Elbow LCL Reconstruction: Master Stability with Extensor Carpi Ulnaris

Key Takeaway
This article provides essential research regarding Elbow LCL Reconstruction: Master Stability with Extensor Carpi Ulnaris. Lateral Collateral Ligament (LCL) injuries frequently result from significant elbow trauma, such as dislocation, or ligament attenuation. Comprising four main components, including the radial ulnohumeral ligament, the LCL stabilizes the elbow. Injury can lead to posterolateral rotatory instability. Extensor muscle groups, such as the extensor carpi ulnaris, function as dynamic stabilizers, originating deep to the extensor muscle mass.
Introduction and Epidemiology
Lateral collateral ligament (LCL) injuries of the elbow represent a critical disruption of the primary restraint to posterolateral rotatory instability (PLRI). These injuries most frequently occur following significant elbow trauma, with elbow dislocation being the most common inciting event. According to the O'Driscoll classification of elbow instability, the LCL complex is the first structure to fail in a typical traumatic mechanism, initiating a cascade of capsuloligamentous disruption that progresses from lateral to medial.
Beyond acute trauma, attenuation of the LCL complex is increasingly recognized as an iatrogenic complication. Multiple surgical interventions to the lateral compartment of the elbow, particularly aggressive releases for lateral epicondylitis, can compromise the integrity of the ligamentous origin. Furthermore, the administration of local corticosteroid injections has been implicated in ligamentous degradation. Recent literature demonstrates that even a single corticosteroid injection can result in lower complete recovery rates and higher recurrence rates of lateral-sided elbow pathology at one year, predisposing the patient to microtraumatic LCL failure.

Chronic LCL attenuation is also a well-documented phenomenon in patients with residual cubitus varus deformity following the malunion of supracondylar humerus fractures. In these cases, the altered mechanical axis subjects the lateral ligamentous complex to chronic tensile overload, ultimately leading to tardy PLRI. Understanding the diverse epidemiological factors—from acute high-energy dislocations to chronic insidious attenuation—is essential for the orthopedic surgeon evaluating lateral elbow pain and mechanical symptoms.

Surgical Anatomy and Biomechanics
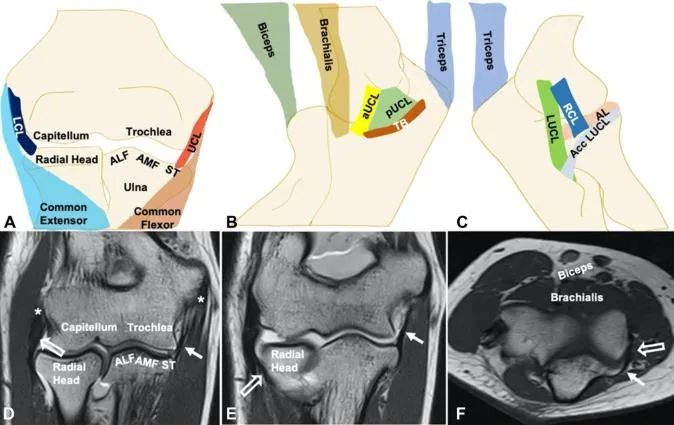
The LCL complex is a sophisticated capsuloligamentous network comprising four major components: the lateral ulnar collateral ligament (LUCL), also referred to as the radial ulnohumeral ligament (RUHL); the radial collateral ligament (RCL) proper; the annular ligament; and the accessory collateral ligament.

The ligamentous complex originates from a broad, fan-shaped footprint over the lateral epicondyle. This origin lies deep to the common extensor muscle mass. The isometric point of the LCL complex on the humerus is located at the center of the capitellum, serving as the axis of rotation for the ulnohumeral joint. Distally, the complex separates into more discrete functional structures.

The Lateral Ulnar Collateral Ligament
The LUCL (or RUHL) is the primary static stabilizer against varus and external rotatory stress, making it the most critical structure in preventing PLRI. It traverses posterodistally to attach to the supinator crest of the ulna. The supinator tubercle, a key osseous landmark for ulnar tunnel placement during reconstruction, resides approximately 15 mm distal to the proximal border of the proximal radioulnar joint (PRUJ).

