Advanced Arthroscopic Reduction and Fixation for Complex Wrist Fractures
Key Takeaway
In this comprehensive guide, we discuss everything you need to know about Advanced Arthroscopic Reduction and Fixation for Complex Wrist Fractures. **Arthroscopic reduction and fixation** addresses complex, displaced intra-articular distal radius and ulnar styloid fractures, which are common skeletal injuries often resulting from high-energy mechanisms. This surgical technique is crucial when traditional closed manipulation and casting are insufficient, aiming to restore joint congruity and reduce residual shortening for optimal patient prognosis.
Introduction and Epidemiology
Fractures of the distal radius represent one of the most common skeletal injuries treated by orthopaedic surgeons, accounting for approximately one-sixth of all fractures evaluated in the Emergency Department. The epidemiological profile of these injuries demonstrates a distinct bimodal age distribution, reflecting divergent mechanisms of injury across different patient populations. In young adults, these fractures typically result from high-energy trauma, such as motor vehicle collisions or falls from a significant height. Conversely, in the elderly population, they predominantly occur via low-energy mechanisms, such as falls from a standing height, secondary to decreased bone mineral density.
Patients 65 years of age or older exhibit an annual incidence of 8 to 10 fractures of the distal radius per 1000 person-years. The incidence is markedly gender-skewed, being seven times higher in women than in men. Demographic projections and epidemiological studies indicate that 16% of white women and 23% of white men will sustain a fracture of the distal radius after the age of 50 years.
Displaced intra-articular fractures of the distal radius constitute a unique and highly complex subset of these injuries. Driven by high-energy axial loading and shear forces, these injuries frequently result in severely comminuted fracture patterns. Because of the disruption of the articular surface and the displacement of metaphyseal bone, these fractures are significantly less amenable to traditional closed manipulation and casting. The long-term prognosis for these fractures is strictly dependent on the anatomic restoration of the joint. Clinical outcomes correlate directly with the amount of residual radius shortening, the restoration of both radiocarpal and radioulnar articular congruity, and the diagnosis and management of associated soft tissue injuries.

Surgical Anatomy and Biomechanics
Osseous Architecture of the Distal Radius
The distal radius serves as the critical foundational plateau supporting the carpus, facilitating load transfer from the hand to the forearm. Anatomically, the distal radius features three distinct concave articular surfaces: the scaphoid fossa, the lunate fossa, and the sigmoid notch. The scaphoid and lunate fossae are separated by an interfascial ridge, which often dictates the location of sagittal split fractures in intra-articular injury patterns.
In the coronal plane, the distal articular surface of the radius demonstrates a radial inclination averaging 22 degrees. In the sagittal plane, it exhibits a palmar tilt averaging 11 degrees. Restoration of these specific angular parameters, alongside radial height (typically 11 to 12 mm relative to the ulnar head), is paramount during surgical reconstruction to normalize carpal kinematics and load distribution.
Ligamentous Anatomy and the Triangular Fibrocartilage Complex
The stability of the radiocarpal and midcarpal joints relies heavily on a robust network of intrinsic and extrinsic ligaments. Radial-based volar and dorsal extrinsic ligaments arise from the distal radius to support the wrist. The volar radiocarpal ligaments, including the radioscaphocapitate, long radiolunate, and short radiolunate ligaments, are thick and provide primary resistance to palmar carpal translation. The intrinsic ligaments, most notably the scapholunate interosseous ligament and the lunotriquetral interosseous ligament, are critical for synchronous carpal motion.
The sigmoid notch of the distal radius articulates with the ulnar head, forming the distal radioulnar joint. The sigmoid notch angles distally and medially at an average of 22 degrees, accommodating the rotational translation of the ulnar head during forearm pronation and supination. The distal radioulnar joint is primarily stabilized by the triangular fibrocartilage complex. This complex structure comprises the central articular disc, the dorsal and volar radioulnar ligaments, the meniscal homologue, the ulnocarpal ligaments, and the extensor carpi ulnaris subsheath. Foveal detachments of the triangular fibrocartilage complex are a frequent concomitant injury in displaced distal radius fractures and a primary driver of chronic distal radioulnar joint instability.
Indications and Contraindications
Arthroscopically assisted reduction and fixation of distal radius fractures provide unparalleled visualization of the articular surface and allow for the concurrent diagnosis and treatment of intrinsic ligamentous and triangular fibrocartilage complex injuries. However, patient selection must be rigorous, balancing the benefits of enhanced visualization against the risks of fluid extravasation and prolonged operative times.
