Partial-Thickness Rotator Cuff Tears: Repair or Debride?
Key Takeaway
Your ultimate guide to Partial-Thickness Rotator Cuff Tears: Repair or Debride? starts here. For a 5mm deep partial-thickness rotator cuff tear, treatment is guided by the Ellman classification. An articular-sided tear (3-6mm) typically warrants debridement. Conversely, a bursal-sided partial-thickness rotator cuff tear of this depth (3-6mm) generally requires surgical repair. This ensures appropriate management based on tear characteristics.
Introduction and Epidemiology
Partial-thickness rotator cuff tears represent a complex and frequently encountered pathology in orthopedic sports medicine and shoulder surgery. Unlike full-thickness tears, which present with a clear disruption of the tendon from the bursal to the articular surface, partial-thickness tears involve only a portion of the tendon substance. The fundamental clinical dilemma surrounding these lesions remains the decision-making process between arthroscopic debridement and surgical repair. This decision is dictated by tear depth, location, patient age, activity level, and the chronicity of symptoms.
The epidemiology of partial-thickness rotator cuff tears is characterized by a high prevalence, particularly in the aging population and overhead athletic cohorts. Cadaveric studies have historically demonstrated that partial-thickness tears are more common than full-thickness tears, with an estimated prevalence ranging from 13 percent to 32 percent in the general population. The incidence increases significantly with advancing age, suggesting a degenerative component to the etiology. However, in young overhead athletes, such as baseball pitchers and tennis players, these tears frequently manifest as articular-sided lesions secondary to internal impingement and repetitive microtrauma.
Understanding the precise pathophysiology is critical for guiding management. The etiology is generally divided into intrinsic and extrinsic factors. Intrinsic factors include age-related microvascular changes, specifically within the critical zone of Codman, leading to localized ischemia, tenocyte apoptosis, and subsequent myxoid degeneration. Extrinsic factors involve mechanical compression, such as subacromial impingement against the coracoacromial arch, or internal impingement where the articular surface of the supraspinatus and infraspinatus abuts the posterosuperior glenoid rim during extreme abduction and external rotation.
Pathophysiology and Classification
The most widely utilized system for categorizing partial-thickness rotator cuff tears is the Ellman classification, which stratifies tears based on location and depth.
Location is designated as:
* Type A: Articular sided tears
* Type B: Bursal sided tears
* Type I: Interstitial or intratendinous tears
Depth is graded based on the percentage of footprint involvement:
* Grade 1: Less than 3 mm depth (less than 25 percent of the footprint)
* Grade 2: 3 to 6 mm depth (25 to 50 percent of the footprint)
* Grade 3: Greater than 6 mm depth (greater than 50 percent of the footprint)
Articular-sided tears are approximately two to three times more common than bursal-sided tears. However, bursal-sided tears are generally considered more symptomatic and exhibit a higher propensity for rapid progression to full-thickness tears due to the distinct biomechanical environment of the subacromial space.
Surgical Anatomy and Biomechanics
A profound understanding of the rotator cuff footprint anatomy and the microstructural properties of the tendon is imperative for evaluating tear depth and executing a biomechanically sound repair.
Rotator Cuff Footprint and Microanatomy
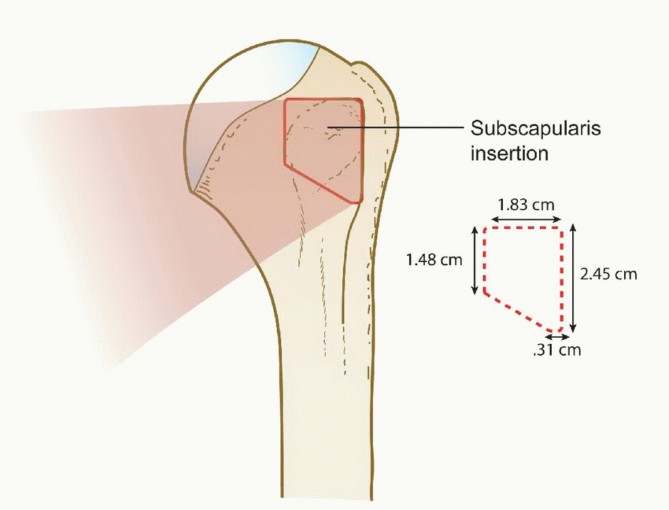
The supraspinatus and infraspinatus tendons insert onto the greater tuberosity of the proximal humerus, creating a complex, interdigitated footprint. The supraspinatus footprint is classically described as triangular, measuring approximately 14 to 16 mm in the medial-to-lateral dimension and 25 mm in the anterior-to-posterior dimension. The infraspinatus footprint is larger and more trapezoidal. Recognizing the 14 to 16 mm medial-to-lateral width is the cornerstone of intraoperative decision-making; a tear exposing 7 to 8 mm of the lateral articular footprint represents a 50 percent partial-thickness tear.
