Arthroscopic Acromioplasty: The Chockblock Method and Management of Partial-Thickness Rotator Cuff Tears
Key Takeaway
The Chockblock method for arthroscopic acromioplasty provides a highly controlled, reproducible technique for subacromial decompression. By utilizing a posterior portal for the burr and a lateral viewing portal, surgeons can precisely gauge bone resection using the burr's diameter. This guide details the step-by-step Chockblock technique, portal placement strategies, and the comprehensive management of partial-thickness rotator cuff tears, including PASTA lesions and intratendinous defects.
INTRODUCTION TO SUBACROMIAL PATHOLOGY
Subacromial impingement syndrome and partial-thickness rotator cuff tears (PTRCTs) represent a continuum of shoulder pathology frequently encountered by the orthopedic surgeon. The etiology of these conditions is multifactorial, encompassing extrinsic mechanical compression from the coracoacromial arch and intrinsic degenerative changes within the rotator cuff tendons.
Historically, open anterior acromioplasty was the gold standard for mechanical impingement. However, the advent of advanced arthroscopic techniques has revolutionized the approach, minimizing deltoid morbidity and accelerating rehabilitation. Among these techniques, the Chockblock Method for Acromioplasty, popularized by Sampson et al., offers unparalleled precision in bone resection. By utilizing the known diameter of the arthroscopic burr as a depth gauge, surgeons can perform a smooth, mathematically precise undersurface acromioplasty, avoiding the common pitfalls of over-resection or inadequate decompression.
Concurrently, the management of partial-thickness rotator cuff tears remains a highly nuanced topic. Decision-making hinges on the tear's location (articular, bursal, or intratendinous), the percentage of tendon thickness involved, and the presence of delamination. This comprehensive guide details the biomechanical rationale, precise surgical execution of the Chockblock method, and an evidence-based algorithm for addressing partial-thickness rotator cuff tears.
PREOPERATIVE EVALUATION AND BIOMECHANICS
Pathoanatomy of Impingement
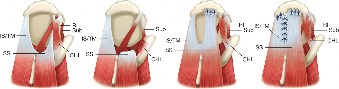
The subacromial space is bordered superiorly by the anterior undersurface of the acromion, the coracoacromial (CA) ligament, and the acromioclavicular (AC) joint. Bigliani's classification of acromial morphology (Type I: flat, Type II: curved, Type III: hooked) remains highly relevant, with Type III acromions demonstrating a strong correlation with full-thickness and bursal-sided partial-thickness rotator cuff tears. The goal of acromioplasty is to convert a Type II or III acromion into a flat Type I morphology, thereby increasing the subacromial volume and reducing mechanical friction on the supraspinatus tendon during forward elevation and internal rotation.
Imaging Modalities
Standard radiographic evaluation should include a true anteroposterior (Grashey), axillary lateral, and supraspinatus outlet (Y-scapula) view to assess acromial morphology and acromiohumeral distance. Magnetic Resonance Imaging (MRI) or MR Arthrography is the gold standard for evaluating the rotator cuff. MR Arthrography is particularly sensitive for detecting Partial Articular-Sided Tendon Avulsion (PASTA) lesions and intratendinous delamination, which may be underappreciated on standard non-contrast MRI.
Clinical Pearl: Intratendinous tears are notoriously difficult to visualize during standard diagnostic arthroscopy. Preoperative MRI localization is critical. Measure the distance of the intratendinous cyst or tear from the biceps tendon and the lateral edge of the footprint to guide intraoperative spinal needle localization.
SURGICAL SETUP AND PORTAL PLACEMENT
Patient Positioning
The procedure may be performed in either the beach chair or lateral decubitus position, depending on surgeon preference.
* Beach Chair: Offers a highly anatomic orientation, excellent access to the subacromial space, and ease of conversion to an open procedure if necessary. Care must be taken to secure the head in a neutral position to avoid cervical neurapraxia.
* Lateral Decubitus: Provides excellent joint distraction and visualization of the articular surface, which is particularly beneficial for evaluating and repairing articular-sided partial tears.
