Open Reduction of First Metatarsophalangeal Joint Dislocation: A Comprehensive Surgical Guide
Key Takeaway
First metatarsophalangeal (MTP) joint dislocations are complex injuries often requiring open reduction when the plantar plate or sesamoid complex blocks closed reduction. Utilizing a midline medial approach allows for direct visualization of the incarcerated structures, meticulous repair of the collateral ligaments, and stable anatomic restoration. This guide details the step-by-step surgical technique, biomechanical considerations, and postoperative protocols to optimize functional outcomes and minimize post-traumatic arthrosis.
Introduction to First Metatarsophalangeal Joint Dislocations
Dislocations of the first metatarsophalangeal (MTP) joint are relatively uncommon but highly debilitating injuries. The first MTP joint is a critical biomechanical pivot point during the terminal stance phase of gait, bearing up to 119% of body weight. The inherent stability of this joint is provided by a robust capsuloligamentous complex, including the plantar plate, the sesamoid apparatus, and the collateral ligaments.
Traumatic dislocation typically occurs secondary to a high-energy axial load applied to a hyperextended foot, forcing the proximal phalanx into extreme dorsiflexion. While some dislocations can be managed with closed reduction, complex dislocations—particularly those where the metatarsal head becomes incarcerated within the intrinsic musculature and the plantar plate—demand prompt surgical intervention. The midline medial approach is the gold standard for open reduction, providing excellent visualization of the medial capsular structures while minimizing the risk to the dorsal neurovascular bundle.
Surgical Anatomy and Biomechanics
A profound understanding of the first MTP joint anatomy is non-negotiable for successful surgical reconstruction. The joint is a modified hinge joint, but its stability relies heavily on its soft-tissue envelope rather than its bony architecture.

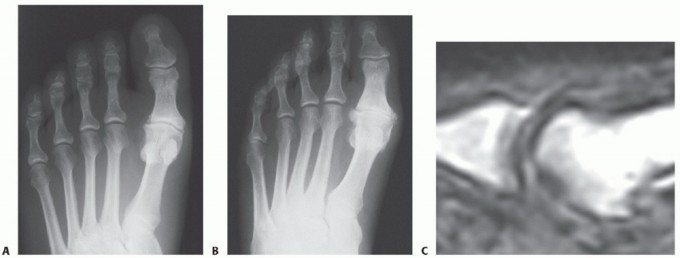
FIGURE 88-78 A: Normal anatomy of the first metatarsophalangeal joint, demonstrating the relationship of the metatarsal head to the proximal phalanx and the underlying sesamoid complex.
The Plantar Plate and Sesamoid Complex
The plantar plate is a thick, fibrocartilaginous structure that originates from the metatarsal neck and inserts firmly onto the plantar base of the proximal phalanx. Embedded within the flexor hallucis brevis (FHB) tendons are the medial (tibial) and lateral (fibular) sesamoids, which articulate with the plantar aspect of the first metatarsal head.
Clinical Pearl: The sesamoids function as a fulcrum, increasing the mechanical advantage of the FHB and protecting the flexor hallucis longus (FHL) tendon, which glides between them. The intersesamoid ligament connects the two sesamoids; its integrity dictates the reducibility of the dislocation.
The Collateral Ligaments
The collateral ligament complex consists of the proper collateral ligaments (connecting the metatarsal head to the proximal phalanx) and the accessory collateral ligaments (connecting the metatarsal head to the plantar plate and sesamoids). Rupture or avulsion of these ligaments, particularly the tibial collateral ligament, is a hallmark of lateral or dorsal dislocations.
Classification of First MTP Joint Dislocations
The Jahss Classification is the universally accepted system for categorizing dorsal dislocations of the first MTP joint. It is based on the integrity of the plantar plate and the intersesamoid ligament, which directly influences whether the dislocation can be reduced closed.
Type I Dislocation
In a Type I dislocation, the intersesamoid ligament remains intact. The entire plantar plate and sesamoid complex are avulsed from their metatarsal attachment and displace dorsally over the metatarsal head.