The Radial Collateral and Annular Ligaments
The RCL proper is positioned more anteriorly and blends intimately with the annular ligament. Its primary biomechanical role is to resist varus stress. The annular ligament sweeps around the radial head and neck, inserting on the anterior and posterior margins of the lesser sigmoid notch, thereby stabilizing the PRUJ. The accessory collateral ligament provides supplementary stabilization to the annular ligament during varus stress.

Dynamic Stabilizers and Neurologic Considerations
The joint capsule acts as a secondary static stabilizer, particularly the anterior band during elbow extension. Dynamically, the anconeus, extensor carpi ulnaris (ECU), and the common extensor muscle group provide active compressive forces across the radiocapitellar joint.

Surgical exposure of the lateral elbow requires a precise understanding of the posterior interosseous nerve (PIN). The PIN courses through the supinator muscle and is highly vulnerable during lateral approaches. On average, the PIN crosses the midpoint of the radius 33.4 ± 5.7 mm distal to the radiocapitellar joint with the forearm in supination. This safe zone increases significantly to 52.0 ± 7.8 mm when the forearm is placed in full pronation. Therefore, pronation is a mandatory maneuver during deep dissection to protect the nerve.

Pathogenesis of Posterolateral Rotatory Instability
Injury to the LUCL initiates PLRI. When the forearm is supinated and slightly flexed, a valgus stress applied to an elbow with an incompetent LCL complex causes the ulnohumeral joint to externally rotate. This rotation compresses the radiocapitellar joint and ultimately forces the radial head to subluxate or dislocate posteriorly relative to the capitellum.

Indications and Contraindications
The diagnosis of PLRI relies heavily on a thorough history and a nuanced physical examination. Patients typically present with mechanical symptoms such as clicking, popping, or a sensation of the elbow slipping during extension and supination. These symptoms are often exacerbated by activities that load the joint in this position, such as pushing up from a chair or performing push-ups.

Physical examination tests, including the lateral pivot-shift test, the posterolateral rotatory apprehension test, the chair sign, and the push-up sign, are diagnostic. However, due to patient guarding, these provocative maneuvers are often best elicited under anesthesia or confirmed with fluoroscopic stress views.

Reconstruction of the LCL is indicated when non-operative measures fail or when gross instability significantly impairs upper extremity function. The utilization of an ECU autograft is particularly advantageous as it utilizes a local dynamic stabilizer, avoiding the donor site morbidity associated with distant grafts like the palmaris longus or gracilis.

| Parameter | Operative Indications | Non-Operative Indications |
|---|---|---|
| Clinical Presentation | Chronic symptomatic PLRI failing conservative care | First-time acute dislocation (stable after reduction) |
| Mechanical Symptoms | Recurrent locking, catching, or giving way | Mild, infrequent symptoms manageable with bracing |
| Functional Demand | High-demand athletes, manual laborers | Low-demand or elderly patients |
| Associated Injuries | Concomitant radial head or coronoid fractures (Terrible Triad) | Isolated LCL sprain without gross instability |
| Imaging | Complete LCL avulsion with persistent subluxation | Partial interstitial tearing with a concentrically reduced joint |
Contraindications to surgical reconstruction include active local or systemic infection, severe degenerative joint disease of the ulnohumeral or radiocapitellar joints (which may necessitate arthroplasty rather than ligament reconstruction), and medical comorbidities precluding anesthesia.

Pre Operative Planning and Patient Positioning
Thorough preoperative planning involves advanced imaging, typically an MRI or MR arthrogram, to assess the quality of the residual LCL tissue, the presence of chondral damage, and the integrity of the common extensor origin. If an ECU autograft is planned, the surgeon must clinically verify the presence and function of the ECU muscle belly and tendon.

Patient Positioning and Operating Room Setup
The patient is typically positioned supine on the operating table. A non-sterile tourniquet is applied high on the brachium. The arm can be positioned on a standard hand table; however, many surgeons prefer placing the arm across the patient's chest. This cross-chest position allows for excellent access to the lateral aspect of the elbow and facilitates natural pronation of the forearm, which drops the PIN away from the surgical field.

