Cheilectomy for Hallux Rigidus: Comprehensive Surgical Guide
Key Takeaway
Cheilectomy is a joint-sparing surgical procedure indicated primarily for early to intermediate stages of hallux rigidus. The procedure involves the resection of dorsal osteophytes from the first metatarsal head and the base of the proximal phalanx, alongside the excision of the dorsal 25% to 35% of the metatarsal articular surface. This aims to decompress the joint, eliminate dorsal impingement, and restore pain-free dorsiflexion while preserving the intrinsic biomechanics of the first ray.
Introduction to Cheilectomy and Hallux Rigidus
Hallux rigidus is the most common osteoarthritic condition of the foot, characterized by degenerative arthritis of the first metatarsophalangeal (MTP) joint. The condition manifests clinically as pain, restricted dorsiflexion, and the formation of prominent dorsal osteophytes. The term "cheilectomy" is derived from the Greek word cheilos (meaning lip) and ectomy (meaning excision). It is a highly effective, joint-sparing surgical intervention designed to excise the dorsal osteophytic "lip" of the first metatarsal head and the base of the proximal phalanx, thereby decompressing the joint and restoring the functional arc of motion.
When conservative measures—such as rigid Morton's extensions, rocker-bottom shoes, NSAIDs, and intra-articular corticosteroid injections—fail to provide adequate relief, surgical intervention is warranted. Cheilectomy remains the gold standard for early to intermediate stages of hallux rigidus, offering high patient satisfaction rates, rapid recovery, and preservation of the first ray's weight-bearing biomechanics.
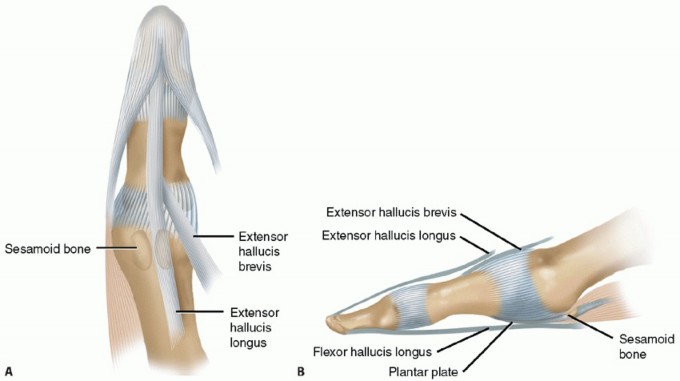
Biomechanics and Pathoanatomy
The first MTP joint is a complex hinge joint that plays a critical role in the terminal stance and pre-swing phases of the gait cycle. Normal gait requires approximately 65 to 75 degrees of passive dorsiflexion at the first MTP joint to engage the windlass mechanism, as described by Hicks.
In hallux rigidus, repetitive microtrauma or altered joint kinematics leads to cartilage degradation, primarily on the dorsal aspect of the metatarsal head. As the cartilage wears, reactive dorsal osteophytes form. These osteophytes act as a mechanical block to dorsiflexion, causing dorsal impingement.
Clinical Pearl: The pain associated with hallux rigidus is often twofold: deep articular pain from cartilage loss and superficial mechanical pain from the dorsal osteophyte impinging against the dorsal capsule and shoe wear. Furthermore, patients often supinate their foot to offload the first MTP joint, leading to lateral transfer metatarsalgia.
Indications and Patient Selection
Proper patient selection is paramount for a successful cheilectomy. The Coughlin and Shurnas clinical and radiographic classification system is the standard for guiding surgical decision-making:
- Grade 0: Stiffness, normal radiographs. (Treated conservatively).
- Grade I: Mild pain at extremes of motion, mild dorsal osteophyte, joint space preserved. (Excellent candidate for cheilectomy).
- Grade II: Moderate pain, moderate dorsal osteophyte, <50% joint space narrowing. (Excellent candidate for cheilectomy).
- Grade III: Significant pain, constant stiffness, >50% joint space narrowing, extensive osteophytes. (Controversial; cheilectomy may be combined with a Moberg osteotomy, though arthrodesis is often preferred).
- Grade IV: Pain throughout the entire range of motion, including mid-arc, with complete loss of joint space. (Contraindication for cheilectomy; arthrodesis is the procedure of choice).

Figure 1: Patient with stage II (radiographically) hallux rigidus; note the prominent dorsal osteophyte over the first metatarsal.