Histologically, the rotator cuff is not a homogeneous structure. Clark and Harryman described five distinct layers of the supraspinatus and infraspinatus tendons:
1. Layer One: The superficial coracohumeral ligament fibers.
2. Layer Two: Densely packed, parallel tendon fibers (the primary load-bearing layer).
3. Layer Three: A loose network of crossing collagen fibers.
4. Layer Four: Loose connective tissue containing the deep extension of the coracohumeral ligament.
5. Layer Five: The true glenohumeral joint capsule.
Partial-thickness tears most commonly occur at the interface of these layers, particularly involving the articular capsule (Layer Five) and the deep tendon fibers (Layers Three and Four) in articular-sided tears, or the superficial layers in bursal-sided tears.
Biomechanical Principles
The biomechanical behavior of the rotator cuff explains the pathogenesis and the rationale for surgical intervention. The articular and bursal layers of the tendon possess distinct biomechanical properties. The articular fibers have a lower ultimate tensile strength but are significantly stiffer than the bursal fibers. This discrepancy creates a "strain mismatch" during loading. When the shoulder is subjected to tensile forces, the stiffer articular fibers fail first, explaining the higher incidence of articular-sided tears.
Furthermore, Burkhart's description of the rotator cable and crescent is vital. The rotator cable is a thick bundle of fibers running perpendicular to the supraspinatus tendon, spanning from the coracohumeral ligament to the infraspinatus, shielding the thinner, avascular rotator crescent. If a partial tear compromises the integrity of the rotator cable, the biomechanical transmission of force is severely altered, necessitating repair regardless of the strict percentage of depth.
Indications and Contraindications
The management of partial-thickness rotator cuff tears requires a nuanced approach, balancing the natural history of the disease against the morbidity of surgical intervention. Non-operative management remains the initial standard of care for the majority of degenerative partial-thickness tears.
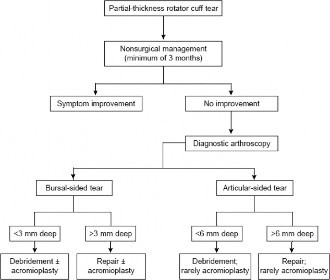
Decision Making Algorithm
Non-operative modalities include physical therapy focusing on periscapular stabilization and rotator cuff strengthening, non-steroidal anti-inflammatory drugs, and judicious use of subacromial or intra-articular corticosteroid injections. Biologic augmentations, such as platelet-rich plasma, are actively being investigated but remain an adjunct rather than a definitive cure.
Surgical intervention is indicated when patients experience persistent pain and functional limitation despite a comprehensive non-operative regimen lasting 3 to 6 months. Acute traumatic partial tears in young, active patients may warrant earlier surgical consideration.
The crux of the surgical decision lies in whether to debride the lesion or perform a structural repair. The widely accepted threshold is the "50 percent rule."
* Tears involving less than 50 percent of the tendon thickness (Grade 1 and early Grade 2) are generally treated with arthroscopic debridement, with or without subacromial decompression.
* Tears involving greater than 50 percent of the tendon thickness (Grade 3 and deep Grade 2) require surgical repair to restore the biomechanical integrity of the footprint and prevent progression to a full-thickness tear.
