Open Lateral Release, Medial Reefing, and MPFL Reconstruction: A Comprehensive Surgical Guide
Key Takeaway
Open lateral release and mini-open medial reefing are foundational procedures for addressing patellofemoral maltracking and instability. This guide details the Nam and Karzel technique, emphasizing precise retinacular release, superolateral geniculate artery hemostasis, and anatomic medial reefing using mattress sutures. Proper execution restores patellar kinematics, while concurrent MPFL reconstruction provides robust stabilization for chronic cases, preventing recurrent dislocation and patellofemoral arthrosis.
INTRODUCTION TO PATELLOFEMORAL SURGERY
Patellofemoral instability and maltracking present a complex biomechanical challenge that requires a nuanced, patient-specific surgical approach. Historically, isolated lateral retinacular release was overutilized for anterior knee pain and instability, often leading to suboptimal outcomes or iatrogenic medial patellar subluxation. Today, the indications have been rigorously refined. Open lateral release is now primarily reserved for documented lateral patellar compression syndrome or utilized as an essential adjunct to medial-sided stabilization procedures.
When lateral retinacular tightness is coupled with medial-sided incompetence—often following acute or recurrent patellar dislocations—a combined approach is mandated. The mini-open medial reefing combined with an arthroscopic lateral release (as popularized by Nam and Karzel) provides a powerful method to restore the delicate soft-tissue balance of the patellofemoral joint. In cases of chronic instability with severe medial patellofemoral ligament (MPFL) attenuation, formal MPFL reconstruction using a semitendinosus autograft is the gold standard.
This comprehensive guide details the biomechanical rationale, precise surgical steps, and evidence-based postoperative protocols for open lateral release, mini-open medial reefing, and MPFL reconstruction.
BIOMECHANICS AND PREOPERATIVE EVALUATION
Patellofemoral Joint Kinematics
The stability of the patellofemoral joint relies on a complex interplay of static and dynamic restraints.
* Static Restraints: The bony architecture of the trochlear groove provides primary stability at flexion angles greater than 30 degrees. The MPFL is the primary soft-tissue restraint to lateral patellar translation, contributing 50% to 60% of the restraining force from 0 to 30 degrees of flexion.
* Dynamic Restraints: The vastus medialis obliquus (VMO) dynamically pulls the patella medially, countering the lateral vector forces generated by the vastus lateralis and the iliotibial band.
Clinical and Radiographic Assessment
A meticulous examination under anesthesia (EUA) is the critical first step in the operating room. The surgeon must document the baseline range of motion, patellar tilt, and the degree of medial and lateral glide.
💡 Clinical Pearl: The Patellar Glide Test
A normal lateral glide is 1 to 2 quadrants of the patellar width. A glide of 3 or more quadrants lacking a firm endpoint indicates gross MPFL incompetence. Conversely, an inability to evert the patella past the horizontal plane or a medial glide of less than 1 quadrant indicates severe lateral retinacular tightness, justifying a lateral release.
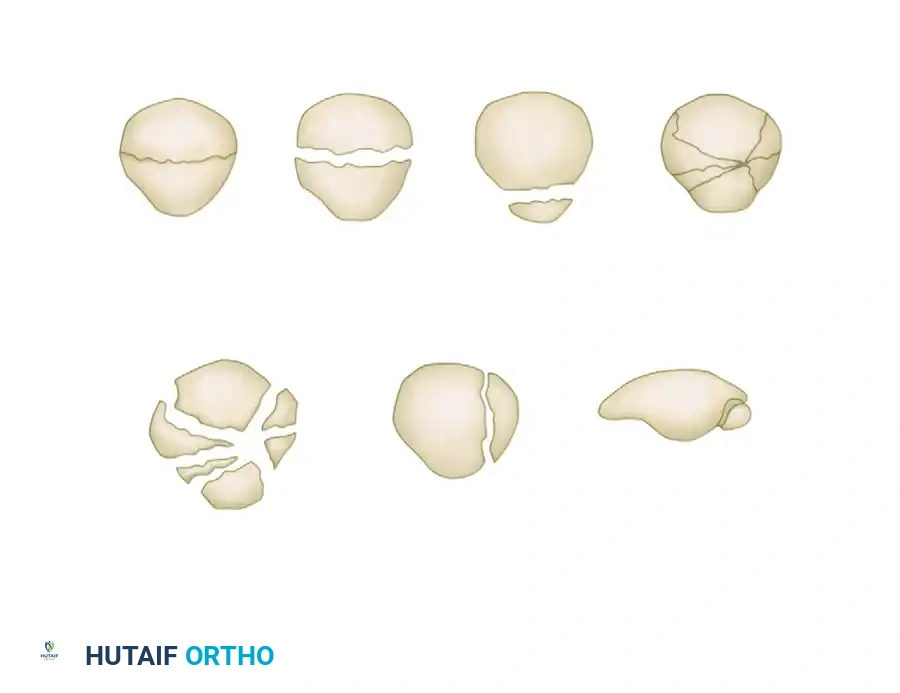
Preoperative imaging must include weight-bearing anteroposterior, lateral, and axial (Merchant or skyline) radiographs to assess patellar height (Caton-Deschamps index), trochlear dysplasia, and baseline tilt. Magnetic Resonance Imaging (MRI) is mandatory to evaluate the integrity of the MPFL, identify osteochondral shear fractures, and assess the tibial tubercle-trochlear groove (TT-TG) distance.
