Management of Pelvic Ring and Sternoclavicular Joint Dislocations
Key Takeaway
Traumatic dislocations of the pubic symphysis, sacroiliac, and sternoclavicular joints represent severe, high-energy injuries requiring meticulous orthopedic management. While anterior sternoclavicular dislocations are often managed nonoperatively, posterior dislocations are true emergencies due to mediastinal compression risks. Pelvic ring disruptions demand precise restoration of the complex ligamentous anatomy to ensure biomechanical stability. This guide details evidence-based surgical indications, operative approaches, and complication management for these critical joint injuries.
PUBIC SYMPHYSIS AND SACROILIAC JOINTS
Dislocations involving the symphysis pubis and sacroiliac (SI) joints occur almost exclusively in the setting of high-energy trauma, such as motor vehicle collisions, crush injuries, or falls from significant heights. The adult pelvis is a highly stable osseoligamentous ring; therefore, considerable force is required to overcome the complex ligamentous structures that provide its inherent stability.
Biomechanics and Pathoanatomy
The stability of the pelvic ring relies on a robust posterior tension band and an anterior strut.
* Posterior Complex: The sacroiliac joints are stabilized by the interosseous sacroiliac ligaments (the strongest ligaments in the body), the anterior and posterior sacroiliac ligaments, and the accessory pelvic ligaments (sacrotuberous and sacrospinous). Disruption of this posterior complex leads to profound vertical and rotational instability.
* Anterior Complex: The pubic symphysis acts as a secondary stabilizer, resisting external rotation forces. It is supported by the superior and arcuate pubic ligaments, as well as the interlacing fibers of the rectus abdominis and external oblique aponeuroses.
Surgical Indications and Decision Making
The primary goal in managing pelvic ring disruptions is the restoration of mechanical stability and anatomical alignment to facilitate early mobilization and minimize long-term disability.
Indications for operative intervention include:
1. Symphyseal Diastasis: Greater than 2.5 cm, indicative of anterior tension band failure and often associated with rotational instability (e.g., APC-II or APC-III injuries).
2. Sacroiliac Joint Dislocation: Any significant displacement (>1 cm), vertical shear injuries, or highly unstable crescent fractures.
3. Hemodynamic Instability: Requiring emergent pelvic packing, external fixation, or angiographic embolization prior to definitive internal fixation.
Operative Approach: Pubic Symphysis Plating
SURGICAL PEARL: Always ensure a Foley catheter is placed prior to the procedure to decompress the bladder and assist in identifying the urethra, which is highly susceptible to injury in anterior pelvic ring disruptions.
- Positioning: The patient is placed supine on a radiolucent table. The entire abdomen to the mid-thighs is prepped and draped.
- Incision: A Pfannenstiel incision is made 2 fingerbreadths superior to the pubic symphysis.
- Dissection: The anterior rectus sheath is incised transversely. The rectus abdominis muscles are split vertically along the linea alba. Care is taken to protect the spermatic cord or round ligament.
- Exposure: The retropubic space of Retzius is developed bluntly. The superior pubic rami and the disrupted symphysis are exposed.
- Reduction: Pointed Weber reduction clamps are placed on the superior pubic rami. Alternatively, a Jungbluth clamp can be utilized via pre-drilled 3.5mm holes to compress the symphysis.
- Fixation: A multi-hole (usually 4 to 6 holes) 3.5mm or 4.5mm reconstruction plate or specialized symphyseal plate is contoured to the superior aspect of the pubic ring. Fully threaded cortical screws are placed to secure the construct.
ASSOCIATED HIGH-ENERGY TRAUMA: HIP DISLOCATIONS
High-energy axial loading that causes pelvic ring disruptions frequently results in concomitant injuries to the appendicular skeleton, most notably traumatic hip dislocations. Posterior dislocations of the hip are orthopedic emergencies requiring immediate closed reduction to mitigate the risk of devastating complications.
Complications of Hip Dislocation: Osteonecrosis
The vascular supply to the femoral head (primarily the medial femoral circumflex artery) is highly vulnerable during a posterior dislocation. Delay in reduction beyond 6 hours exponentially increases the risk of osteonecrosis (avascular necrosis) of the femoral head.
CLINICAL PITFALL: Even with prompt and concentric closed reduction, patients remain at risk for late-onset osteonecrosis and post-traumatic osteoarthritis due to the initial mechanical insult to the chondrocytes and transient ischemia.