Surgical Technique: The Pfeffer Modification
The following step-by-step guide details the modified cheilectomy technique, emphasizing meticulous soft tissue handling, precise bone resection, and immediate postoperative mobilization.
1. Anesthesia and Positioning
The procedure is typically performed on an outpatient basis under a regional ankle block combined with monitored anesthesia care (MAC) or general anesthesia. The patient is placed in the supine position. A calf or ankle tourniquet is applied to ensure a bloodless surgical field.
2. Incision and Exposure
- Using a No. 15 blade, make a 5- to 6-cm dorsal longitudinal incision centered over the first MTP joint.
- The incision can be placed along either the medial or lateral border of the extensor hallucis longus (EHL) tendon, depending on surgeon preference and the location of the most prominent osteophytes.

Figure 2: Incision is placed at the border of the extensor hallucis longus.
- Blunt dissection is utilized in the subcutaneous tissues to identify and protect the dorsomedial and dorsolateral cutaneous sensory nerves (branches of the superficial peroneal nerve). Retraction of these nerves must be gentle to prevent postoperative neuromas.

Figure 3: The dorsal sensory nerve to the hallux is carefully isolated and protected.
3. Capsulotomy and Joint Inspection
- Divide the extensor hood approximately 2 mm medial to the border of the EHL. It is critical to keep the EHL tendon within its sheath to minimize the risk of postoperative adhesions, which can severely limit active dorsiflexion.
- Retract the EHL tendon laterally.
- Carefully dissect the joint capsule longitudinally to expose the medial, dorsal, and lateral aspects of the metatarsal head and the base of the proximal phalanx.
- Perform a complete synovectomy. Inspect the joint for cartilaginous loose bodies, which are frequently present in the medial or lateral gutters, and remove them.
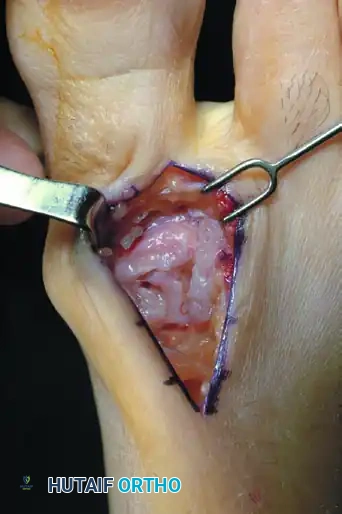
Figure 4: The first metatarsophalangeal joint is fully exposed, revealing the degenerative changes.
4. Osteophyte Excision
- Plantarflex the toe at the MTP joint to approximately 45 degrees to fully inspect the metatarsal head. Further subperiosteal dissection of the capsule may be necessary to gain adequate exposure of the medial and lateral gutters.
- The large dorsal ridge of bone and the predominant lateral/medial osteophytes will be readily apparent.
- Using a rongeur or a microsagittal saw, excise the dorsal, medial, and lateral osteophytes flush with the metatarsal shaft.
- If a prominent dorsal ridge of bone is present at the base of the proximal phalanx, remove it meticulously with a needle-nosed rongeur.

Figure 5: Dorsal osteophytes are removed from the metatarsal head and the base of the proximal phalanx. The dorsolateral osteophyte must also be addressed.
5. Metatarsal Head Resection
The most critical step of the cheilectomy is the resection of the dorsal articular surface of the metatarsal head.
- Excise the dorsal bony prominence along with 25% to 35% of the metatarsal head. The exact amount of bone excised depends on the degree of dorsal cartilage destruction and the volume of bone removal required to allow unimpeded passive dorsiflexion.
- The Cut: Use a small power saw or a 6-mm osteotome. A small amount of continuous saline irrigation should be used with the saw to avoid thermal necrosis of the remaining viable articular cartilage.
- Slope the line of resection upward from distal to proximal, extending from just dorsal to the edge of the viable cartilage to the dorsal prominence of the metatarsal neck.
- When removing 25% or more of the head, making the cut from proximal to distal is often easier. If less bone is being removed, a distal-to-proximal cut allows for better parallel alignment with the metatarsal shaft.
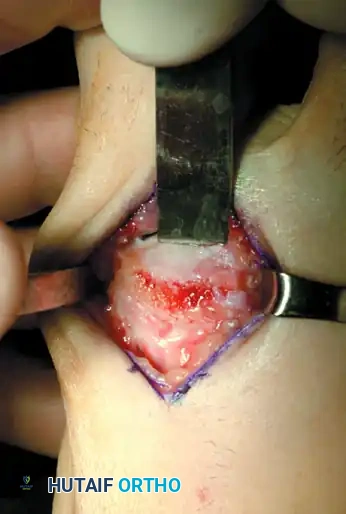
Figure 6: Twenty to 25 percent of the metatarsal head is removed dorsally to decompress the joint.
