Tibone and Bradley Technique: Advanced Posterior Capsular Shift for Shoulder Instability
Key Takeaway
The Tibone and Bradley technique is a highly effective posterior capsular shift procedure designed to address moderate posterior shoulder instability, particularly in athletic populations. By utilizing an interval split between the infraspinatus and teres minor, or a bipennate infraspinatus split, this approach preserves the posterior rotator cuff while allowing robust capsular imbrication. This results in a thickened posterior soft-tissue restraint, restoring glenohumeral stability without compromising dynamic muscle function.
Introduction to Posterior Shoulder Instability
Posterior shoulder instability represents a complex and often underdiagnosed clinical entity, comprising approximately 2% to 10% of all shoulder instability presentations. Unlike anterior instability, which frequently results from an acute traumatic dislocation, posterior instability often manifests as recurrent microtrauma, particularly in athletic populations such as weightlifters, throwers, and contact sports athletes. The pathology typically involves attenuation of the posterior capsulolabral complex, specifically the posterior band of the inferior glenohumeral ligament (IGHL) and the posterior capsule.
Historically, surgical management of posterior instability was fraught with high failure rates and complications, largely due to non-anatomic procedures or excessive tightening that restricted range of motion. The evolution of the posterior capsular shift, initially popularized by Neer and Foster, and later refined by Bigliani et al., marked a paradigm shift toward anatomic volume reduction of the redundant capsule.
The Tibone and Bradley Technique represents a highly sophisticated variation of the posterior capsular shift. By specifically targeting the interval between the infraspinatus and teres minor—or utilizing a muscle-splitting approach through the bipennate infraspinatus—this technique minimizes iatrogenic trauma to the posterior rotator cuff. The primary biomechanical advantage of this approach is that the imbrication of the posterior capsule on the glenoid side produces a significantly thicker, more robust posterior soft-tissue restraint, making it the preferred open technique for athletes with moderate posterior instability.
Surgical Anatomy and Biomechanics
A profound understanding of the posterior shoulder anatomy is mandatory to execute the Tibone and Bradley technique safely and effectively.
The Posterior Rotator Cuff Interval
The traditional approach to the posterior capsule involves navigating the posterior rotator cuff. Tibone and Bradley advocated for splitting the interval between the infraspinatus (innervated by the suprascapular nerve) and the teres minor (innervated by the axillary nerve). This internervous plane provides direct access to the posterior capsule while preserving the dynamic stabilizing function of the cuff.
Alternatively, Shaffer et al. described an infraspinatus muscle-splitting incision. The infraspinatus is a bipennate muscle supplied by two distinct branches of the suprascapular nerve. By carefully splitting the muscle between its two innervations, the surgeon can achieve excellent exposure of the middle portion of the posterior capsule without causing long-term denervation or functional deficit to the muscle.
The Capsulolabral Complex
The posterior capsule is inherently thinner than the anterior capsule. In patients with posterior instability, this tissue is often further attenuated, patulous, or stripped from the glenoid (reverse Bankart lesion). The goal of the capsular shift is to reduce capsular volume and recreate the posterior bumper.
Surgical Warning: The axillary nerve and posterior humeral circumflex artery exit the quadrangular space immediately inferior to the teres minor and lie in perilous proximity to the inferior capsule. Aggressive inferior dissection or blind placement of retractors at the 6 o'clock position can result in devastating iatrogenic axillary nerve injury.
Indications and Patient Selection
The Tibone and Bradley technique is not a panacea for all forms of shoulder instability. Meticulous patient selection is the cornerstone of surgical success.
Primary Indications
- Recurrent Posterior Subluxation: Particularly in athletes (e.g., offensive linemen, weightlifters) who have failed a minimum of 6 months of dedicated conservative management (periscapular and posterior deltoid strengthening).
- Moderate Posterior Instability: Patients demonstrating symptomatic posterior translation (Grade 2 or 3 on the posterior drawer test) with a competent anterior capsule.