Operative Indications and Contraindications
| Parameter | Indications for Arthroscopic Assistance | Contraindications for Arthroscopic Assistance |
|---|---|---|
| Articular Displacement | Intra-articular step-off or gap > 2 mm after fluoroscopic reduction | Extra-articular fractures (unless concomitant soft tissue injury is highly suspected) |
| Soft Tissue Pathology | Suspected scapholunate or lunotriquetral ligament tears | Isolated extra-articular fractures with stable distal radioulnar joint |
| Distal Radioulnar Joint | Clinical or fluoroscopic instability of the distal radioulnar joint | Fixed, chronic distal radioulnar joint dislocations requiring open reconstruction |
| Fracture Pattern | Die-punch fragments, Fernandez Type III and V fractures | Severe metaphyseal comminution precluding stable platform for traction |
| Physiologic Factors | High-demand patients requiring precise articular restoration | Active local infection, severe medical comorbidities, polytrauma with hemodynamic instability |
| Soft Tissue Envelope | Intact fascial compartments accommodating fluid | Severe baseline swelling, impending compartment syndrome, open fractures with massive soft tissue loss |
Pre Operative Planning and Patient Positioning
Imaging Modalities and Fracture Classification
Comprehensive preoperative imaging is mandatory for surgical planning. Standard posteroanterior, lateral, and oblique radiographs of the wrist provide initial assessment of radial height, inclination, and volar tilt. For intra-articular fractures, a non-contrast computed tomography scan with sagittal and coronal reconstructions is the gold standard. Computed tomography allows precise mapping of fracture lines, identification of the dorsal lunate facet fragment, assessment of die-punch comminution, and evaluation of the sigmoid notch.
The Fernandez and Geissler classification system is highly utility-driven, categorizing fractures based on the mechanism of injury and the degree of energy absorbed.
* Type I: Bending fractures of the metaphysis where one cortex fails under tensile stress while the opposite undergoes comminution (e.g., extra-articular Colles or Smith fractures).
* Type II: Shearing fractures of the joint surface (e.g., radial styloid fractures, volar or dorsal Barton fractures).
* Type III: Compression fractures of the joint surface with impaction of the subchondral and metaphyseal cancellous bone (intra-articular comminuted fractures, die-punch injuries).
* Type IV: Avulsion fractures of ligamentous attachments, including radial and ulnar styloid fractures associated with radiocarpal fracture-dislocations.
* Type V: High-energy injuries involving a combination of bending, compression, shearing, and avulsion mechanisms, often with significant bone loss.
Operating Room Setup and Patient Positioning
The patient is positioned supine on the operating table with the operative extremity extended on a radiolucent hand table. Regional anesthesia (supraclavicular or axillary block) combined with general anesthesia or deep sedation is standard. A high-arm tourniquet is applied.

Following standard sterile prep and drape, the hand is suspended using sterile finger traps applied to the index and long fingers. A traction tower or a boom system is utilized to apply 10 to 15 pounds of longitudinal traction. This traction is critical not only for ligamentotaxis to aid in initial fracture reduction but also to open the radiocarpal space to accommodate the arthroscope. The fluoroscopy unit (C-arm) is positioned parallel to the table, allowing unimpeded orthogonal views of the wrist without compromising the sterile field or the surgeon's ergonomics.
Detailed Surgical Approach and Technique
Portal Anatomy and Establishment
Arthroscopic evaluation of the radiocarpal and midcarpal joints relies on precise portal placement to avoid iatrogenic injury to extensor tendons, superficial nerves, and vascular structures. Standard radiocarpal portals include the 3-4 portal, 4-5 portal, 6R portal, and 6U portal.
The 3-4 portal is established just distal to Lister's tubercle, between the extensor pollicis longus and the extensor digitorum communis tendons. This serves as the primary viewing portal. The 4-5 portal is located between the extensor digitorum communis and the extensor digiti minimi and is utilized primarily as the working portal. The 6R and 6U portals, located radial and ulnar to the extensor carpi ulnaris tendon respectively, are essential for evaluating and repairing the triangular fibrocartilage complex. Midcarpal portals (radial and ulnar) are established to evaluate the intrinsic ligaments from the midcarpal articulation.
To minimize the risk of compartment syndrome secondary to fluid extravasation through capsular rents, many surgeons advocate for "dry arthroscopy" or the use of gravity inflow with an open outflow system rather than a pressurized fluid pump.
Arthroscopic Hematoma Evacuation and Joint Evaluation
Upon entering the radiocarpal joint via the 3-4 portal, the initial view is typically obscured by fracture hematoma and debris. A shaver is introduced through the 4-5 portal to meticulously evacuate the hematoma, perform a limited synovectomy, and clear chondral debris. This step is critical for visualizing the fracture lines and the articular step-offs.
