Sesamoid Injuries of the Hallux: Comprehensive Surgical Guide
Key Takeaway
Hallux sesamoid injuries encompass a spectrum of pathologies including acute fractures, stress fractures, osteochondritis dissecans, and chronic sesamoiditis. Accurate diagnosis relies on precise clinical examination and specialized radiographic projections, particularly the axial sesamoid view. Management ranges from conservative offloading to surgical excision. This guide details the biomechanics, diagnostic algorithms, and step-by-step surgical approaches required to optimize patient outcomes and prevent debilitating first ray deformities.
INTRODUCTION TO HALLUX SESAMOID PATHOLOGY
The hallux sesamoid complex is a critical biomechanical engine of the forefoot, functioning to absorb weight-bearing forces, reduce friction, and protect the flexor hallucis longus (FHL) tendon. Because of an increased awareness of pathological conditions affecting the first metatarsophalangeal (MTP) joint, injuries to the sesamoids during sports activities or falls from heights are now recognized more rapidly. However, more subtle pathological conditions frequently escape initial diagnosis, leading to chronic pain and functional impairment.
Historically, chronic inflammatory conditions of a traumatic, infectious, or arthritic origin have been grouped under the non-specific diagnosis of "sesamoiditis." Modern orthopedic practice demands a more precise diagnostic approach. Inflamed bursae, intractable plantar keratoses (IPK), or diffuse callus beneath the tibial sesamoid may herald underlying, severe sesamoid pathology. Furthermore, conditions such as chondromalacia, flexor hallucis brevis (FHB) tendinitis, osteochondritis dissecans (OCD), and acute or stress fractures all occur within the sesamoids and require distinct management algorithms.
Clinical Pearl: The term "sesamoiditis" should be considered a diagnosis of exclusion. The surgeon must aggressively rule out fracture, osteonecrosis, and chondromalacia before settling on a purely inflammatory etiology.
ANATOMY AND BIOMECHANICS
The first MTP joint is supported by a complex capsuloligamentous network. The two sesamoids—tibial (medial) and fibular (lateral)—are embedded within the medial and lateral slips of the flexor hallucis brevis (FHB) tendon. They articulate dorsally with the plantar facets of the first metatarsal head, separated by the intersesamoidal crista.
Biomechanical Function
- Force Transmission: The sesamoids absorb up to 300% of body weight during the push-off phase of the gait cycle.
- Mechanical Advantage: They act as a fulcrum, increasing the moment arm of the FHB, thereby enhancing plantarflexion power at the first MTP joint.
- Tendon Protection: They elevate the metatarsal head, creating a protective channel for the FHL tendon to glide without impingement.
The tibial sesamoid is the most commonly injured of the two. This vulnerability is due to its central location directly beneath the medial condyle of the first metatarsal head, where it bears a disproportionate amount of weight during the propulsive phase of gait.
MECHANISMS OF INJURY
Hyperextension combined with axial loading is the most common mechanism of injury resulting in an acute fracture or a severe sprain of the capsuloligamentous complex (often termed "turf toe" when involving the plantar plate).
Repetitive stress is another primary etiology. Repetitive microtrauma through a syndesmotic union of a bipartite sesamoid can progressively weaken the junction. Over time, this chronic stress can result in a displaced "fracture" through the synchondrosis, leading to severe pain and dysfunction.
CLINICAL EVALUATION
On physical examination, patients often present with an antalgic gait, avoiding push-off on the medial column. Initially, diffuse tenderness may be present around the entire metatarsophalangeal joint.
Palpation and Provocative Testing
With careful, isolated palpation of each sesamoid, the tenderness usually becomes highly localized.
* Technique: Passively dorsiflex the hallux to draw the sesamoids distally from beneath the metatarsal head. This exposes them to direct plantar palpation, allowing the surgeon to differentiate between tibial and fibular sesamoid pathology.
* Differential Diagnosis: Any patient complaining of pain around the first MTP joint should have a thorough evaluation of the sesamoids to rule out FHL tendinitis, gout, septic arthritis, or a plantar plate rupture.
Surgical Warning: Do not mistake a diffuse first MTP joint effusion for simple gout or osteoarthritis without specifically palpating the sesamoids. Missed sesamoid fractures can lead to rapid joint destruction and intractable pain.
RADIOGRAPHIC EVALUATION
Routine radiographs are the cornerstone of initial evaluation, though standard views often fail to isolate the pathology. The standard lateral view of the foot is usually obscured by the lesser metatarsals and is not revealing.
Anteroposterior (AP) and Oblique Views
Standing AP views allow for a comparison of the sesamoids. This is especially helpful if a fracture is suspected but a bipartite sesamoid is present. Accessory sesamoids are normal, although uncommon, findings.