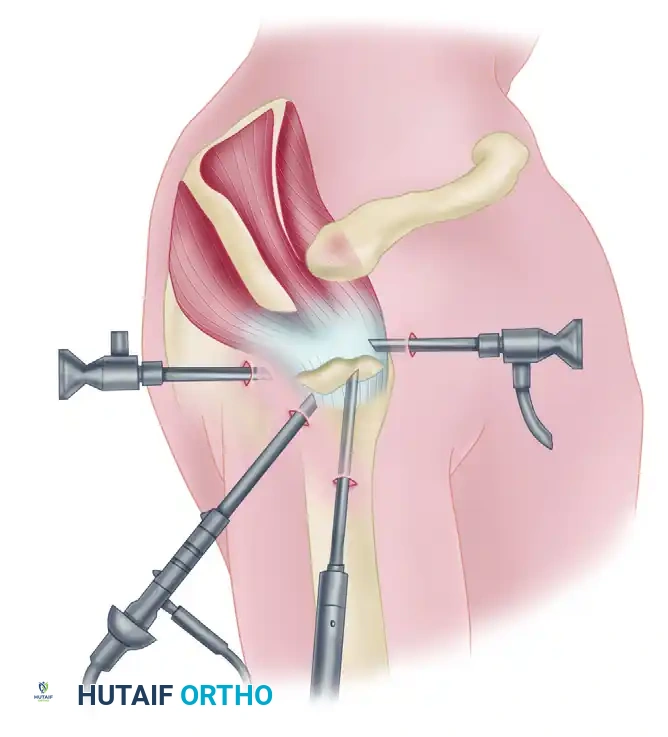
Portal Placement and Arthroscopic Anatomy
Precise portal placement is the foundation of successful arthroscopic shoulder surgery. Overcrowding of portals leads to instrument collision, poor trajectory, and surgical frustration.
Figure 52-33: Relative location of portals. The middle working portal is located at the center of the rotator cuff tear and 3 cm lateral from the lateral margin of the acromion. The rear viewing portal is placed at the posterior lip of the tear and 1 cm lateral from the lateral margin of the acromion. Portals should be placed at least 2 cm apart to prevent overcrowding.
- Standard Posterior Portal: Established 2 cm inferior and 1 cm medial to the posterolateral corner of the acromion. Used primarily for initial glenohumeral diagnostic arthroscopy and later as the working portal for the burr in the Chockblock method.
- Lateral Portal: Established 2 to 3 cm lateral to the lateral edge of the acromion, in line with the posterior aspect of the clavicle. This serves as the primary viewing portal during the Chockblock acromioplasty.
- Anterior Portal: Established via an outside-in technique using a spinal needle, entering the rotator interval just lateral to the coracoid process.
Surgical Warning: When establishing the lateral portal, avoid placing it too inferiorly, as this risks injury to the axillary nerve, which typically runs 5 cm distal to the lateral acromial edge.
THE CHOCKBLOCK METHOD FOR ACROMIOPLASTY
The Chockblock method, described by Sampson et al., is a highly systematic approach to subacromial decompression. It utilizes a posterior-to-anterior burr trajectory while viewing from the lateral portal, allowing the surgeon to use the burr itself as a depth gauge (the "chockblock").
Step-by-Step Surgical Technique
Step 1: Subacromial Bursectomy and Preparation
Following the glenohumeral diagnostic arthroscopy, the arthroscope is redirected into the subacromial space via the posterior portal. A lateral portal is established. A motorized shaver and radiofrequency ablation wand are introduced laterally to perform a thorough subacromial bursectomy. The CA ligament is identified, and its acromial attachment is carefully released using electrocautery, exposing the anterior undersurface of the acromion.
Step 2: Portal Transition
Once the bony architecture is clearly visualized, the arthroscope is moved to the lateral portal. This provides a panoramic view of the undersurface of the acromion from lateral to medial.
Step 3: Introduction of the Burr
A 4.0-mm or 5.5-mm round burr is introduced through the posterior portal. The posterior portal tract should allow the burr to enter the subacromial space approximately 2 to 3 cm distal to the undersurface of the acromion, allowing it to lie parallel to the acromial undersurface.
Step 4: Gauging the Resection (The "Chockblock" Concept)
Pass the burr anteriorly, up under the anterior edge of the acromion, into the space between the rotator cuff footprint and the concavity of the acromion. By placing the burr flat against the bone, the surgeon uses the known diameter of the burr (e.g., 4 mm) to visually determine the exact amount of bone to be removed to achieve a flat Type I morphology.
Step 5: Systematic Bone Resection
Bring the burr back to the posterior edge of the apex over the curvature. Begin sweeping the burr from medial to lateral, resecting the bone from the posterior part of the curve advancing toward the anterior aspect.
* Keep the burr completely flat and parallel to the acromion.
* Avoid "divoting" or creating a reverse slope.
* The resection should extend medially to the AC joint and laterally to the lateral edge of the acromion.
Alternative Approach (Lateral to Posterior Transition)
An alternative technique, preferred by some senior authors, involves starting the procedure with the acromionizer (burr) in the lateral portal.
1. View from the posterior portal.
2. Use the burr in the lateral portal to resect the anterior and lateral edges of the acromion, establishing the initial depth and trajectory.
3. Once the anterior edge is flattened, transition the arthroscope to the lateral portal and move the burr to the posterior portal to complete the posterior-to-anterior smoothing, as described in the standard Chockblock method.