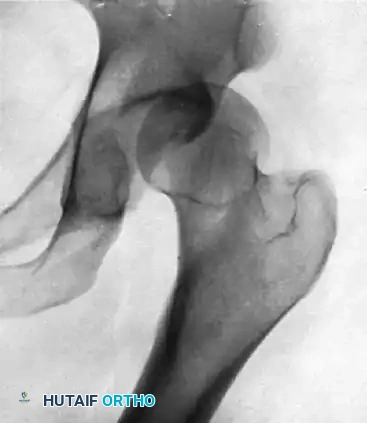
Below is a classic radiographic progression demonstrating the severe sequelae of a posterior hip dislocation:
FIGURE A: Initial anteroposterior radiograph demonstrating a posterior dislocation of the hip. Note the superior and lateral displacement of the femoral head relative to the acetabulum.

FIGURE B: Radiograph taken 8 months after successful closed reduction. The image reveals advanced osteonecrosis of the femoral head. Note the profound subchondral sclerosis, narrowed joint space, and early structural collapse of the femoral head.
STERNOCLAVICULAR JOINT DISLOCATIONS
The sternoclavicular (SC) joint is the sole true synovial articulation connecting the appendicular skeleton of the upper extremity to the axial skeleton. It is a diarthrodial, saddle-shaped joint containing an intra-articular fibrocartilaginous disc. Stability is conferred almost entirely by its ligamentous envelope, primarily the costoclavicular (rhomboid) ligament, the interclavicular ligament, and the anterior/posterior sternoclavicular capsular ligaments.
Traumatic dislocation of the sternoclavicular joint usually results from an indirect force transmitted through the anterior shoulder with the arm abducted. The sternoclavicular joint can also be dislocated congenitally, or as a result of developmental, degenerative, and inflammatory processes.
Anterior Sternoclavicular Dislocations
The most frequent of these injuries is the anterior dislocation, in which the medial end of the clavicle is displaced anteriorly and superiorly relative to the sternum.
Clinical Presentation
When traumatic dislocation is anterior, patients present with considerable pain, localized swelling, and a prominent, palpable deformity over the dislocated joint. The anteriorly displaced clavicle may appear elevated in relation to the sternum or may remain depressed near the first rib, depending on the exact vector of the force and the extent of ligamentous disruption.
Management Strategy
Acute anterior dislocations usually can be treated by nonoperative methods. Closed reduction can be attempted under conscious sedation by placing a bolster between the scapulae and applying posterior pressure to the medial clavicle while extending and abducting the arm.
However, interposition of the joint capsule or the intra-articular disc may cause the dislocation to be irreducible. If the joint remains dislocated, the medial end of the clavicle causes an unsightly cosmetic prominence, but for sedentary patients, little functional disability is to be expected. Surgical intervention for anterior dislocations is rarely indicated and is generally reserved for highly symptomatic, chronic, unreduced, or recurrent dislocations in high-demand athletes.
Posterior Sternoclavicular Dislocations: A True Emergency
Posterior (retrosternal) dislocation of the sternoclavicular joint is far less common but represents a true orthopedic emergency. It is a much more serious injury than the anterior dislocation because the critical anatomic structures residing in the superior mediastinum may be compressed or lacerated by the posteriorly displaced medial end of the clavicle.
Mediastinal Anatomy and Associated Risks
The structures immediately posterior to the SC joint include:
* The trachea and esophagus.
* The thoracic duct.
* The great vessels: Innominate artery, internal jugular vein, subclavian vein, aorta, and pulmonary artery.
* The superior aspect of the heart.
* The brachial plexus.
The posteriorly displaced medial end of the clavicle can produce a constellation of life-threatening symptoms, including respiratory distress (stridor, dyspnea), venous congestion, arterial insufficiency (diminished distal pulses), brachial plexus compression (paresthesias), and myocardial conduction abnormalities. Occasionally, direct pressure on these structures makes the dislocation a life-threatening crisis requiring immediate intervention.
Surgical Management of the Sternoclavicular Joint
Surgical treatment should be strictly reserved for irreducible posterior sternoclavicular dislocations, or for significantly symptomatic, old, unreduced, or recurrent anterior sternoclavicular dislocations.