- Failed Arthroscopic Stabilization: Cases where arthroscopic posterior labral repair or capsular plication has failed due to severe capsular redundancy or poor tissue quality.
Contraindications
- Voluntary Dislocators: Patients with underlying psychiatric conditions or those who utilize muscular substitution to voluntarily dislocate the shoulder are absolute contraindications for operative intervention.
- Significant Bony Defects: Patients with severe glenoid retroversion (greater than 15 degrees) or a large reverse Hill-Sachs lesion (engaging defect >20% of the articular surface) require bony augmentation (e.g., posterior bone block or McLaughlin procedure) rather than an isolated soft-tissue shift.
- Multidirectional Instability (MDI): If the primary component of instability is inferior, an isolated posterior shift will fail. A global capsular shift is required.
Preoperative Evaluation
Clinical Examination
The patient will typically present with pain localized to the posterior joint line, exacerbated by the provocative position of flexion, adduction, and internal rotation. Key clinical tests include:
* Jerk Test: A sudden "clunk" as the humeral head subluxates posteriorly when the arm is axially loaded in 90 degrees of flexion and internal rotation.
* Kim Test: Evaluates for a posteroinferior labral tear.
* Load and Shift Test: Quantifies the degree of posterior translation.
Imaging Protocol
- Standard Radiographs: True AP (Grashey), axillary lateral, and Stryker notch views to assess for glenoid hypoplasia, retroversion, and reverse Hill-Sachs lesions.
- MRI Arthrogram: The gold standard for evaluating the posterior labrum, capsular volume, and the integrity of the rotator cuff. It accurately delineates paralabral cysts and reverse Bankart lesions.
- CT Scan: Recommended if significant glenoid bone loss or excessive retroversion is suspected.
Surgical Technique: Step-by-Step Guide
The Tibone and Bradley technique demands meticulous soft-tissue handling and precise spatial awareness. The following steps outline the procedure in exhaustive detail.
1. Anesthesia and Positioning
- Anesthesia: A combination of general endotracheal anesthesia and an interscalene regional block is preferred to ensure complete muscle relaxation and optimal postoperative pain control.
- Positioning: Place the patient in the lateral decubitus position on a beanbag. Ensure all bony prominences (peroneal nerve, greater trochanter) are heavily padded.
- Arm Suspension: The operative arm is placed in a sterile traction sleeve (e.g., STAR sleeve) and suspended with 10 to 15 pounds of traction. The arm should be positioned in approximately 45 degrees of abduction and 20 degrees of forward flexion. This position opens the posterior joint space and relaxes the posterior capsule.
2. The Surgical Approach
- Incision: Make a vertical or slightly oblique incision over the posterior aspect of the shoulder, centered over the posterior joint line. The incision typically extends from the posterolateral corner of the acromion distally for about 8 to 10 cm.
- Deltoid Split: Identify the raphe between the middle and posterior thirds of the deltoid. Split the deltoid bluntly in line with its fibers.
Surgical Warning: Do not extend the deltoid split further than 5 cm distal to the acromion to avoid injury to the axillary nerve, which crosses the deep surface of the deltoid.
- Deep Exposure: Retract the deltoid to expose the underlying posterior rotator cuff. Identify the interval between the infraspinatus and the teres minor. Alternatively, identify the bipennate structure of the infraspinatus (Shaffer modification).
- Interval Development: Carefully split the chosen interval. Retract the infraspinatus superiorly and the teres minor inferiorly to expose the underlying posterior capsule.
3. Capsular Exposure and Arthrotomy
- Capsular Separation: Use blunt dissection and a Cobb elevator to separate the posterior capsule from the overlying rotator cuff muscles. This step is critical; the capsule must be completely mobilized to allow for an adequate shift.
- Transverse Arthrotomy: Make a transverse arthrotomy incision into the posterior capsule, starting laterally near the humeral insertion and proceeding medially toward the glenoid labrum.