Bursal-sided tears are less forgiving. Due to the high rate of progression and significant pain associated with bursal-sided pathology, many surgeons advocate for repair at a lower threshold, often repairing bursal tears that exceed 3 mm in depth.
| Clinical Variable | Operative Indication | Non Operative Indication |
|---|---|---|
| Duration of Symptoms | > 3 to 6 months of failed conservative therapy | < 3 months, initial presentation |
| Tear Depth | > 50% footprint involvement (> 6-7 mm) | < 50% footprint involvement (< 6 mm) |
| Tear Location | Bursal-sided > 3mm depth | Articular-sided < 50% depth |
| Patient Profile | Young, overhead athlete, high functional demand | Elderly, low demand, multiple comorbidities |
| Trauma History | Acute traumatic avulsion | Insidious, degenerative onset |
| Associated Pathology | Concomitant unstable SLAP tear or biceps pathology | Isolated, stable partial tear |
Contraindications to surgical repair include advanced glenohumeral osteoarthritis, active joint infection, severe medical comorbidities precluding anesthesia, and profound stiffness (adhesive capsulitis), which must be resolved prior to any rotator cuff intervention.
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is essential for anticipating the tear pattern and ensuring the appropriate equipment is available.
Imaging Modalities
Standard radiographs (true anteroposterior, scapular Y, and axillary lateral views) are obtained to assess for acromial morphology, os acromiale, calcific tendinitis, and degenerative joint changes.
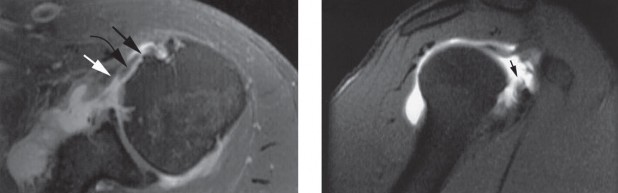
Magnetic Resonance Imaging (MRI) is the gold standard for evaluating rotator cuff pathology. On T2-weighted sequences, a partial-thickness tear appears as a focal region of hyperintensity that does not traverse the entire tendon substance. For articular-sided tears, Magnetic Resonance Arthrography (MRA) provides superior sensitivity and specificity. The intra-articular contrast distends the joint and readily enters articular-sided defects. The ABER (Abduction and External Rotation) view on MRI is particularly useful for visualizing articular-sided tears and assessing internal impingement.
Anesthesia and Positioning Setup
Surgery is typically performed under general anesthesia supplemented with an interscalene regional nerve block for optimal postoperative pain control.
Patient positioning is based on surgeon preference, utilizing either the beach chair or lateral decubitus position.
* Beach Chair Position: Offers the advantage of an upright anatomical orientation, ease of conversion to an open procedure if necessary, and excellent visualization of the subacromial space. However, it carries a risk of cerebral hypoperfusion and requires careful blood pressure monitoring.
* Lateral Decubitus Position: Provides excellent joint distraction, which is highly beneficial for visualizing and instrumenting articular-sided tears. Traction is applied via a dedicated suspension system. Care must be taken to pad all bony prominences and avoid excessive traction to prevent neuropraxia.
Detailed Surgical Approach and Technique
The surgical execution requires meticulous diagnostic arthroscopy, precise measurement of the tear, and a decision to either debride, perform a transtendon repair, or complete the tear and repair it to the footprint.
Diagnostic Arthroscopy and Tear Measurement
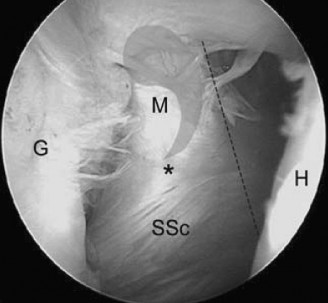
A standard posterior viewing portal is established. A thorough diagnostic arthroscopy of the glenohumeral joint is performed. The articular surface of the rotator cuff is inspected. An articular-sided partial tear (often referred to as a PASTA lesion - Partial Articular Supraspinatus Tendon Avulsion) will present as a detachment of the tendon from the medial footprint.
An anterior portal is established within the rotator interval. An arthroscopic probe is introduced to palpate the tear and assess the quality of the remaining tissue. The critical step is measuring the exposed footprint. A calibrated probe is used to measure the distance from the articular margin of the cartilage to the intact tendon insertion. If the exposed footprint measures greater than 7 mm, the tear is deemed >50% and warrants repair.