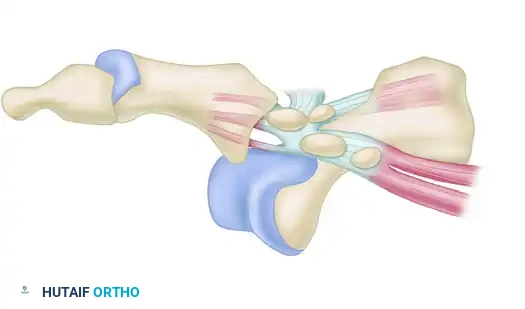
FIGURE 88-78 B: Type I dislocation. The intact intersesamoid ligament traps the metatarsal head, making closed reduction impossible.
Surgical Warning: Type I dislocations are almost universally irreducible by closed means. The metatarsal head becomes tightly incarcerated between the FHB tendons, the intact intersesamoid ligament, and the plantar plate. Applying longitudinal traction without hyperextension will only tighten this "noose" around the metatarsal neck.
Type IIA Dislocation
In a Type IIA dislocation, the intersesamoid ligament is ruptured. The medial and lateral sesamoids separate, allowing the metatarsal head to pass between them.
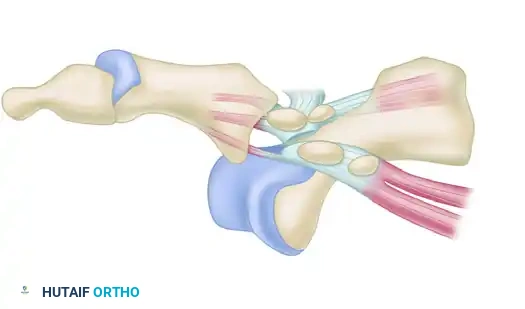
FIGURE 88-78 C: Type IIA dislocation. The ruptured intersesamoid ligament typically allows for successful closed reduction.
Type IIB Dislocation
A Type IIB dislocation involves a transverse fracture of one of the sesamoids (usually the medial sesamoid) along with a rupture of the intersesamoid ligament.
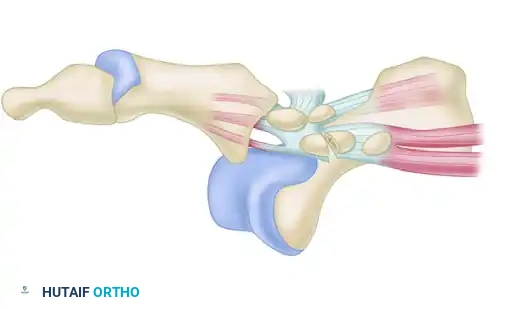
FIGURE 88-78 D: Type IIB dislocation. The sesamoid fracture acts as a release, often permitting closed reduction, though surgical repair may be indicated for the fracture.
Indications for Open Reduction
Surgical intervention via a midline medial approach is indicated in the following scenarios:
* Irreducible Dislocations: Primarily Jahss Type I dislocations where the metatarsal head is buttonholed through the capsule.
* Unstable Reductions: Cases where the joint redislocates upon testing range of motion, indicating severe capsuloligamentous incompetence.
* Open Dislocations: Requiring urgent irrigation, debridement, and stabilization.
* Concomitant Intra-articular Fractures: Fractures of the metatarsal head or proximal phalanx base that require anatomic restoration.
Preoperative Planning and Positioning
Imaging
Standard weight-bearing (if possible) anteroposterior (AP), lateral, and oblique radiographs of the foot are mandatory. The lateral view is critical for assessing the dorsal displacement of the proximal phalanx and the position of the sesamoids relative to the metatarsal head. Computed Tomography (CT) may be utilized if an occult intra-articular fracture is suspected.
Patient Positioning and Anesthesia
- Anesthesia: General anesthesia or a regional popliteal block with a saphenous nerve block is recommended to ensure complete muscle relaxation.
- Positioning: The patient is placed in the supine position on a radiolucent operating table.
- Tourniquet: A well-padded thigh or calf tourniquet is applied and inflated to provide a bloodless surgical field.
- Preparation: The foot and ankle are prepped and draped in a standard sterile orthopedic fashion.