- Joint Inspection: Retract the capsular edges and inspect the glenohumeral joint. Evaluate the articular cartilage, the anterior structures, and the posterior labrum.
4. Creating the Capsular Flaps
- T-Shaped Incision: Create two capsular flaps by making a vertical incision into the capsule parallel to the glenoid cavity, just adjacent to the labrum. This converts the transverse arthrotomy into a "T" shape.
- Tagging: Immediately tag the superior and inferior capsular flaps with heavy nonabsorbable traction sutures (e.g., #2 FiberWire or Ethibond) to maintain control.
Clinical Pearl: The inferior capsular flap must be developed with extreme caution. The axillary nerve lies in close proximity to the undersurface of the inferior capsule. Keep all dissection strictly on the capsular tissue and avoid plunging inferiorly.
5. Labral Assessment and Preparation
- Intact Labrum: If the posterior labrum is firmly attached and structurally sound, it can be used as the foundation for the capsular repair. Sutures can be passed directly through the intact labral tissue.
- Torn Labrum (Reverse Bankart): If the labrum is detached, it must be mobilized and repaired. Lightly decorticate the posterior glenoid neck with a rasp or motorized burr to create a bleeding bone bed. Place 2 to 3 suture anchors into the posterior glenoid rim (typically at the 7, 8, and 9 o'clock positions for a right shoulder).
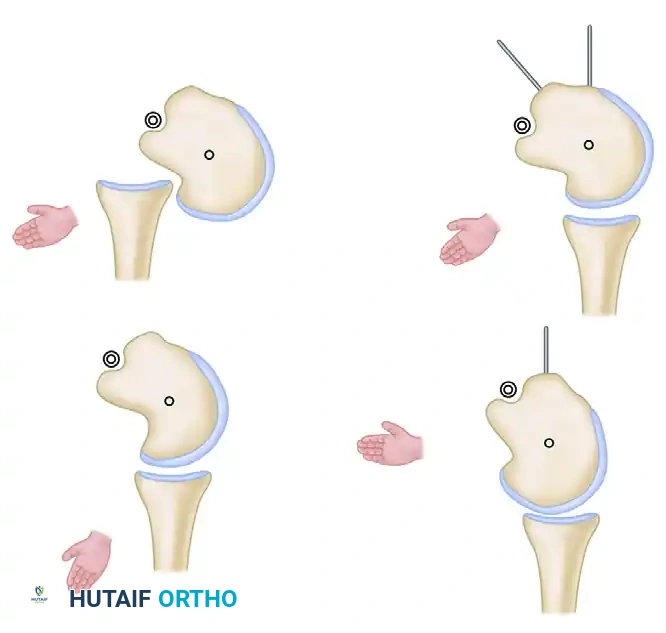
6. The Capsular Shift and Imbrication
This is the most critical step of the Tibone and Bradley technique, dictating the biomechanical success of the operation.
- Inferior Flap Advancement: Take the sutures from the inferior capsular flap (or the sutures passed through the inferior anchors/labrum) and advance the inferior flap superiorly and medially. Tie these sutures securely.
- Biomechanical Rationale: This maneuver obliterates the redundant inferior capsular pouch and tightly tensions the posterior band of the IGHL, effectively eliminating posteroinferior instability.
- Superior Flap Advancement: Next, take the superior capsular flap and advance it inferiorly and medially, directly over the previously secured inferior flap. Suture this flap to the labrum or the underlying inferior flap.
- Biomechanical Rationale: This "pants-over-vest" imbrication creates a double-layered, significantly thickened posterior soft-tissue restraint, acting as a robust bumper against posterior humeral translation.
- Lateral Closure: After the medial shift is complete, a transverse gap will remain laterally in the capsule. Close this gap with interrupted mattress sutures to ensure a watertight seal and uniform capsular tension.
7. Closure
- Remove traction and assess the stability and range of motion. The shoulder should easily reach neutral rotation without excessive tension, but posterior translation should be firmly eliminated.
