Operative Management of Hamate, Trapezium, and Rare Carpal Fractures
Key Takeaway
Fractures of the hook of the hamate and adjacent carpal bones present unique diagnostic and surgical challenges. This guide details the operative techniques for excision or open reduction and internal fixation (ORIF) of the hamate hook. It also provides a comprehensive review of trapezium and trapezoid fractures, emphasizing biomechanics, surgical approaches, and postoperative protocols to optimize functional recovery and prevent late-stage arthrosis in the wrist and hand.
INTRODUCTION TO RARE CARPAL FRACTURES
While scaphoid fractures dominate the landscape of carpal trauma, fractures of the remaining carpal bones—particularly the hamate, trapezium, and trapezoid—require an equally rigorous diagnostic and therapeutic approach. These injuries often result from high-energy trauma, repetitive stress in athletes (e.g., golfers, baseball players), or complex fracture-dislocations of the wrist. Delayed diagnosis is common due to the subtle radiographic appearance of these fractures on standard posteroanterior (PA) and lateral views.
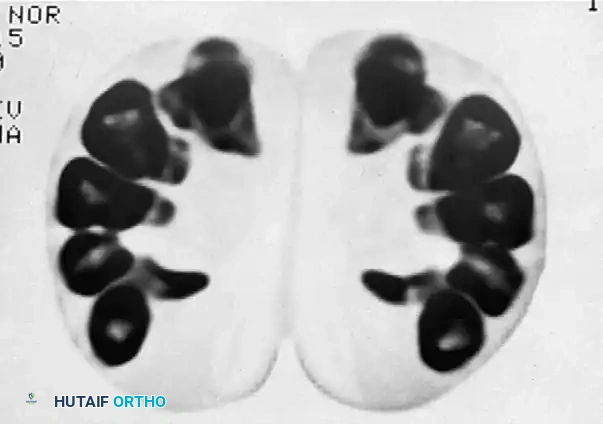
Advanced imaging, specifically computed tomography (CT) and specialized radiographic projections (such as the carpal tunnel view), is mandatory for accurate characterization. The operative management of these fractures demands a profound understanding of carpal biomechanics, the intricate ligamentous anatomy of the wrist, and the proximity of critical neurovascular structures, most notably the ulnar nerve within Guyon’s canal.
EXCISION OR REDUCTION AND FIXATION OF THE HOOK OF THE HAMATE
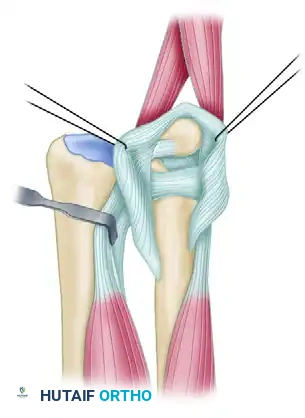
Fractures of the hook of the hamate typically occur secondary to a direct blow to the palm, often from a grounded golf club, a baseball bat, or a racquet. The hook serves as a critical pulley for the ulnar flexor tendons and an attachment site for the transverse carpal ligament and the pisohamate ligament.
Because the hook of the hamate possesses a watershed blood supply at its waist—with feeding vessels entering through the tip and the base—fractures through the waist are notoriously prone to nonunion.
🔪 Surgical Warning
A displaced or ununited fracture of the hamate hook can cause chronic irritation and eventual spontaneous rupture of the ulnar-sided flexor digitorum profundus (FDP) tendons. Furthermore, the close proximity of the deep motor branch of the ulnar nerve places it at high risk for compression or iatrogenic injury during surgical intervention.
Preoperative Imaging and Planning
Standard PA and lateral radiographs are often insufficient. A carpal tunnel view or a supinated oblique view may demonstrate the fracture, but a CT scan is the gold standard for definitive diagnosis and preoperative planning.

Indications for Surgery
- Acute Displaced Fractures: Consider Open Reduction and Internal Fixation (ORIF) in high-demand athletes to preserve the biomechanical advantage of the ulnar finger flexors.