Once visibility is established, a systematic diagnostic arthroscopy is performed. The articular surfaces of the scaphoid and lunate fossae are inspected. The intrinsic ligaments are probed. Arthroscopic studies demonstrate a high incidence of injury to the triangular fibrocartilage complex, followed by the scapholunate interosseous ligament, and then the lunotriquetral interosseous ligament.
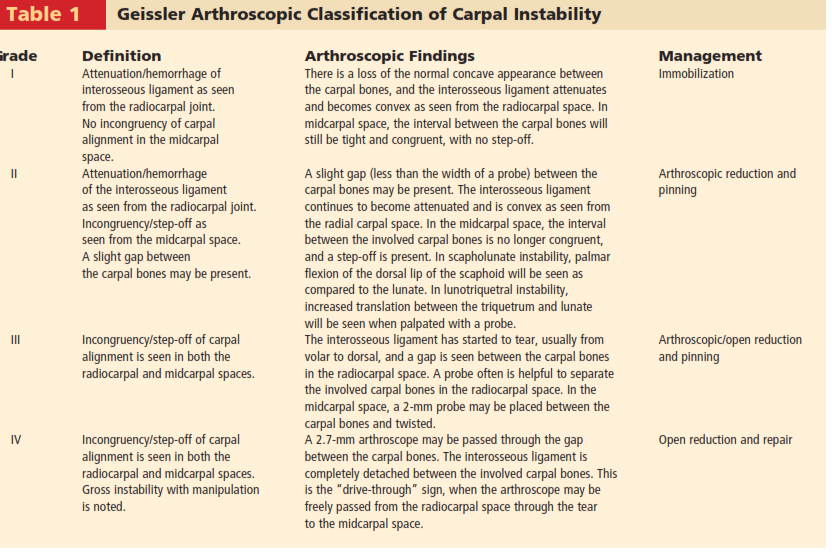
The Geissler arthroscopic classification of interosseous ligament tears is utilized to define the degree of ligamentous injury and direct subsequent management:
* Grade I: Attenuation or hemorrhage of the ligament without step-off; incongruency is not present.
* Grade II: Attenuation or tear with a slight step-off between the carpal bones; a probe cannot be passed through the interval.
* Grade III: Step-off is present, and a probe can be passed through the interosseous interval, indicating a significant tear.
* Grade IV: Complete disruption of the ligament allowing the passage of the 2.7mm arthroscope between the carpal bones (pathognomonic for gross instability).
Fracture Reduction and Fixation Strategies
Arthroscopic-assisted reduction is typically performed in conjunction with volar locking plate fixation. The volar approach (modified Henry) is performed first. The flexor carpi radialis tendon sheath is incised, and the tendon is retracted ulnarly. The floor of the sheath is incised to expose the pronator quadratus, which is elevated from its radial border to expose the distal radius metaphysis.
The volar plate is provisionally applied to the proximal radial shaft. Under arthroscopic visualization, intra-articular step-offs and gaps are directly addressed. Depressed articular fragments (die-punch) are elevated using a bone tamp or freer elevator introduced through the metaphyseal fracture window or via a dedicated dorsal portal. Once the articular surface is anatomically reduced (aiming for less than 1 mm of step-off), the fragments are provisionally stabilized with subchondral K-wires.

The distal locking screws of the volar plate are then inserted. The arthroscope provides real-time, direct visualization to ensure that no screws penetrate the radiocarpal joint—a complication that fluoroscopy alone may fail to detect due to the complex three-dimensional anatomy of the distal radius.
Management of Concomitant Soft Tissue Injuries
Following rigid skeletal fixation, attention is turned to the soft tissue envelope.
* Scapholunate Ligament Tears: Geissler Grade III and IV tears require intervention. Acute tears can be managed with arthroscopic debridement, thermal shrinkage (for Grade II), or percutaneous K-wire pinning (scaphoid-to-lunate and scaphoid-to-capitate) for 8 weeks. Complete avulsions may necessitate open dorsal repair and capsulodesis.
* Triangular Fibrocartilage Complex Tears: Peripheral tears (Palmer Class 1B) are highly amenable to arthroscopic repair. Using an inside-out or outside-in technique through the 6R and 6U portals, sutures are passed through the articular disc and tied over the dorsal ulnar capsule. Foveal detachments may require transosseous suture anchors placed into the ulnar fovea.
Complications and Management
Arthroscopic assistance in distal radius fracture fixation introduces specific technical challenges and potential complications distinct from standard open reduction and internal fixation. Meticulous surgical technique and strict adherence to fluid management protocols are required to mitigate these risks.