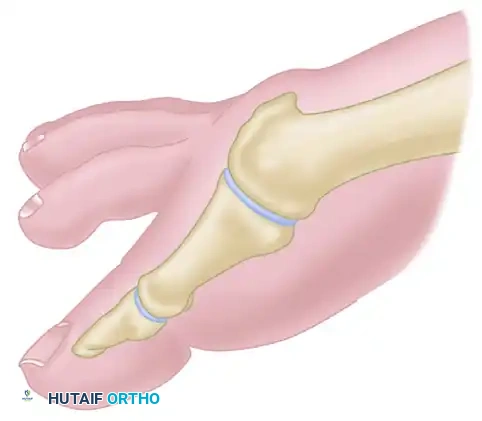
Figure 7: Pfeffer cheilectomy line of resection. Note the sloped trajectory from distal to proximal, ensuring removal of the dorsal impingement.
6. Joint Debridement and Microfracture
- After the primary bony cuts have been made, use a rongeur or a micro-reciprocating rasp to smooth any sharp borders left by the saw.
- Carefully trim any small irregularities along the remaining cartilage using a No. 15 blade.
- Microfracture: Drill any exposed subchondral bone that remains on the weight-bearing surface of the metatarsal head several times with a small Kirschner wire (K-wire). This induces bleeding and stimulates the formation of a fibrocartilage cap.
Surgical Warning: Do not resect excessive bone in the sagittal plane unless there is severe loss of medial or lateral cartilage. Over-resection can destabilize the joint and compromise the intrinsic musculature.
7. Sesamoid Assessment and Range of Motion Check
- Examine the sesamoid-metatarsal complex. While degenerative changes here are rare in early hallux rigidus, adhesions are common.
- Pass a small Freer elevator along the plantar aspect of the metatarsal head to break up any capsulosesamoid adhesions. Mobilizing the capsulosesamoid apparatus usually yields a few extra degrees of crucial dorsiflexion.
- Distract the joint and move it through a passive range of motion. At this point, passive dorsiflexion to 60 to 70 degrees must be possible. If this is not achieved, re-examine the joint to determine if further dorsal bony resection or plantar release is required.
- Palpate through the skin to ensure no abnormal bony prominences remain that could cause shoe-wear irritation.
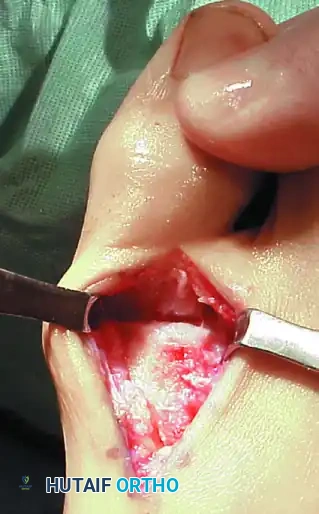
Figure 8: The joint is distracted, loose cartilage is removed, and the joint is moved through 60 to 70 degrees of motion to confirm adequate decompression.
8. Hemostasis and Closure
- Irrigate the joint copiously with sterile saline or an antibiotic solution.
- Optional Pearl: Apply bone wax to the raw bone surfaces to decrease postoperative bleeding and hematoma formation (ensure the patient is not allergic to bee venom prior to application).
- Deflate the tourniquet and obtain meticulous hemostasis with compression and electrocautery. Hematoma prevention is vital to minimize postoperative fibrosis.
- Close the joint capsule beneath the extensor tendon using two or three 4-0 absorbable sutures. Realign and repair the extensor mechanism, sewing into the medial border of the EHL sheath.
- Close the skin in a single layer using interrupted 4-0 horizontal nylon mattress sutures. Subcutaneous sutures are generally not required and can increase the risk of wound complications in this thin-skinned area.
- Apply a tight, well-padded compression dressing.
Postoperative Care and Rehabilitation
The success of a cheilectomy relies heavily on the patient's adherence to the postoperative rehabilitation protocol, specifically the early initiation of motion.
Phase 1: Immediate Postoperative (Days 0-14)
- 0 to 18 Hours: The initial bulky compression dressing remains in place. Elevation is strictly enforced to control edema.