- Symptomatic Nonunions: Excision of the hook is the procedure of choice, offering a rapid return to sport and eliminating the risk of flexor tendon rupture.
- Ulnar Neuropathy or Tendon Irritation: Immediate excision is warranted if signs of ulnar nerve compression or flexor tendon fraying are present.
Surgical Technique: Excision of the Hamate Hook
Patient Positioning and Preparation:
* Place the patient supine on the operating table with the arm extended on a radiolucent hand table.
* Administer appropriate regional or general anesthesia.
* Prepare the skin with standard surgical solutions and exsanguinate the limb using an Esmarch bandage before inflating a pneumatic tourniquet to 250 mm Hg.
Incision and Superficial Dissection:
* Make an incision parallel to the thenar crease, extending distally into the palm. Proximally, curve the incision obliquely and medially across the wrist flexion crease. This approach exposes the hook of the hamate at the medial distal margin of the carpal tunnel.
* Carefully incise the palmar fascia longitudinally. This exposes the underlying transverse carpal ligament roofing the carpal tunnel.
* Note: For a simple excision of the hook, it is generally not necessary to completely open the carpal tunnel, though partial release may aid visualization.
Deep Dissection and Fragment Mobilization:
* Palpate the hook of the hamate with the tip of a blunt instrument (e.g., a Freer elevator).
* Incise the ligamentous and periosteal cover directly over the tip of the hook.
* Expose the hook subperiosteally. Meticulously "shuck" the soft tissue covering off the hook using a sharp elevator or scalpel until the fracture line or nonunion site is clearly visualized.
* Grasp the tip of the hook firmly with a Kocher clamp to mobilize the fracture site.
* If a nonunion is present, dense fibrosis at the base of the hook may make mobilization difficult. Carefully incise the fibrous attachments at the nonunion site.
💡 Clinical Pearl
Avoid straying ulnar or distal to the hook during your subperiosteal dissection. The ulnar nerve and artery pass from medial to distal, wrapping laterally around the base of the hook. Strict adherence to the subperiosteal plane is the only way to guarantee the safety of the deep motor branch of the ulnar nerve.
Excision and Closure:
* Remove the mobilized hook fragment.
* Inspect the remaining base of the hamate. Use a rongeur to smooth any rough bony surfaces or osteophytes that could abrade the overlying flexor tendons.
* If possible, close the periosteal and ligamentous flaps over the exposed cancellous bone of the fracture site to create a smooth gliding surface for the tendons.
* Deflate the tourniquet, obtain meticulous hemostasis, and close the skin with fine nonabsorbable sutures (e.g., 4-0 or 5-0 nylon).
Surgical Technique: Open Reduction and Internal Fixation (ORIF)
If ORIF is selected (typically for acute, large basal fractures in elite athletes), the approach is identical to that described for excision.
* In cases of ORIF, a complete release of the transverse carpal ligament is often performed to improve visualization of the fracture footprint.
* Reduce the fragment anatomically.
* Fixation is typically achieved using a single headless compression screw or multiple smooth Kirschner wires.
* Ensure the hardware is countersunk beneath the articular/cortical surface to prevent tendon attrition.
Postoperative Protocol
- Excision: Immobilize the wrist in a bulky soft dressing or a short-arm volar splint for 1 to 2 weeks to allow for wound healing. Initiate early active range of motion (ROM) of the fingers immediately. Return to sports is typically permitted at 4 to 6 weeks once grip strength returns and tenderness resolves.
- ORIF: Cast immobilization in slight radial deviation (to minimize the deforming pull of the ulnar flexors) is maintained for 4 to 6 weeks, followed by progressive rehabilitation.
TRAPEZIUM AND TRAPEZOID FRACTURES
Fractures of the trapezium and trapezoid are exceedingly rare as isolated injuries. They are most frequently encountered in conjunction with radial fracture-dislocations, first carpometacarpal (CMC) joint dislocations, or fractures of the adjacent metacarpal bases.
Trapezium Fractures
Trapezium fractures typically occur through the body of the bone or through the trapezial ridge. The trapezial ridge acts as a critical anatomical pulley for the flexor carpi radialis (FCR) tendon.