Summary of Complications and Salvage Strategies
| Complication | Incidence / Risk Factors | Clinical Presentation | Management and Salvage Strategies |
|---|---|---|---|
| Fluid Extravasation / Compartment Syndrome | Highest in high-energy injuries with extensive capsular tearing; exacerbated by pressurized infusion pumps. | Disproportionate forearm pain, tight compartments, pain with passive digital extension. | Immediate cessation of fluid. Use "dry arthroscopy" techniques. If compartment syndrome is confirmed, emergent volar and dorsal forearm fasciotomies. |
| Intra-articular Hardware Penetration | Occurs when distal locking screws breach the subchondral bone; often missed on standard 2D fluoroscopy. | Crepitus with wrist ROM, mechanical block, delayed chondrolysis, or tendon irritation. | Direct arthroscopic visualization during screw placement. Immediate exchange for shorter screws if penetration is visualized. |
| Iatrogenic Tendon or Nerve Injury | Related to aberrant portal placement (e.g., superficial radial nerve at 1-2 portal, dorsal ulnar sensory nerve at 6U). | Postoperative neuropathic pain, paresthesias, or extensor lag (EPL rupture). | Strict adherence to anatomic landmarks. Use blunt dissection down to the capsule. Late EPL ruptures require extensor indicis proprius transfer. |
| Post-Traumatic Wrist Stiffness | Common in combined osseous and ligamentous injuries requiring prolonged immobilization. | Decreased radiocarpal and midcarpal motion, impaired grip strength. | Early aggressive occupational therapy. If refractory after 6 months, arthroscopic capsular release and manipulation under anesthesia. |
| Complex Regional Pain Syndrome | Associated with severe trauma, tight cast/splint, or unrecognized nerve irritation. | Allodynia, hyperalgesia, sudomotor/vasomotor changes, trophic skin changes. | Multidisciplinary approach: early mobilization, Vitamin C prophylaxis (500mg daily for 50 days), gabapentinoids, sympathetic nerve blocks. |
Post Operative Rehabilitation Protocols
Phased Recovery and Functional Restoration
The postoperative rehabilitation protocol must be carefully tailored to the stability of the fracture fixation and the presence of any concomitant soft tissue repairs.
Phase I: Immediate Postoperative Period (0 to 2 Weeks)
The wrist is immobilized in a bulky Jones dressing and a volar orthosis. If a scapholunate pinning or triangular fibrocartilage complex repair was performed, a Muenster or sugar-tong splint may be utilized to restrict forearm rotation. Immediate active range of motion of the digits, elbow, and shoulder is initiated to prevent stiffness and reduce edema. Edema control techniques, including elevation and retrograde massage, are emphasized.
Phase II: Early Mobilization (2 to 6 Weeks)
Sutures are removed at 10 to 14 days. If isolated rigid bony fixation was achieved without major ligamentous repair, the patient is transitioned to a removable custom thermoplastic splint. Active and active-assisted range of motion of the wrist (flexion, extension, pronation, supination) is initiated. If K-wires were placed for intercarpal instability, wrist motion is deferred until wire removal at 6 to 8 weeks.
Phase III: Strengthening and Functional Restoration (6 to 12 Weeks)
Radiographic union is typically confirmed between 6 and 8 weeks. Splinting is discontinued. Progressive resistive exercises and weight-bearing activities are introduced. Dynamic splinting may be employed if significant capsular contractures are present. Return to heavy manual labor or contact sports is generally restricted until 12 to 16 weeks postoperatively, contingent upon the restoration of grip strength to at least 80% of the contralateral extremity.
Summary of Key Literature and Guidelines
The paradigm shift toward arthroscopic-assisted management of distal radius fractures is supported by a robust body of orthopaedic literature. Traditional fluoroscopy has been shown to have significant limitations in detecting minor articular step-offs and identifying intrinsic carpal ligament tears.
Several landmark studies have elucidated the high incidence of associated soft tissue injuries seen with displaced intra-articular distal radius fractures. Forward et al. and Richards et al. demonstrated that fluoroscopy frequently fails to detect articular incongruities of less than 2 mm, which are readily visualized and corrected via arthroscopy. Furthermore, Geissler’s foundational arthroscopic studies revealed that up to 70% of intra-articular distal radius fractures are associated with tears of the triangular fibrocartilage complex, and up to 30% have concomitant scapholunate interosseous ligament tears.
The spectrum of injury to the interosseous ligaments dictates that untreated high-grade tears (Geissler Grade III and IV) lead to progressive carpal instability, dorsal intercalated segment instability, and eventual post-traumatic osteoarthritis (scapholunate advanced collapse). Current academic guidelines strongly recommend arthroscopic evaluation for any high-energy, displaced intra-articular distal radius fracture, particularly Fernandez Type III and V patterns, to ensure anatomic articular restoration and the comprehensive management of the "hidden" soft tissue lesions that dictate long-term functional outcomes.
Clinical & Radiographic Imaging
You Might Also Like