SURGICAL WARNING: THE DANGER OF HARDWARE MIGRATION
Historically, smooth K-wires or Steinmann pins were used to stabilize the SC joint. This practice is now universally condemned. Occasionally, a whole pin migrates, or the pin breaks, and parts of it may migrate directly into the heart, pulmonary artery, innominate artery, or aorta. Reports suggest that the incidence of significant, life-threatening complications approaches 25% when pins are used in sternoclavicular procedures. Never use unthreaded pins or wires across the sternoclavicular joint.
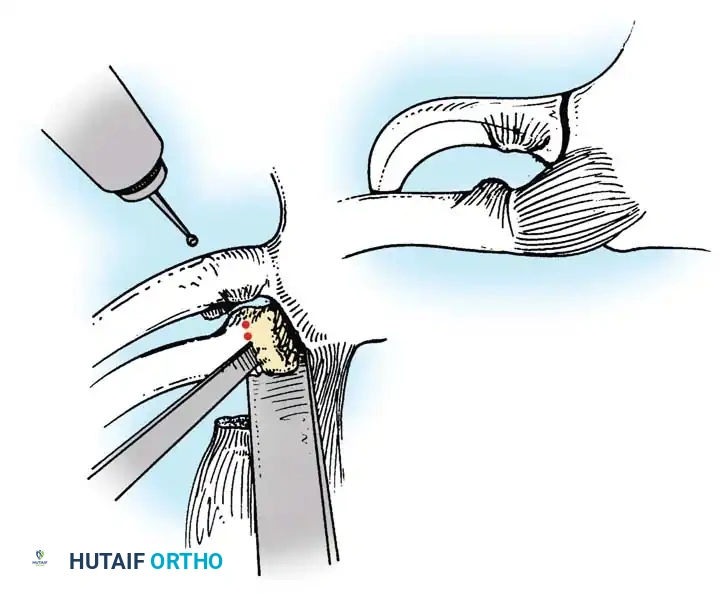
Operative Technique: Suture Stabilization and Graft Reconstruction
For unstable reductions or irreducible posterior dislocations, modern techniques rely on robust soft-tissue reconstruction rather than rigid metallic fixation. Waters et al. advocated for suture stabilization of the costoclavicular and sternoclavicular ligaments, which has become the gold standard.
- Preparation: The patient is placed in a beach-chair or supine position with a bump between the scapulae. A cardiothoracic surgeon must be available on standby when operating on a posterior SC joint dislocation due to the risk of catastrophic hemorrhage upon reduction.
- Incision: A transverse incision is made centered over the medial clavicle, extending medially over the manubrium.
- Dissection: The platysma is incised, and the periosteum of the medial clavicle and manubrium is exposed. Care is taken to preserve the anterior capsule if it is intact (though it is usually torn).
- Reduction: For posterior dislocations, a towel clip is placed around the medial clavicle to apply anterior and lateral traction. A blunt periosteal elevator can be carefully inserted behind the clavicle to lever it anteriorly.
- Reconstruction (Figure-of-Eight Technique):
- Drill holes are carefully created in the medial clavicle and the manubrium. A drill guide and retractor must be placed posterior to the bone to protect the mediastinum.
- Heavy, non-absorbable tape (e.g., FiberWire) or a tendon autograft/allograft (such as a semitendinosus or gracilis graft) is passed through the drill holes in a figure-of-eight fashion.
- The graft or suture is tensioned and tied with the joint held in anatomic reduction.
- Capsular Repair: The remaining anterior capsule and the sternal head of the sternocleidomastoid muscle are meticulously repaired over the construct to provide additional dynamic stability.
Postoperative Protocol
Following SC joint reconstruction, the patient is placed in a sling or figure-of-eight harness for 4 to 6 weeks.
* Weeks 0-4: Absolute immobilization. Pendulum exercises may be permitted depending on the security of the fixation, but active elevation and abduction are strictly prohibited.
* Weeks 4-8: Gradual introduction of active-assisted range of motion, limiting forward elevation to 90 degrees.
* Weeks 8-12: Progression to full active range of motion and initiation of periscapular and rotator cuff strengthening.
* Months 4-6: Return to heavy lifting or contact sports is generally restricted until at least 6 months postoperatively, contingent upon clinical stability and radiographic healing.
You Might Also Like