Palmer Classification of Trapezial Ridge Fractures:
Palmer classified trapezial ridge fractures into two distinct types based on the mechanism of injury and healing potential:
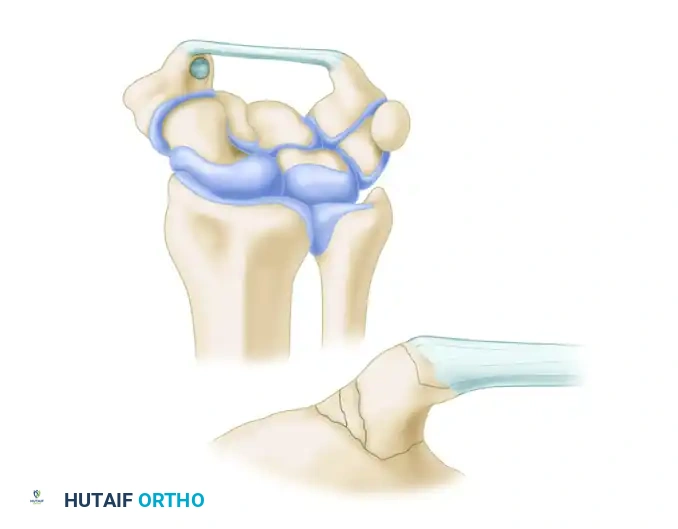
- Type I (Base Fracture): A fracture through the broad base of the trapezial ridge, typically caused by direct loading or a fall on an outstretched hand. Because of the larger cancellous surface area, Type I fractures often heal successfully when treated with rigid cast immobilization.

- Type II (Tip Avulsion): An avulsion fracture at the very tip of the ridge. This is usually caused by a sudden, forceful contraction of the transverse carpal ligament or direct trauma. Type II fractures have a high rate of nonunion when treated conservatively and frequently require surgical excision if they remain symptomatic.

Surgical Approach to the Trapezium:
* Body Fractures: Displaced fractures of the trapezial body require anatomical open reduction to prevent late first CMC arthrosis. These are best exposed through a J-shaped incision along the dorsum of the thumb metacarpal, curving medially at the wrist flexion crease. Protect the superficial sensory branches of the radial nerve.
* Ridge Fractures: Ununited fragments of the trapezial ridge can be excised using the proximal limb of the aforementioned J-shaped incision, or through a longitudinal incision in the thenar crease (similar to the carpal tunnel approach).
* Surgical Warning: When approaching the volar trapezium, meticulous care must be taken to identify and retract the palmar cutaneous branch of the median nerve to prevent painful neuroma formation.
Trapezoid Fractures
The trapezoid is the least frequently fractured carpal bone. Its keystone shape and rigid ligamentous attachments within the distal carpal row make it highly stable.
- Mechanism: Injury usually occurs secondary to high-energy axial loading through the second metacarpal, often resulting in a dorsal fracture-dislocation of the second CMC joint.
- Diagnosis: Standard radiographs frequently miss these injuries. CT or MRI is almost always required for definitive diagnosis.
- Treatment: Minimally displaced fractures can be treated with cast immobilization for 4 to 6 weeks. Displaced fractures require closed reduction and percutaneous pinning, or ORIF. Recurrence of posterior subluxation of the second metacarpophalangeal joint must be carefully monitored. In cases of late presentation or post-traumatic arthrosis, localized fusion of the trapezoid to the second metacarpal may be necessary to alleviate pain.
COMPREHENSIVE PATTERNS OF CARPAL FRACTURES
Understanding the specific morphological patterns of carpal fractures is essential for determining the appropriate conservative or surgical intervention. The following outlines the evidence-based management for the remaining carpal bones.
Lunate Fractures
Lunate fractures are categorized into palmar pole, osteochondral (chip), and dorsal pole fractures.
- Treatment: Closed treatment and casting for 4–6 weeks is appropriate for minimally displaced or small fragments. ORIF is mandated for intraarticular incongruity or associated carpal instability.