FIGURE 81-100 A: Standing anteroposterior view of both feet on the same cassette allows comparison of sesamoids. This is especially helpful if a fracture is suspected but a bipartite sesamoid is present. Accessory sesamoids (arrows) are normal, although uncommon, findings.
The oblique view is critical for profiling the fibular sesamoid.

FIGURE 81-100 B: Oblique view profiles the fibular sesamoid. Note the cystic fibular sesamoid on the right foot. This probably represents an old fracture through the syndesmotic union of a bipartite sesamoid.
For the tibial sesamoid, a specific medial oblique (sesamoid) view is highly helpful.
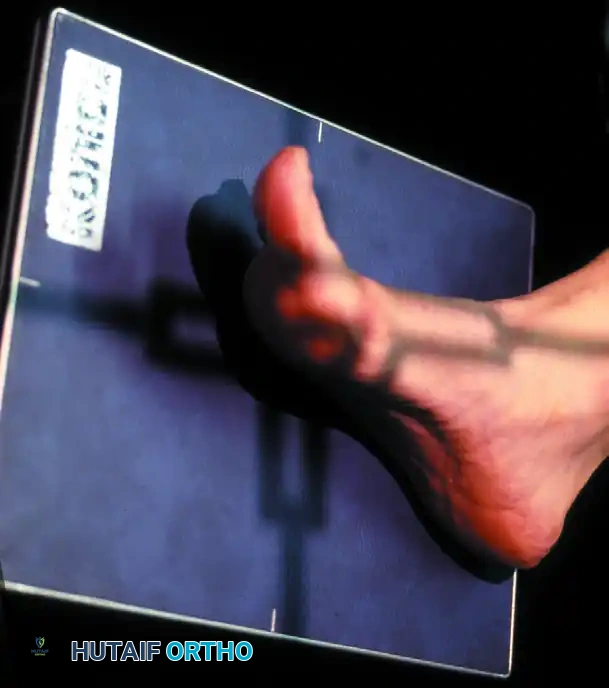
FIGURE 81-101 A: Position of the foot for the medial oblique view.

FIGURE 81-101 B: Tibial sesamoid profiled on the medial oblique view.
The Axial Sesamoid View
The axial sesamoid view should always be obtained if a sesamoid pathological condition is suspected. It provides a tangential look at the articular surface, the crista, and the joint space.

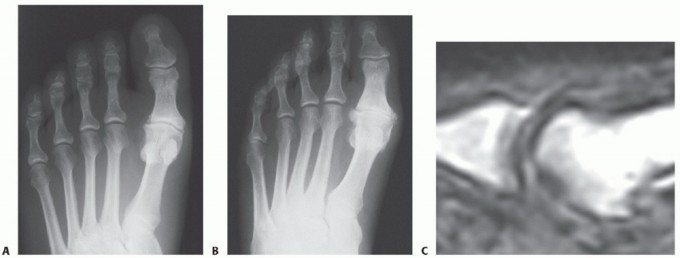
FIGURE 81-102 A: Hallux valgus deformity on AP radiograph.

FIGURE 81-102 B: On the axial sesamoid view, degenerative changes are present with subluxation of the sesamoids laterally.
Techniques for Axial Imaging
Proper positioning is paramount for a diagnostic axial view. The patient can be positioned standing on an inclined plane to simulate weight-bearing forces.

FIGURE 81-103 A: View may be taken with the patient standing on an inclined plane.

FIGURE 81-103 B: Axial sesamoid view taken from the front while the patient stands on an inclined plane.