SURGICAL TECHNIQUE: OPEN LATERAL RELEASE
An open lateral release allows for precise, controlled division of the lateral retinaculum while minimizing the risk of postoperative hemarthrosis—a notorious complication of purely arthroscopic releases.
Diagnostic Arthroscopy
- Positioning: Place the patient supine with a lateral post and a foot piece to allow full, unhindered knee flexion and extension. Apply a proximal thigh tourniquet.
- Portal Placement: Establish standard inferolateral and inferomedial portals.
- Intra-articular Assessment: Perform a comprehensive diagnostic arthroscopy. Evaluate patellar tracking dynamically from the superolateral portal. Treat any concomitant chondral lesions with chondroplasty or address meniscal pathology via partial meniscectomy or repair before addressing the patellofemoral compartment.
The Open Release Procedure
- Incision and Dissection: Extend the anterolateral portal slightly, or make a dedicated superior anterolateral 2-cm incision starting just lateral to the proximal pole of the patella. This specific superior approach is critical for identifying the superolateral geniculate vessel.
- Retinacular Division: Using Metcalf-type scissors, extend the retinacular release distally to the level of the tibial tuberosity.
- Proximal Extension: Carefully extend the release proximally to the superolateral edge of the patella.
- Vastus Lateralis Management: Release only the lateral third of the vastus lateralis tendon. Extend this release obliquely, strictly in line with the vastus lateralis muscle fibers superiorly and laterally. Over-release of the vastus lateralis can lead to catastrophic quadriceps weakness and iatrogenic medial instability.
- Capsular Release: Release the lateral capsule down to, but preserving where possible, the underlying synovium to maintain a barrier against intra-articular bleeding.
⚠️ Surgical Warning: Hemarthrosis Prevention
The most common complication of lateral release is a massive postoperative hemarthrosis. To prevent this, utilize the 2-cm superior anterolateral incision to directly visualize and meticulously coagulate the superolateral genicular artery. Do not rely solely on arthroscopic electrocautery, as the vessel often retracts into the extra-articular soft tissues.
Closure and Dressing
- Place an intra-articular closed-suction drain to evacuate residual hematoma.
- Apply a compression-type Jones dressing incorporating a reinforced lateral patellar pad to mechanically compress the lateral dead space and prevent hematoma accumulation.
SURGICAL TECHNIQUE: MINI-OPEN MEDIAL REEFING (NAM AND KARZEL)
When lateral release alone is insufficient due to medial incompetence, the Nam and Karzel mini-open medial reefing technique provides an anatomic, robust imbrication of the medial structures.
Approach and Tissue Preparation
- Incision: Make a 4-cm longitudinal incision starting at the level of the superior pole of the patella, positioned 2 cm medial and parallel to the medial border of the patella, extending distally.
- Dissection: Carry the dissection sharply down through the subcutaneous tissues to expose the extensor mechanism.