To correlate the articular findings with the bursal surface, a marker suture (e.g., PDS) is passed through the tear via a spinal needle from the subacromial space into the joint.
Arthroscopic Debridement
For tears involving less than 50 percent of the tendon thickness, arthroscopic debridement is performed. The goal is to remove frayed, degenerative, and non-viable tissue to stimulate a healing response and eliminate mechanical catching. An arthroscopic shaver or radiofrequency ablation wand is used carefully to debride the margins of the tear back to stable, healthy tendon tissue. It is imperative not to over-debride and inadvertently convert a stable partial tear into a functionally significant defect.
Following intra-articular debridement, the arthroscope is redirected into the subacromial space. A bursectomy is performed. If there is evidence of extrinsic impingement, an acromioplasty (subacromial decompression) is executed to create a flat (Type I) acromial under-surface.
Transtendon Repair Technique
For articular-sided tears greater than 50 percent depth, an in situ transtendon repair is a biomechanically superior option that preserves the intact bursal fibers.
- Footprint Preparation: The exposed greater tuberosity footprint is debrided of soft tissue and lightly decorticated using a burr or rasp to expose bleeding cancellous bone, optimizing the biologic environment for tendon healing.
- Anchor Placement: Viewing from the posterior or lateral portal, a spinal needle is used to localize the ideal trajectory for anchor placement. The needle is passed through the intact bursal portion of the tendon, directly into the prepared footprint. A small stab incision is made in the tendon, and a bioabsorbable or biocomposite suture anchor is inserted through the tendon and into the bone.
- Suture Management: The sutures are passed through the articular leaflet of the tear. This can be achieved using a spinal needle and a shuttle relay technique (e.g., passing a monofilament loop to retrieve the anchor sutures) or using a dedicated penetrating suture passer.
- Knot Tying: The sutures are tied in the subacromial space. Because the intact bursal fibers obscure the articular repair, the knots are tied "blindly" over the bursal surface, compressing the articular leaflet down to the footprint. Alternatively, knotless anchor constructs can be utilized to minimize subacromial knot impingement.
Tear Completion and Repair Technique
An alternative approach for high-grade partial tears is to intentionally complete the tear, converting it into a full-thickness defect, followed by a standard single or double-row rotator cuff repair.
- Tear Completion: Using an arthroscopic scalpel or radiofrequency device, the remaining intact bursal fibers are transected in line with the tear.
- Mobilization: The entire tendon edge is mobilized. This allows for a comprehensive assessment of tissue quality and ensures the tendon can be reduced to the lateral footprint without excessive tension.
- Footprint Preparation and Repair: The tuberosity is prepared. Depending on the tear size and surgeon preference, a single-row or double-row suture bridge construct is utilized.
The debate between transtendon repair and tear completion remains active. Transtendon repair preserves the native anatomy and bursal fibers, theoretically providing a stronger construct. However, it is technically demanding, alters the length-tension relationship of the intact fibers, and carries a higher risk of postoperative stiffness. Tear completion allows for a familiar, anatomic repair and excision of degenerative tissue but sacrifices intact tendon. Current literature suggests equivalent long-term clinical outcomes between the two techniques, though tear completion has a faster recovery of motion.
Complications and Management
Surgical management of partial-thickness rotator cuff tears is generally highly successful, but complications can occur and must be managed systematically.
Postoperative Stiffness
Postoperative stiffness, or secondary adhesive capsulitis, is the most common complication, particularly following transtendon repair. The tethering of the intact bursal fibers and the alteration of the tendon's length-tension relationship contribute to this phenomenon. Management begins with aggressive, supervised physical therapy emphasizing prolonged, low-load passive stretching. Intra-articular corticosteroid injections can rapidly decrease capsular inflammation. If stiffness persists beyond 6 to 9 months despite conservative measures, arthroscopic capsular release may be indicated.