FIGURE 81-103 C: Close-up of the axial sesamoid projection technique.
Additional variations of the axial projection can be utilized depending on patient mobility and equipment availability:
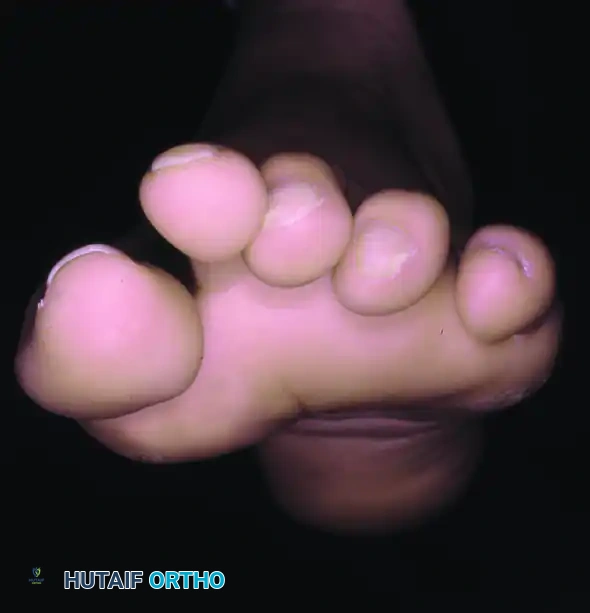
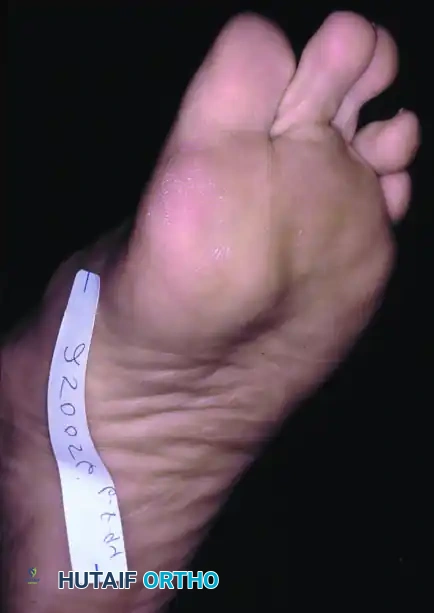
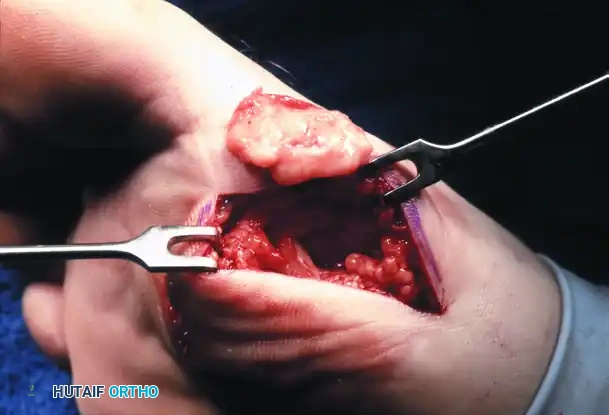

FIGURE 81-103 D-G: Alternative techniques for obtaining axial sesamoid views, ensuring the X-ray beam is tangential to the metatarsal head articular surface.
Evaluating the Fibular Sesamoid
Oblique radiography is particularly helpful for evaluating the fibular sesamoid, which rests between the first and second metatarsals.

FIGURE 81-105 A: Oblique radiography demonstrating the fibular sesamoid.