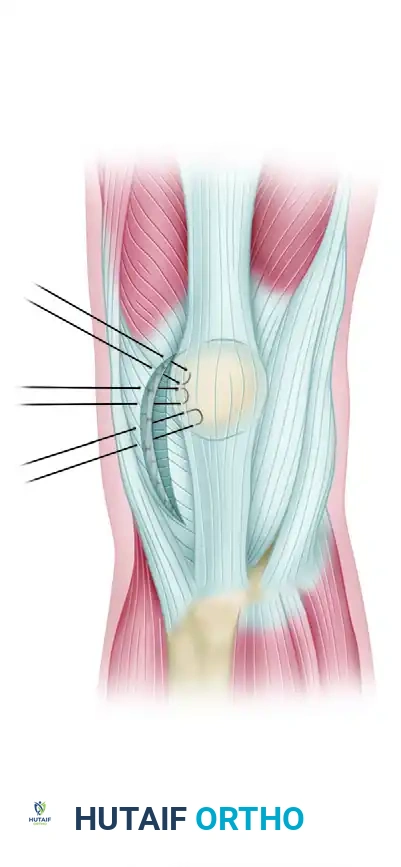
- Tissue Identification: Identify the vastus medialis and the medial retinaculum. Carefully inspect these structures for any areas of traumatic detachment or interstitial tearing.
- Integrity Assessment: Grasp the medial structures with a Kocher clamp and manually pull them laterally. This maneuver assesses the integrity of the tissue at the adductor tubercle attachment site (the femoral origin of the MPFL).
- Synovial Preservation: Continue lateral advancement toward the patella. Carefully incise the vastus medialis and medial retinaculum along the medial border of the patella down to, but not through, the level of the synovium. Preserving the synovium prevents intra-articular extravasation of extra-articular hematoma.
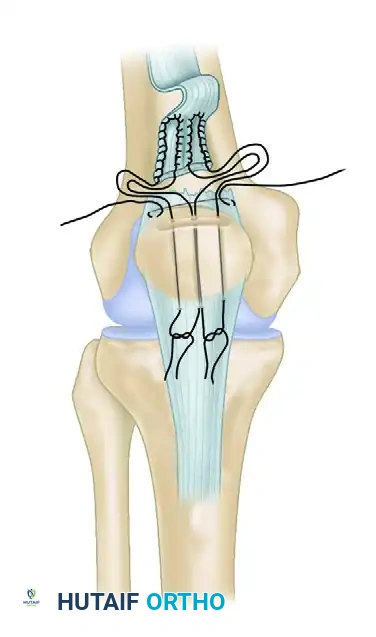
Suture Placement and Imbrication
- Mattress Sutures: Using heavy, non-absorbable braided sutures (e.g., No. 2 Ethibond; Ethicon Inc, Johnson & Johnson, Somerville, NJ), advance the medial retinaculum to the medial border of the patella.
- Configuration: Place at least four horizontal mattress sutures to ensure a broad, secure area of tissue imbrication. The mattress configuration prevents tissue pull-through under the high tensile loads of the extensor mechanism.
Kinematic Assessment and Fixation
- Trial Tensioning: Before the sutures are permanently tied, temporarily tension them and take the knee through a full range of motion.
- Tracking Verification: Ensure congruent tracking of the patella within the trochlear groove. The knee must be able to achieve at least 90 degrees of flexion without excessive tension on the medial repair.
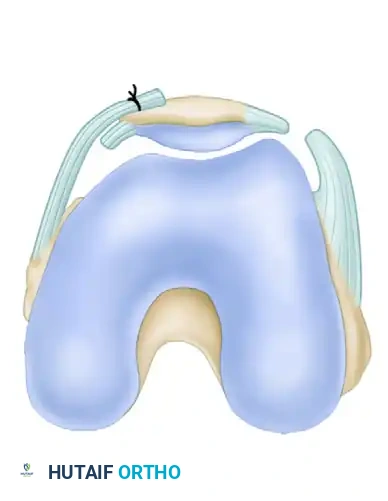
- Arthroscopic Confirmation: Reintroduce the arthroscope into the inferolateral portal. Directly visualize the patellofemoral articulation to confirm the centralization of the patella within the trochlear groove. Increase or decrease the suture tension as necessary based on this direct visual feedback.
- Final Fixation: Tie the sutures securely with the knee held in full extension. Closing in extension prevents over-constraining the medial compartment, which could lead to loss of flexion or elevated patellofemoral contact pressures.
- Closure: Close the subcutaneous tissues and skin in a standard, layered fashion.
SURGICAL TECHNIQUE: MPFL RECONSTRUCTION
For patients with chronic instability, a Q angle of less than 20 degrees, or an extensively damaged MPFL that cannot be primarily reefed, formal reconstruction using a semitendinosus hamstring tendon graft is indicated.
Graft Harvest and Preparation
- Harvest: Harvest the ipsilateral semitendinosus tendon using a standard open tendon stripper technique.
