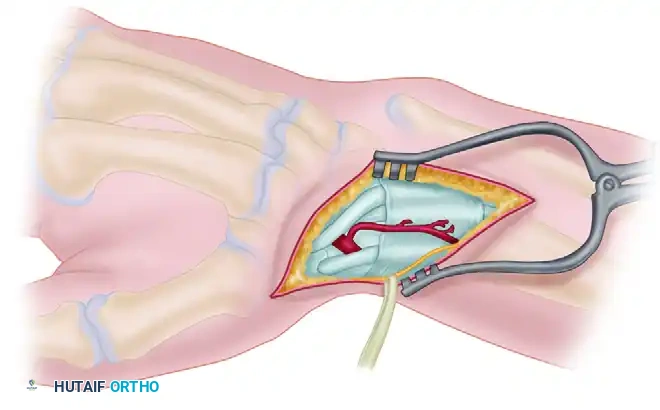
C. Graft Harvest and Vascularity Check:
Using a fine osteotome or a microsurgical burr, a cortical-cancellous block of bone is harvested from the distal radius, keeping the 1,2 ICSRA pedicle attached. With the graft levered out of the donor site, the pneumatic tourniquet is temporarily deflated. The surgeon must visually confirm active punctate bleeding from the cancellous surface of the graft, verifying its vascular integrity before transfer.
D. Graft Inset and Fixation:
The scaphoid nonunion site is thoroughly debrided of all fibrous tissue and necrotic bone until healthy, bleeding margins are achieved. The wrist is placed in ulnar deviation to open the nonunion gap. The vascularized graft is gently rotated on its pedicle and press-fit into the scaphoid trough. Supplemental rigid fixation is paramount; this is typically achieved with multiple parallel Kirschner wires or a headless compression scaphoid screw, ensuring the vascular pedicle is not compressed or kinked during hardware placement.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The success of both hamate excision and complex carpal reconstruction relies heavily on strict adherence to postoperative rehabilitation protocols.
Following Hamate Hook Excision:
* Weeks 0-2: The wrist is immobilized in a bulky soft dressing and a volar resting splint. Digital range of motion (ROM) is encouraged immediately to prevent flexor tendon adhesions.
* Weeks 2-4: Sutures are removed. The patient is transitioned to a removable custom orthosis. Gentle active wrist
You Might Also Like