Surgical Technique: Midline Medial Approach
The midline medial approach is preferred over a dorsal approach as it provides direct access to the medial collateral ligament, the medial sesamoid, and the plantar plate, while avoiding the extensor hallucis longus (EHL) tendon and the dorsal neurovascular structures.
Step 1: Incision and Superficial Dissection
- Make a medial longitudinal incision on the great toe, approximately 5 cm in length.
- Center the incision directly over the medial eminence of the first metatarsophalangeal joint.
- Crucial Technique: Use sharp dissection through the skin only. The medial dorsal cutaneous nerve and the medial plantar proper digital nerve course in close proximity to this incision. Meticulous blunt dissection in the subcutaneous tissues is required to avoid injuring any displaced or stretched cutaneous nerves.
Step 2: Deep Dissection and Joint Exposure
- Elevate the dorsal flap in the same manner as one would during a standard hallux valgus (bunion) repair.
- Carefully retract the dorsal soft tissues to expose the dorsal capsule.
- Assess the magnitude of the injury. Systematically inspect the following structures:
- The medial (tibial) collateral ligament.
- The dorsal capsule.
- The plantar plate and the enclosed sesamoid complex.
- In a typical irreducible dorsal dislocation, the metatarsal head will be found protruding medially and plantarly, having buttonholed through the medial capsule.
Step 3: The Reduction Maneuver
- Do not simply pull longitudinally on the toe, as this will tighten the intrinsic muscles around the metatarsal neck.
- Instead, insert a small Freer elevator or a smooth periosteal elevator into the joint space.
- Hyperextend the great toe to recreate the deformity and relax the plantar structures.
- While maintaining hyperextension, apply gentle distal traction.
- Use the Freer elevator to carefully pry and guide the base of the proximal phalanx over the dorsal lip of the metatarsal head.
- Once the phalanx clears the metatarsal head, plantarflex the toe to snap the joint into its anatomically reduced position.
Step 4: Capsuloligamentous Repair
- Following reduction, thoroughly irrigate the joint to remove any hematoma or osteochondral debris.
- Repair the torn collateral ligament (most commonly the tibial collateral ligament) and the dorsal capsule.
- Utilize heavy absorbable sutures (e.g., 2-0 or 0 Vicryl) in an interrupted or figure-of-eight fashion. Ensure the repair is robust enough to withstand early passive motion.
Step 5: Assessment of Stability
- Once the repair is complete, assess the dynamic stability of the metatarsophalangeal joint.
- Perform gentle passive flexion and extension of the MTP joint.
- Simultaneously flex and extend the ankle joint; this produces a tenodesis effect, pulling on the long flexor tendons (FHL) to ensure the joint remains congruous under physiologic tension.
Step 6: Adjunctive Internal Fixation (If Unstable)
- If the reduction appears unstable or if the capsular tissues are too attenuated to hold the joint congruous, temporary transarticular fixation is mandatory.
- Drive a small Kirschner wire (0.045-inch or 0.062-inch) longitudinally across the MTP joint from distal to proximal.
- Ensure the joint is held in a neutral or slightly extended position (10 to 15 degrees of dorsiflexion) during pinning.
- Bend the K-wire outside the skin and cap it to prevent migration. This wire will be removed 3 weeks after surgery in the outpatient clinic.
Step 7: Closure
- Deflate the tourniquet and secure meticulous hemostasis using electrocautery. Hematoma formation can lead to severe postoperative stiffness.
- Close the skin with nonabsorbable, interrupted sutures (e.g., 3-0 or 4-0 Nylon).
Management of Concomitant Intra-articular Fractures
In high-energy trauma, a first MTP joint dislocation may be complicated by an intra-articular fracture severely displaced into the interphalangeal or metatarsophalangeal joint of the great toe. These variants require Open Reduction and Internal Fixation (ORIF) to prevent severe angular deformity, joint incongruity, and rapid-onset post-traumatic arthritic changes.

FIGURE 88-79 A: Preoperative radiograph demonstrating a severely displaced intra-articular phalangeal fracture associated with joint subluxation.
Fracture ORIF Technique
- Exposure: The fracture and the joint are exposed through the same medial longitudinal approach, extended distally if necessary.