- Associated Injuries: Frequently associated with lunotriquetral or radiolunate ligament tears.
- Clinical Pearls: Beware of Kienböck disease (avascular necrosis of the lunate) if a fracture is present independent of significant trauma. Consider an MRI for the evaluation of lunate vascularity. The presence of a lunate fracture strongly suggests an underlying carpal instability pattern.
Triquetrum Fractures
Triquetral fractures are the second most common carpal fractures (after the scaphoid) and are divided into dorsal rim chip fractures and body fractures (medial tuberosity, sagittal, transverse, palmar radial, or comminuted).
- Treatment: Closed treatment with casting for 4–6 weeks is highly successful for small dorsal chip fractures or minimally displaced body fractures. Large, significantly displaced body fractures may require ORIF.
- Clinical Pearls: A dorsal avulsion fracture often represents an avulsion of the dorsal radiocarpal (DRC) and dorsal intercarpal (DIC) ligaments. If the DRC ligament is torn, the triquetrum and lunate may secondarily flex, leading to instability. Ulnar impaction syndrome or triangular fibrocartilage complex (TFCC) injuries frequently accompany triquetral body fractures. Arthroscopy may be necessary to evaluate the TFCC after the bony injury has healed.
Capitate Fractures
Capitate fractures include transverse proximal pole, transverse body, and coronal oblique patterns.

- Treatment: Cast immobilization for 4–6 weeks is reserved for strictly nondisplaced fractures. Closed reduction and Kirschner wire fixation can be used for extraarticular reducible fractures. ORIF is required for irreducible, displaced, intraarticular, or proximal pole fractures.
- Associated Injuries: Capitate fractures are the hallmark of "Scaphocapitate syndrome," which involves a concomitant scaphoid fracture and lunotriquetral ligament injury.
- Clinical Pearls: The proximal pole of the capitate is entirely intraarticular, rendering its blood supply tenuous. Displaced or rotated proximal pole fractures carry a high risk of late avascular necrosis and demand urgent ORIF. Always maintain a high index of suspicion for associated, radiographically occult perilunate injuries.
Hamate Fractures (Body and Hook)
Beyond the hook, the hamate body can fracture in several patterns: proximal pole, medial tuberosity, sagittal oblique, and dorsal coronal.
- Treatment: Cast immobilization for 4–6 weeks is suitable for minimally displaced body fractures. Displaced body or intraarticular fractures require ORIF. As discussed extensively above, symptomatic hook fractures often require excision.
- Associated Injuries: Hamate body fractures are frequently associated with fourth or fifth metacarpophalangeal fracture-dislocations. Avulsion fractures may occur at the insertion of the flexor carpi ulnaris (FCU).
- Clinical Pearls: When casting a hamate fracture, immobilizing the wrist in slight radial deviation minimizes the deforming force of the ulnar finger flexors.
Pisiform Fractures
Pisiform fractures typically present as transverse or parasagittal fracture lines.

- Treatment: Immobilization for 2–4 weeks is usually sufficient for minimally displaced or comminuted fractures.
- Surgical Indications: Consider ORIF or complete excision with tendon reconstruction if the FCU tendon is severely disrupted. Excision is also the definitive treatment for late post-traumatic pisotriquetral arthrosis.
- Clinical Pearls: Pisiform fractures are best visualized on a true lateral radiograph or a specialized carpal tunnel view. Always assess for partial or complete FCU disruption.
CONCLUSION
The operative management of rare carpal fractures requires meticulous preoperative planning, advanced cross-sectional imaging, and a profound respect for the complex neurovascular and ligamentous anatomy of the wrist. Whether performing a subperiosteal excision of a nonunited hamate hook or an anatomical ORIF of a displaced trapezial body, the surgeon's primary goal remains the restoration of carpal stability, the prevention of tendon attrition, and the mitigation of late-stage post-traumatic arthrosis. Strict adherence to evidence-based surgical approaches and tailored postoperative rehabilitation protocols are paramount to achieving optimal functional outcomes in this challenging patient population.
You Might Also Like