- Preparation: Whipstitch both ends of the graft using high-strength non-absorbable suture. Double the graft to create a robust construct.
Femoral and Patellar Fixation
- Femoral Site: Make a 3-cm incision over the site of the MPFL femoral origin (Schöttle's point), located between the adductor tubercle and the medial epicondyle, as confirmed by preoperative MRI and intraoperative fluoroscopy.
- Direct Repair (Alternative): If the MRI shows an incompetent ligament with damage strictly limited to the femoral attachment, it can occasionally be repaired directly to the bone and reinforced using a slip of the adductor magnus tendon.
- Reconstruction: For full reconstruction, drill a femoral socket at the physiometric point.
- Patellar Fixation: Create two transverse drill holes or use suture anchors along the proximal half of the medial patellar border. Pass the free ends of the doubled graft into the patellar fixation sites.
💡 Clinical Pearl: Isometry and Tensioning
Numerous techniques exist for MPFL reconstruction, but the unifying principle is achieving a physiometric position. Confirm landmarks via palpation and fluoroscopic imaging. Test for isometry by temporarily fixing the graft and cycling the knee. The graft should be tensioned at 30 degrees of flexion with only enough force to eliminate lateral laxity (typically 2-10 Newtons).
Over-tensioning is the most common technical error in MPFL reconstruction. It results in medial patellofemoral arthrosis, severe pain, and a mechanical loss of knee flexion. A properly tensioned graft acts as a check-rein, not a dynamic medializer.
POSTOPERATIVE CARE AND REHABILITATION
A meticulously executed surgery can be easily undone by an inappropriate rehabilitation protocol. The postoperative care must balance tissue protection with the prevention of arthrofibrosis.
Phase 1: Protection and Healing (Weeks 0-2)
- Drain Management: The intra-articular drain (if used during the open lateral release) is removed after 24 hours.
- Immobilization: A knee immobilizer or hinged knee brace locked in full extension is used for approximately 48 hours to reduce initial swelling and protect the medial repair.
- Weight Bearing: The patient is allowed to bear weight as tolerated (WBAT) while locked in the knee immobilizer.
- Early Motion: After 48 hours, the immobilizer is unlocked for seated, passive range-of-motion (ROM) exercises (0 to 90 degrees) to prevent intra-articular adhesions.
Phase 2: Early Strengthening (Weeks 2-6)
- Brace Weaning: At 2 to 3 weeks postoperatively, the immobilizer is gradually discontinued as quadriceps control improves.
- Physical Therapy: A formal physical therapy program is initiated.
- Exercises: Begin with straight-leg raises (in the brace initially to prevent extensor lag) and progress to gentle, closed-chain strengthening exercises (e.g., mini-squats, leg presses limited to 0-45 degrees of flexion). Open-chain knee extensions are strictly avoided to prevent excessive shear forces on the patellofemoral joint and the medial repair.
Phase 3: Advanced Strengthening and Return to Play (Weeks 6-16+)
- Progression: Continue to advance closed-chain strengthening, proprioception, and core stability exercises.
- Functional Milestones: Patients must achieve full, painless range of motion and symmetric quadriceps strength (at least 85-90% of the contralateral limb on isokinetic testing).
- Return to Sports: Patients are typically allowed to return to unrestricted sports participation at approximately 4 months postoperatively, provided all functional criteria are met and symptoms have fully resolved.
COMPLICATIONS AND MANAGEMENT
While highly successful when indicated, these procedures carry specific risks:
1. Hemarthrosis: As emphasized, meticulous hemostasis of the superolateral genicular artery is paramount. If a massive hemarthrosis occurs, early aspiration may be required to prevent capsular distension and subsequent quadriceps inhibition.
2. Iatrogenic Medial Subluxation: Caused by an over-aggressive lateral release (violating the vastus lateralis tendon excessively). This is a devastating complication requiring complex lateral retinacular reconstruction.
3. Loss of Flexion: Often due to over-tensioning of the medial reefing or MPFL graft. If aggressive physical therapy fails, arthroscopic lysis of adhesions and potential graft release may be necessary.
4. Recurrent Instability: Usually stems from failing to address underlying bony abnormalities (e.g., severe trochlear dysplasia or a TT-TG distance >20 mm, which would require a concurrent tibial tubercle osteotomy). Careful preoperative patient selection is the ultimate safeguard against recurrence.
You Might Also Like