- The teres minor and infraspinatus muscles naturally fall back together. They usually do not require suturing, though a few loose approximating sutures can be placed in the epimysium.
- Close the deltoid split, subcutaneous tissue, and skin in a standard layered fashion.
Postoperative Rehabilitation Protocol
The rehabilitation following a Tibone and Bradley posterior capsular shift is deliberately conservative to protect the soft-tissue imbrication. Premature stretching is the leading cause of recurrent instability.
Phase I: Maximum Protection (Weeks 0 to 3)
- Immobilization: The shoulder is placed in a specialized abduction orthosis (abduction pillow) positioning the arm in 15 to 20 degrees of abduction, slight extension, and neutral rotation.
- Rationale: Immobilization in internal rotation places maximum stress on the posterior repair and must be strictly avoided.
- Exercises: Active range of motion (ROM) of the elbow, wrist, and hand. Scapular retractions are encouraged. No glenohumeral motion is permitted.
Phase II: Moderate Protection and Early Motion (Weeks 3 to 6)
- Discontinuation of Brace: The abduction pillow is removed at 3 weeks.
- ROM Progression: Initiate active and active-assisted ROM exercises.
- Safe Zones: Emphasis is placed on elevating the arm strictly in the scapular plane (scaption). Internal and external rotation are gradually restored.
Clinical Pearl: Avoid combined flexion, adduction, and internal rotation, as this position directly stresses the posterior capsular repair.
Phase III: Strengthening (Weeks 6 to 12)
- Advanced ROM: At 6 weeks, forward flexion is permitted and progressed to full.
- Strengthening: Initiate isotonic strengthening of the rotator cuff and periscapular stabilizers. Focus heavily on the posterior deltoid, infraspinatus, and teres minor to provide dynamic posterior stability.
- Proprioception: Rhythmic stabilization and closed kinetic chain exercises are integrated.
Phase IV: Return to Sport (Months 3 to 12)
- Month 3: Weightlifting is permitted, progressing gradually to increase strength and muscular endurance. Avoid heavy bench presses or exercises that force the elbows behind the plane of the body.
- Month 6: Light throwing programs and non-contact sports-specific drills can be resumed.
- Month 12: A full return to competitive throwing and heavy contact sports is permitted, provided the athlete has achieved full, pain-free ROM and isokinetic strength testing demonstrates at least 90% strength compared to the contralateral limb.
Complications and Pitfalls
While highly effective, the Tibone and Bradley technique carries specific risks that the orthopedic surgeon must anticipate and mitigate.
- Recurrent Instability: The most common complication of posterior stabilization. It is usually secondary to unrecognized glenoid retroversion, failure to adequately shift the inferior capsule, or patient non-compliance with the postoperative immobilization protocol.
- Over-tightening and Stiffness: Excessive superior advancement of the inferior flap can lead to severe restriction of internal rotation. The shift must be anatomic, reducing redundancy without tethering the joint.
- Axillary Nerve Injury: As previously noted, the axillary nerve is highly vulnerable during the inferior capsular dissection. Meticulous hemostasis and direct visualization of capsular planes are mandatory.
- Hardware Complications: If suture anchors are utilized, improper trajectory can result in articular cartilage penetration. Anchors must be placed precisely on the glenoid face, angled away from the articular surface.
Conclusion
The Tibone and Bradley technique remains a gold-standard open procedure for the management of moderate posterior shoulder instability. By intelligently utilizing the internervous or intermuscular planes of the posterior rotator cuff, surgeons can achieve excellent exposure of the posterior capsule. The subsequent T-shaped capsulotomy and pants-over-vest imbrication provide a biologically robust, thickened posterior restraint. When combined with rigorous patient selection and a disciplined postoperative rehabilitation protocol, this technique yields excellent long-term outcomes, allowing high-demand athletes to return to their pre-injury levels of performance.
You Might Also Like