Alternatively, the lateral decubitus position with the arm draped over a post can be utilized, providing unobstructed access to both the medial and lateral compartments if a combined procedure is anticipated. Fluoroscopy must be readily available and positioned to allow for orthogonal views of the elbow without compromising the sterile field.

Detailed Surgical Approach and Technique
Reconstruction of the LCL using a split ECU autograft requires meticulous dissection, precise tunnel placement, and rigid fixation. The ECU graft provides excellent tensile strength and is conveniently located within the primary surgical incision.

Surgical Approach and Exposure
A longitudinal incision is made over the lateral epicondyle, extending distally toward the supinator crest of the ulna. Subcutaneous flaps are elevated to expose the deep fascia. The standard Kocher approach is utilized, exploiting the internervous plane between the anconeus (innervated by the radial nerve) and the ECU (innervated by the posterior interosseous nerve).

The deep fascia is incised, and the interval is developed. The anconeus is retracted posteriorly, and the ECU is retracted anteriorly. It is imperative to maintain the forearm in full pronation during this deep dissection to maximize the distance of the PIN from the surgical field. The joint capsule is exposed, and a longitudinal capsulotomy is performed slightly anterior to the LUCL footprint to allow for inspection of the radiocapitellar joint and to confirm the diagnosis of instability.

Graft Harvest Extensor Carpi Ulnaris
The ECU tendon is identified within the anterior flap of the exposure. The tendon is traced as far distally as the incision allows. A longitudinal split is created in the ECU tendon, harvesting approximately 50% of its width.

The split graft is released distally and dissected proximally toward its musculotendinous junction. The proximal attachment can be left intact if a pedicled technique is desired, but a free graft is generally preferred to allow for optimal tensioning and passage through the osseous tunnels. The harvested strip is typically 10 to 12 cm in length. The ends of the free graft are whipstitched with high-tensile, non-absorbable sutures (e.g., #2 FiberWire or similar).

Preparation of Isometric Footprints
Accurate tunnel placement is the most critical step in LCL reconstruction. Non-isometric tunnel placement will lead to graft stretching, recurrent instability, or severe loss of elbow motion.

Ulnar Tunnels: The anatomic insertion of the LUCL is on the supinator crest of the ulna. Two converging drill holes (typically 3.2 mm or 3.5 mm) are created. The first hole is placed at the supinator tubercle, and the second is placed approximately 1.5 cm proximal to the first, along the crest. These holes are connected using a curved curette or a specialized tunnel-connecting tool to create a bone bridge of at least 1 cm to prevent fracture during graft tensioning.

Humeral Tunnel: The isometric origin on the humerus is located at the center of the capitellum, slightly anterior and inferior to the apex of the lateral epicondyle. A guide pin is placed at this isometric point. Isometry can be verified by looping a suture around the pin and the ulnar bone bridge and taking the elbow through a full range of motion; the suture should not excursion more than 1-2 mm.

Once isometry is confirmed, a blind-ended tunnel is drilled over the guide pin to a depth of approximately 15 to 20 mm, depending on the chosen fixation method (e.g., interference screw or docking technique). For a docking technique, two smaller exit holes are drilled superiorly to allow for suture passage.

Graft Passage and Fixation
The prepared ECU graft is first passed through the ulnar bone tunnel. The two limbs of the graft are then routed proximally toward the humeral tunnel.

If utilizing the docking technique, the whipstitched sutures of both graft limbs are passed into the main humeral tunnel and out through the smaller superior exit holes.

Tensioning the graft is a critical maneuver. The elbow is positioned in 30 to 40 degrees of flexion, and the forearm is placed in maximal pronation. This position closes the radiocapitellar joint and reduces the posterolateral subluxation. A mild valgus force is applied to ensure the medial joint space is not over-constrained.

While holding the joint in this reduced position, the sutures are tied securely over the humeral bone bridge. Alternatively, an interference screw can be utilized in the main humeral tunnel to secure the graft limbs directly against the bone, providing immediate rigid fixation.

Following fixation, the elbow is taken through a gentle range of motion to confirm stability and assess for any impingement or loss of extension. The extensor origin and fascia are meticulously repaired over the graft to provide additional dynamic stability.