- Day 1 to 3: The bulky dressing is removed and replaced with a smaller, snug dressing. Patients are allowed to bear weight on the heel and the lateral aspect of the foot as tolerated in a rigid, wooden-soled postoperative shoe. Crutches are provided for comfort but are discontinued as soon as possible.
- Day 10 to 14: Sutures are removed once the wound is fully healed. The patient is transitioned to a flexible-soled sneaker.
Phase 2: Range of Motion and Strengthening (Weeks 2-6)
- Active and Passive ROM: Gentle, active, and passive range-of-motion exercises are initiated immediately after suture removal. Patients are instructed to manually dorsiflex and plantarflex the hallux multiple times a day.
- Physical Therapy: Formal physical therapy may be prescribed if the patient is hesitant to mobilize the joint. Aggressive scar massage is encouraged to prevent capsular contracture.
Radiographic Follow-up
Immediate postoperative radiographs are obtained to confirm the adequacy of the resection and establish a baseline.



Figures 9-11: Immediate postoperative AP, Lateral, and Oblique radiographs demonstrating adequate dorsal metatarsal head resection and joint decompression.
Complications and Pitfalls
While cheilectomy is generally a safe and highly successful procedure, complications can occur:
- Inadequate Resection: Failure to remove enough of the dorsal metatarsal head (less than 25%) or failure to slope the cut proximally will result in persistent dorsal impingement and limited dorsiflexion.
- Nerve Injury: Iatrogenic injury or entrapment of the dorsomedial or dorsolateral cutaneous nerves can lead to painful neuromas or numbness over the hallux.
- EHL Adhesions: Failure to preserve the EHL sheath or excessive handling of the tendon can result in severe scarring, limiting active dorsiflexion despite adequate bone removal.
- Progression of Osteoarthritis: Cheilectomy does not halt the underlying degenerative process. Patients must be counseled that while the procedure provides excellent medium-to-long-term relief, progression to end-stage hallux rigidus requiring arthrodesis may eventually occur.
Long-Term Outcomes
Clinical evidence demonstrates that cheilectomy provides excellent pain relief and functional improvement in over 85% of appropriately selected patients. The restoration of the windlass mechanism allows patients to return to normal gait patterns and high-impact activities. Long-term radiographic follow-up often shows maintenance of the joint space and a lack of recurrent dorsal osteophyte formation when the initial resection is adequate.


Figures 12-13: One year postoperative AP and Lateral radiographs demonstrating maintenance of the joint space, absence of recurrent osteophytes, and excellent preservation of the first ray architecture.
By adhering to meticulous surgical principles—adequate exposure, precise bone resection, protection of soft tissue envelopes, and aggressive postoperative mobilization—the orthopedic surgeon can reliably achieve excellent outcomes in the management of hallux rigidus via cheilectomy.
📚 Medical References
- of the hip in children, J Surg Orthop Adv 13:20, 2004.
- Erken EHW, Katz K: Irritable hip and Perthes’ disease, J Pediatr Orthop 10:322, 1990.
- Erkula G, Bursali A, Okan E: False profi le radiography for the evaluation of Legg-Calvé-Perthes disease, J Pediatr Orthop 13B:238, 2004.
- Evans IK, Deluca PA, Gage JR: A comparative study of ambulation-abduction bracing and varus derotation osteotomy in the treatment of severe Legg-Calvé-Perthes disease in children over 6 years of age, J Pediatr Orthop 8:676, 1988.
- Farsetti P, Tudisco C, Caterini R, et al: The Herring lateral pillar classifi cation for prognosis in Perthes disease: late results in 49 patients treated conservatively, J Bone Joint Surg 77B:739, 1995.
- Flashman FL, Ghormley RK: Osteochondritis dissecans of the head of the femur, West J Surg 57:221, 1949.
- Fulford GE, Lunn PG, Macnicol MF: A prospective study of nonoperative and operative management for Perthes’ disease, J Pediatr Orthop 13:281, 1993.
- Futami T, Kasahara Y, Suzuki S, et al: Ultrasonography in transient synovitis and early Perthes’ disease, J Bone Joint Surg 73B:635, 1991.
- Gallistl S, Reitinger T, Linhart W, et al: The role of inherited thrombotic disorders in the etiology of Legg-Calvé-Perthes disease, J Pediatr Orthop 19:82, 1999.
- Garceau GJ: Surgical treatment of coxa plana, J Bone Joint Surg 46B:779, 1964.
- Gaughan DM, Mofenson LM, Hughes MD, et al:
You Might Also Like