Pitfall: Failure to adequately resect the anterolateral corner of the acromion is a common cause of persistent postoperative impingement. Ensure the resection extends fully to the lateral border.
SURGICAL MANAGEMENT OF PARTIAL-THICKNESS ROTATOR CUFF TEARS
Partial-thickness rotator cuff tears (PTRCTs) present a complex decision-making matrix. They are broadly classified by location:
1. Articular-sided tears: Most common, frequently seen in overhead athletes (PASTA lesions).
2. Bursal-sided tears: Often associated with subacromial impingement.
3. Intratendinous tears: Contained within the tendon substance, often degenerative.
The Ellman classification further grades these tears by depth: Grade 1 (<3 mm), Grade 2 (3-6 mm), and Grade 3 (>6 mm or >50% thickness).
Decision-Making Algorithm
The treatment of PTRCTs must be highly individualized, factoring in the patient's age, activity level, tear depth, and tissue quality.
- Tears < 50% Thickness: Generally treated with arthroscopic debridement. For bursal-sided tears, a subacromial decompression (acromioplasty) is performed if mechanical impingement is identified. Goodmurphy et al. demonstrated that extensive debridement of the tendon is unnecessary and may weaken the remaining intact fibers; therefore, debridement should be limited to removing frayed, non-viable tissue to promote a healing response.
- Tears 30% to 50% Thickness: This represents the "gray area" of rotator cuff surgery. Management depends heavily on patient demographics. A young, overhead athlete with a 40% articular-sided tear may require repair, whereas an elderly, low-demand patient with a similar tear may be managed with debridement alone.
- Tears > 50% Thickness: Biomechanical studies indicate that tears involving 50% or more of the tendon thickness significantly alter the strain environment of the remaining intact fibers, predisposing them to propagation and catastrophic failure. These tears are best treated with surgical repair.
Surgical Techniques for Partial Tears
1. Transtendinous Repair for PASTA Lesions
For partial articular-sided supraspinatus tendon avulsion (PASTA) injuries involving >50% of the footprint, a transtendinous repair is indicated. This technique preserves the intact bursal-sided fibers, maintaining the native lateral footprint attachment.
* Technique: A spinal needle is used to localize the tear from the bursal side. A PDS suture is passed through the needle to mark the lesion. Viewing from the subacromial space, a longitudinal split is made in the intact bursal fibers in line with the tendon fibers. One or two suture anchors are placed into the medial articular margin of the footprint. The sutures are passed through the articular half of the tendon using a suture-passing device and tied over the bursal surface, compressing the articular tear down to the bone.
2. Management of Delaminated Tears
Delamination—where the articular and bursal layers of the tendon shear and retract independently—is common in throwing athletes and sports requiring repetitive overhead motion.
* If delamination is present, a simple debridement is insufficient. A transtendinous repair or a specialized double-row repair that independently tensions the articular and bursal leaflets is required to restore the anatomic footprint and prevent interstitial cyst formation.
3. High-Grade Tears (>80% Thickness)
Tears involving more than 80% of the tendon thickness behave biomechanically like full-thickness tears.
* Take-Down vs. In Situ Repair: Historically, these tears were "taken down" (converted to a full-thickness tear by excising the remaining intact fibers) and repaired primarily. However, modern consensus dictates that if the remaining tendon and its lateral attachments are of robust, healthy quality, they should not be sacrificed. An in situ repair (transtendinous) is preferred.
* Conversely, if the remaining 20% of the tendon is severely degenerative, attenuated, and of poor quality, it is more efficient to take down the tear, debride the footprint, and perform a standard primary double-row or single-row repair.
4. Intratendinous Tears
Intratendinous tears are entirely concealed within the tendon substance.
* Localization: They must be identified on preoperative MRI. Intraoperatively, a spinal needle is used to probe the tendon based on MRI measurements.
* Technique: Once localized, an arthroscopic scalpel or radiofrequency wand is used to create a small longitudinal incision in the bursal surface to open the tear. The necrotic edges of the internal cyst/tear are slightly debrided to bleeding tissue to promote local healing. The defect is then repaired side-to-side using standard arthroscopic suturing techniques (e.g., figure-of-eight or horizontal mattress sutures) to close the dead space.
POSTOPERATIVE REHABILITATION PROTOCOL
The postoperative rehabilitation protocol must be tailored to the exact procedures performed. An isolated acromioplasty allows for rapid mobilization, whereas a concomitant rotator cuff repair requires a period of strict protection.
Protocol for Isolated Acromioplasty / Debridement
- Phase I (Days 1-7): The arm is placed in a standard sling for comfort. Codman pendulum exercises are initiated on postoperative day one. The sling is discarded as soon as comfort permits (typically within 3 to 5 days). Active-assisted range-of-motion (AAROM) exercises and isometric strengthening for the deltoid and rotator cuff are begun within the first week.