Construct Failure and Retear
Failure of tendon healing or retear can occur due to poor tissue quality, inadequate footprint preparation, or non-compliance with postoperative rehabilitation. Patients present with recurrent pain and weakness. Diagnosis is confirmed via MRI. Management depends on the patient's symptoms. Asymptomatic retears are treated conservatively. Symptomatic retears in appropriate surgical candidates may require revision repair, potentially augmented with biologic patches or superior capsule reconstruction if the tissue is deemed irreparable.
| Complication | Estimated Incidence | Prevention and Salvage Strategy |
|---|---|---|
| Postoperative Stiffness | 10% - 15% (Higher in transtendon) | Early passive ROM; Corticosteroid injection; Arthroscopic capsular release |
| Retear / Failure to Heal | 5% - 10% | Meticulous footprint prep; Tension-free repair; Revision repair or augmentation |
| Anchor Pullout | < 2% | Assess bone quality; Use appropriately sized anchors; Revision with larger/different anchors |
| Infection | < 1% | Preoperative antibiotics; Chlorhexidine prep; Irrigation and debridement, targeted antibiotics |
| Iatrogenic Chondrolysis | Rare (Historical) | Avoid intra-articular pain pumps with bupivacaine; Ensure anchors are flush/countersunk |
Post Operative Rehabilitation Protocols
Rehabilitation protocols must be tailored to the specific surgical procedure performed. A simple debridement allows for an accelerated protocol, whereas a structural repair requires a phased approach to protect the healing tendon-to-bone interface.
Phase One Protection
For patients undergoing repair (transtendon or completion), Phase One encompasses the first 4 to 6 weeks. The primary goal is protection of the repair while preventing extreme stiffness. The patient is immobilized in an abduction sling. Passive range of motion (ROM) is initiated immediately, focusing on forward elevation and external rotation within safe limits defined intraoperatively. Active motion of the elbow, wrist, and hand is encouraged.
For patients undergoing debridement only, the sling is used for comfort for 1 to 2 weeks, and active-assisted ROM is initiated almost immediately.
Phase Two Motion
Phase Two (weeks 6 to 12) marks the transition from passive to active-assisted and eventually active range of motion. The sling is discontinued. Scapulothoracic mechanics are heavily emphasized to prevent compensatory shoulder hiking. Aquatic therapy can be highly beneficial during this phase. The goal by the end of week 12 is to achieve full, symmetric active range of motion.
Phase Three Strengthening
Phase Three (weeks 12 to 24) introduces progressive resistance exercises. Strengthening begins with isometric exercises and advances to isotonic exercises using resistance bands and light weights. Focus is placed on the rotator cuff force couples and periscapular stabilizers (rhomboids, serratus anterior, trapezius).
Return to overhead sports or heavy manual labor is typically not permitted until 6 months postoperatively, contingent upon the restoration of full strength, absence of pain, and normal dynamic scapular control.
Summary of Key Literature and Guidelines
The academic discourse surrounding partial-thickness rotator cuff tears is robust, with several landmark studies guiding current clinical practice.
Weber (1999) published a seminal study evaluating the outcomes of arthroscopic debridement versus repair for high-grade partial tears. The study demonstrated that patients with tears >50% depth who underwent debridement alone had significantly higher rates of continued pain and progression to full-thickness tears compared to those who underwent repair, establishing the foundation for the "50 percent rule."
Cordasco et al. further refined the indications, highlighting the aggressive natural history of bursal-sided tears. Their work suggested that bursal-sided tears >3 mm in depth have a high rate of clinical failure with non-operative management and warrant earlier surgical consideration compared to articular-sided tears of similar depth.
Shin et al. provided a critical comparative analysis between in situ transtendon repair and tear completion followed by repair. Their prospective data indicated that while both techniques yield excellent long-term functional scores (ASES and Constant scores), the tear completion group experienced a faster recovery of range of motion and lower rates of early postoperative stiffness, whereas the transtendon group theoretically maintained superior biomechanical strength at time zero.
The American Academy of Orthopaedic Surgeons (AAOS) appropriate use criteria generally support a trial of conservative management for degenerative partial tears, reserving surgical repair for symptomatic high-grade tears (>50%) or acute traumatic tears in physiologically young patients. The literature underscores that meticulous surgical technique, whether transtendon or tear completion, combined with structured rehabilitation, is paramount for optimizing patient outcomes in this challenging clinical entity.
You Might Also Like