Complications and Management
Despite meticulous surgical technique, LCL reconstruction carries a risk of complications. Surgeons must be prepared to identify and manage these issues promptly.

| Complication | Estimated Incidence | Etiology and Risk Factors | Management and Salvage Strategies |
|---|---|---|---|
| Recurrent Instability | 5 - 10% | Non-isometric tunnel placement, premature return to activity, graft failure | Revision reconstruction, potential use of allograft, evaluation for underlying osseous deformity (e.g., cubitus varus correction). |
| Elbow Stiffness | 10 - 15% | Over-tensioning of the graft, prolonged immobilization, heterotopic ossification | Aggressive physical therapy, static progressive splinting. Arthroscopic or open capsular release if refractory after 6 months. |
| PIN Neuropathy | 2 - 5% | Retraction injury, failure to pronate forearm during exposure, aberrant anatomy | Observation for neuropraxia (usually resolves in 3-6 months). EMG/NCS at 6 weeks if no improvement. Surgical exploration if complete transection suspected. |
| Ulnar Bone Bridge Fracture | 1 - 3% | Inadequate distance between drill holes (<1 cm), overly aggressive tensioning | Use of suture anchors for distal fixation instead of transosseous tunnels, or extending the tunnel further distally. |
| Infection | 1 - 2% | Standard surgical risks, poor soft tissue envelope | Intravenous antibiotics, surgical debridement. Retention of graft if possible, but removal may be necessary in deep, recalcitrant infections. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation protocol is designed to protect the healing graft while preventing debilitating elbow stiffness.
Immediately following surgery, the elbow is immobilized in a posterior splint at 90 degrees of flexion with the forearm in full pronation. Pronation is critical as it utilizes the intact medial collateral ligament to act as a hinge, compressing the lateral side of the joint and protecting the reconstructed LCL from tensile stress.

At 10 to 14 days postoperatively, the splint and sutures are removed. The patient is transitioned to a hinged elbow brace, locked in 90 degrees of flexion and pronation during rest. Active and active-assisted range of motion exercises are initiated. Extension is typically limited to 30 degrees for the first 4 weeks to prevent excessive stress on the graft. The "overhead protocol" is often utilized, where the patient performs active motion while lying supine with the shoulder flexed to 90 degrees; this position allows gravity to assist in maintaining ulnohumeral reduction.
Shoulder abduction combined with internal rotation must be strictly avoided, as this maneuver creates a significant varus moment at the elbow. Strengthening exercises for the dynamic stabilizers (ECU, anconeus, biceps, triceps) begin at 6 to 8 weeks. Unrestricted range of motion is generally permitted by 8 weeks, but heavy lifting and return to contact sports are restricted until 4 to 6 months postoperatively, contingent upon the return of normal strength and the absence of mechanical symptoms.
Summary of Key Literature and Guidelines
The understanding and management of PLRI have evolved significantly over the past three decades. O'Driscoll et al. provided the foundational biomechanical and clinical descriptions of PLRI, establishing the LUCL as the primary restraint to posterolateral rotatory forces. Their seminal work delineated the stages of elbow instability, shifting the paradigm of how traumatic elbow dislocations are managed.
Subsequent biomechanical studies have validated the use of various grafts for reconstruction. Research comparing palmaris longus, triceps fascia, and ECU grafts has demonstrated that the split ECU autograft provides superior or equivalent load-to-failure characteristics while minimizing donor site morbidity. The local proximity of the ECU allows for a single-incision procedure, reducing operative time and surgical trauma.
Clinical outcomes following LCL reconstruction with ECU autograft show high rates of patient satisfaction, return to pre-injury activity levels, and restoration of objective stability. Sanchez-Sotelo and colleagues have published extensively on the docking technique, highlighting its biomechanical superiority in achieving rigid fixation and allowing for precise tensioning of the graft limbs. Current academic guidelines emphasize the necessity of anatomic, isometric tunnel placement over the specific choice of graft material, reinforcing that technical precision is the primary determinant of successful clinical outcomes.
Clinical & Radiographic Imaging
You Might Also Like