- Phase II (Weeks 2-3): Light resistance exercises using elastic tubing are initiated. Scapular stabilization exercises are emphasized. Most patients achieve full, symmetric range of motion by 3 weeks.
- Phase III (Weeks 4-12): Supervised progressive resistance exercises are instituted. Activities of daily living (ADLs) are resumed as symptoms allow.
- Phase IV (3 Months+): Return to heavy labor or overhead sports is delayed until full strength, endurance, and completely pain-free motion are obtained, typically around the 3-month mark.
Protocol for Partial Rotator Cuff Repair
If a transtendinous, side-to-side, or take-down repair was performed, the protocol is significantly more conservative to protect the healing tendon-to-bone interface.
* Phase I (Weeks 0-4): Strict immobilization in an abduction sling. Only passive range of motion (PROM) is permitted. No active forward elevation or abduction.
* Phase II (Weeks 4-8): Discontinue sling. Initiate AAROM. Progress to active range of motion (AROM) by week 6. No resistance.
* Phase III (Weeks 8-12): Begin light isometric strengthening, progressing to isotonic elastic band exercises.
* Phase IV (Months 3-6): Advanced strengthening, plyometrics, and sport-specific training. Return to play is rarely permitted before 5 to 6 months postoperatively.
CONCLUSION
The arthroscopic management of subacromial impingement and partial-thickness rotator cuff tears requires a meticulous, evidence-based approach. The Chockblock method for acromioplasty provides the surgeon with a highly reproducible technique for achieving a flat, decompressed coracoacromial arch without the risks of over-resection. When addressing partial rotator cuff tears, the surgeon must carefully evaluate the depth, location, and tissue quality, utilizing advanced techniques such as transtendinous repair for PASTA lesions and precise side-to-side closure for intratendinous defects. Adherence to these strict surgical principles, combined with a phased, pathology-specific rehabilitation protocol, ensures optimal functional outcomes for the patient.
📚 Medical References
- Arthroscopic acromioplasty: a 6to 10-year follow-up, Arthroscopy 14:382, 1998.
- Stetson WB, Phillips T, Beutsch A: The use of magnetic resonance arthrography to detect partial-thickness rotator cuff tears, J Bone Joint Surg 87A(suppl 2):81, 2005.
- Stieda A: Zur Pathologie der Schultergelenkschlembeutel. In Lagenbeck B, ed: Archiv für Klinische Chirurgie , Berlin, 1908, Verlag von August Hirschwald. Swiontkowski M, Iannotti JP, Boulas JH, et al: Intraoperative assessment of rotator cuff vascularity using laser Doppler fl owmetry. In Post M, Morrey BE, Hawkins RJ, eds: Surgery of the shoulder, St Louis, 1990, Mosby. Swiontkowski M, Iannotti JP, Esterhai JL, et al: Intraoperative assessment of rotator cuff vascularity using laser Doppler fl owmetry. Paper presented at the Fifty-sixth Annual Meeting of the American Academy of Orthopaedic Surgeons, Las Vegas, 1989.
- Teefey SA, Rubin DA, Middleton WD, et al: Detection and quantifi cation of rotator cuff tears: comparison of ultrasonographic, magnetic resonance imaging, and arthroscopic fi ndings in seventy-one consecutive cases, J Bone Joint Surg 86A:708, 2004.
- Tempelhof S, Rupp S, Seil R: Age-related prevalence of rotator cuff tears in asymptomatic shoulders, J Shoulder Elbow Surg 8:296, 1999.
- Tennent TD, Beach WR, Meyers JF: A review of the special tests associated with shoulder examination, part I: the rotator cuff tests, Am J Sports Med 31:154, 2003.
- Tennent TD, Beach WR, Meyers JF: A review of the special tests associated with shoulder examination, part II: laxity, instability, and superior labral anterior and posterior (SLAP) lesions, Am J Sports Med 31:301, 2003.
- Thompson RC, Schneider W, Kennedy T: Entrapment neuropathy of the inferior branch of the suprascapular nerve by ganglia, Clin Orthop Relat Res 166:185, 1992.
- Tibone JE, Elrod B, Jobe FW, et al: Surgical treatment of tears of the rotator cuff in athletes, J Bone Joint Surg 68A:887, 1986.
- Tokish JM, Decker MJ, Ellis HB, et al: The belly-press test for the physical examination of the subscapularis muscle: electromyographic validation and comparison to the lift-off test, J Shoulder Elbow Surg 12:427, 2003.
- Tomlinson RJ Jr, Glousman RE: Arthroscopic debridement of
You Might Also Like