FIGURE 81-105 B: Note the irregular lucency within the fibular sesamoid, indicating a traumatic etiology.
Advanced Imaging: Bone Scans and MRI
If these radiographic views are normal, but a sesamoid pathological condition is highly suspected, a technetium-99m bone scan or an MRI may be helpful.
When ordering a bone scan, the nuclear medicine department must be explicitly informed that the sesamoids are under question so they can modify the projections accordingly (e.g., pinhole collimator views). The projections are important to rule out intraarticular metatarsophalangeal joint pathological conditions. Today, MRI is frequently preferred over bone scans as it provides superior soft-tissue contrast, identifying bone marrow edema, osteonecrosis, and associated plantar plate or FHB tears.
Bipartite Sesamoid vs. Fracture
A bipartite tibial sesamoid is present in about 10% of the population, and in 25% of these individuals, the condition is bilateral. For this reason, the surgeon must be certain that a tender sesamoid with a radiolucent division through it is a true fracture and not a symptomatic bipartite sesamoid.
- Radiographic Clues: A bipartite sesamoid typically has smooth, well-corticated, rounded edges. A fracture will exhibit sharp, irregular, uncorticated margins.
- Fibular Sesamoid: The fibular sesamoid is rarely bipartite. If clinical symptoms and routine radiographs suggest a fracture of the fibular sesamoid, one is usually present. A bone scan or MRI is an excellent means of confirming this.
NON-OPERATIVE MANAGEMENT
Conservative management is the first line of treatment for sesamoiditis, stress fractures, and non-displaced acute fractures.
- Immobilization: Acute fractures should be managed with a short leg cast or a rigid fracture boot extending past the toes for 4 to 6 weeks, keeping the patient non-weight-bearing or heel-weight-bearing.
- Offloading: For sesamoiditis or chronic stress injuries, a stiff-soled shoe with a custom orthotic featuring a "dancer's pad" (a U-shaped cutout under the affected sesamoid) is highly effective.
- Activity Modification: Cessation of high-impact sports, jumping, and running until asymptomatic.
- Injections: Corticosteroid injections should be used with extreme caution. While they may reduce bursal inflammation, intra-tendinous injection risks FHB rupture, and intra-articular injection may accelerate chondromalacia or osteonecrosis.
OPERATIVE MANAGEMENT
Surgical intervention is indicated when conservative measures fail after 3 to 6 months, or in cases of widely displaced acute fractures, severe osteonecrosis, or intractable symptomatic non-unions.
Preoperative Planning
The decision to perform a partial versus total sesamoidectomy depends on the pathology.
* Partial Sesamoidectomy: Preferred for proximal or distal pole fractures to preserve the FHB continuity.
* Total Sesamoidectomy: Indicated for severe comminution, advanced osteonecrosis, or diffuse arthritic changes.
Pitfall: Excision of both sesamoids (tibial and fibular) should be avoided whenever possible. Bilateral excision eliminates the mechanical advantage of the FHB, leading to a severe "cock-up" deformity (hyperextension of the MTP joint and flexion of the IP joint) due to the unopposed pull of the extensor hallucis longus.
Surgical Approach: Tibial Sesamoidectomy
Positioning: Supine with a bump under the ipsilateral hip to externally rotate the leg. A calf or thigh tourniquet is applied.
- Incision: Make a 4 to 5 cm longitudinal incision along the medial aspect of the first MTP joint, centered over the tibial sesamoid. The incision should be slightly plantar to the midline of the medial eminence to avoid the dorsal medial cutaneous nerve, but dorsal enough to avoid the weight-bearing plantar skin.
- Dissection: Deepen the incision through the subcutaneous tissue. Identify and carefully retract the medial plantar digital nerve, which courses directly plantar to the sesamoid.
- Capsulotomy: Incise the capsule and the medial slip of the FHB longitudinally.
- Excision: Using a #15 blade, carefully shell the sesamoid out of its tendinous envelope. Keep the blade strictly on the bone to avoid severing the FHB tendon or the intersesamoidal ligament.
- Tendon Repair: This is the most critical step. The defect left in the FHB and plantar capsule must be meticulously repaired with heavy non-absorbable sutures (e.g., #0 or 2-0 FiberWire). Failure to repair the medial structures will result in an unopposed pull of the adductor hallucis and the lateral FHB, leading to an iatrogenic hallux valgus deformity.
- Closure: Close the skin in a standard fashion and apply a compressive dressing.
Surgical Approach: Fibular Sesamoidectomy
The fibular sesamoid is technically more demanding to excise due to its deep location and proximity to the neurovascular bundle. Two approaches are utilized: Dorsal and Plantar.
The Dorsal Approach (Preferred)
- Incision: Make a dorsal longitudinal incision in the first web space.
- Dissection: Identify and protect the deep peroneal nerve branches and the first dorsal metatarsal artery.
- Release: Identify the adductor hallucis tendon. To access the sesamoid, the deep transverse metatarsal ligament must be divided.
- Excision: Retract the adductor hallucis dorsally and laterally. Incise the lateral capsule and shell out the fibular sesamoid from the lateral slip of the FHB.
- Repair: The lateral capsular structures and the adductor hallucis must be repaired or reapproximated to prevent an iatrogenic hallux varus deformity.
The Plantar Approach
Note: This approach provides direct access but carries a higher risk of painful scar formation on the weight-bearing surface and injury to the plantar digital nerve.
1. Incision: Make a longitudinal incision directly over the fibular sesamoid on the plantar aspect, slightly lateral to the weight-bearing axis of the first metatarsal.
2. Dissection: Bluntly dissect through the plantar fat pad. Identify and retract the lateral plantar digital nerve to the hallux.
3. Excision: Incise the FHB longitudinally and excise the bone.
4. Closure: Repair the tendon defect meticulously. Close the skin with non-absorbable sutures, leaving them in place for 3 weeks to ensure healing of the thick plantar skin.
POSTOPERATIVE PROTOCOL
- Phase 1 (0-2 Weeks): The patient is placed in a rigid postoperative shoe or fracture boot. Weight-bearing is restricted to the heel. Elevation and strict edema control are mandatory.
- Phase 2 (2-6 Weeks): Sutures are removed at 2 to 3 weeks. The patient may begin progressive flat-foot weight-bearing in a stiff-soled boot. Gentle, passive plantarflexion exercises are initiated to prevent capsular scarring, but active dorsiflexion is restricted to protect the FHB repair.
- Phase 3 (6-12 Weeks): Transition to a supportive athletic shoe with a custom orthotic or Morton's extension. Active range of motion and strengthening exercises begin.
- Return to Play: Athletes typically return to full, unrestricted high-impact activities between 3 to 6 months postoperatively, contingent upon radiographic healing (if partial excision/repair was performed) and the restoration of symmetric push-off strength.
CONCLUSION
Pathologies of the hallux sesamoids require a high index of suspicion, precise clinical examination, and targeted radiographic evaluation—most notably the axial sesamoid view. While conservative management is highly effective for inflammatory and stress-related conditions, surgical excision remains a reliable option for recalcitrant cases. Meticulous surgical technique, specifically the preservation and repair of the flexor hallucis brevis tendon complex, is paramount to preventing postoperative deformities and restoring the biomechanical integrity of the first ray.
You Might Also Like