- Reduction: The fracture fragments are debrided of hematoma and reduced anatomically using pointed reduction forceps.
- Fixation: With a power drill, small 0.045-inch Kirschner wires are inserted for internal fixation. Depending on the fracture pattern, these wires may be crossed or placed parallel to achieve absolute stability.
- Alternative Fixation: For larger, distinct fracture fragments, 1.5 mm or 2.0 mm mini-fragment screws may be used to provide interfragmentary compression.

FIGURE 88-79 B: Postoperative radiograph showing anatomic reduction and stabilization of the phalangeal fracture using crossed Kirschner wires.
Clinical Pearl: When K-wires are used for fracture fixation, they are typically bent and left outside the skin. They are generally removed 3 to 4 weeks after surgery when early fracture callus has stabilized the fragments. Unlike pure ligamentous dislocations, isolated fracture fixations may not require a cast; protected weight-bearing in a stiff-soled surgical shoe can begin as soon as soft tissue healing permits.
Postoperative Care and Rehabilitation Protocol
The postoperative protocol must balance the need for tissue healing with the prevention of debilitating joint stiffness (hallux rigidus).
Phase 1: Immediate Postoperative Period (Weeks 0-3)
- Immobilization: Apply a short-leg cast that extends distal to the toes. This is placed over a bulky, well-padded forefoot dressing.
- Positioning: The dressing and cast must hold the great toe congruously on the metatarsal head in exactly 10 to 15 degrees of extension. Excessive extension can stretch the plantar repair, while flexion can lead to a functionally limiting contracture.
- Weight-Bearing: Partial weight-bearing with crutches is allowed. Elevation is critical to manage edema.
- Hardware Management: If a transarticular K-wire was utilized for joint stability, it is removed in the clinic at the 3-week mark.
Phase 2: Intermediate Rehabilitation (Weeks 3-6)
- Immobilization Removed: The short-leg cast is discontinued.
- Footwear: The patient is transitioned to full weight-bearing while wearing a stiff-soled surgical shoe or a supportive shoe with a wide toe box to prevent medial/lateral compression of the healing joint.
- Orthotics: A toe spacer is placed in the first web space for an additional 3 weeks to maintain alignment and prevent valgus drift.
- Physical Therapy: Active and active-assisted range of motion (ROM) exercises of the first MTP joint are initiated immediately upon cast removal. Plantarflexion exercises are emphasized to stretch the dorsal capsule.
Phase 3: Long-Term Outcomes and Expectations (Months 2+)
- Patients must be counseled preoperatively and postoperatively regarding long-term expectations.
- Stiffness: A permanent reduction in the terminal range of motion of the first metatarsophalangeal joint is to be expected due to capsular scarring.
- Function: Despite the loss of terminal motion, functional, pain-free motion required for normal gait should be regained after several months of diligent rehabilitation.
- Return to Play: Athletes may require 4 to 6 months before returning to high-impact sports, often requiring a rigid carbon-fiber insert in their cleat or shoe to protect the joint from extreme dorsiflexion forces.
Complications and Pitfalls
- Avascular Necrosis (AVN): The metatarsal head is susceptible to AVN following severe dislocations. Extensive soft-tissue stripping during the surgical approach must be avoided.
- Post-Traumatic Hallux Rigidus: The most common complication. Meticulous anatomic reduction, removal of all intra-articular debris, and strict adherence to the early motion protocol at 3 weeks are the best preventative measures.
- Redislocation: Usually the result of unrecognized plantar plate incompetence or premature weight-bearing without adequate immobilization. If the joint is unstable intraoperatively, do not hesitate to use a transarticular K-wire.
- Nerve Injury: Iatrogenic injury to the medial dorsal cutaneous nerve during the initial incision can lead to painful neuromas. Always use blunt dissection in the subcutaneous plane.
By adhering to strict anatomical principles, utilizing the midline medial approach for optimal exposure, and respecting the delicate biomechanics of the sesamoid complex, orthopedic surgeons can reliably restore function and stability to the dislocated first metatarsophalangeal joint.
You Might Also Like