Operative Management of Quadriceps Tendon Ruptures and Hamstring Autograft Augmentation
Key Takeaway
Acute quadriceps tendon ruptures require prompt surgical intervention to restore the extensor mechanism. This comprehensive guide details the biomechanics, indications, and step-by-step surgical techniques for primary repair using transosseous tunnels or suture anchors. Furthermore, it explores the Mandelbaum, Bartolozzi, and Carney hamstring autograft augmentation technique for complex or neglected ruptures, providing orthopedic surgeons with evidence-based protocols to optimize patient outcomes and minimize postoperative complications.
BIOMECHANICS AND PATHOANATOMY OF THE EXTENSOR MECHANISM
The extensor mechanism of the knee is a complex dynamic and static stabilizing structure, primarily comprising the quadriceps muscle group, the quadriceps tendon, the patella, the patellar retinaculum, and the patellar tendon. Ruptures of the tendon of the quadriceps femoris muscle represent a catastrophic failure of this mechanism, leading to profound functional impairment.
Acute ruptures of the quadriceps tendon generally result from a violent, eccentric contraction of the extensor mechanism against a sudden, overwhelming load of body weight. The classic mechanism of injury involves a patient stumbling or falling with the foot firmly planted and the knee in a flexed position.
The Hypovascular Zone
Understanding the vascular anatomy of the quadriceps tendon is paramount for both comprehending the etiology of ruptures and optimizing surgical repair.
Clinical Pearl: Cadaveric microangiographic studies have consistently identified a critical hypovascular zone within the quadriceps tendon, located approximately 1 to 2 cm proximal to the superior pole of the patella. This watershed area corresponds precisely to the most frequent site of spontaneous ruptures reported in the orthopedic literature.
Demographic and Anatomic Considerations
The anatomic location of the tear often correlates with the patient's age and tissue quality:
* Older Patients (>40 years): The quadriceps tendon usually ruptures transversely directly at the osteotendinous junction. These patients frequently have underlying tendinopathy or systemic risk factors (e.g., end-stage renal disease, diabetes mellitus, hyperparathyroidism, gout, or a history of fluoroquinolone or corticosteroid use).
* Younger Patients: Ruptures are more likely to occur at the mid-tendon or musculotendinous junction and are typically associated with high-energy athletic trauma (e.g., weightlifting, jumping sports).
The rupture often extends deep through the vastus intermedius tendon, which typically tears slightly proximal to the rupture of the rectus femoris tendon. Furthermore, the medial and lateral retinacula are frequently torn to varying degrees, which dictates the extent of extensor lag observed clinically.
CLINICAL EVALUATION AND INDICATIONS FOR TREATMENT
Diagnosis
The diagnosis of a quadriceps tendon rupture is primarily clinical. Patients present with acute knee pain, swelling, and a palpable suprapatellar gap (the "sulcus sign"). The hallmark clinical finding is the inability to initiate or maintain an active straight-leg raise.
Nonoperative Management
Incomplete ruptures can usually be treated nonoperatively. The decision hinges on the extent of the tear, the integrity of the retinaculum, and the patient’s functional demands.
- Indications: Partial tears with an intact extensor mechanism (patient can perform a straight-leg raise against gravity).
- Protocol: Immobilization of the knee in full extension using a cylinder cast or rigid knee immobilizer for 6 weeks. This is followed by protected, progressive range-of-motion (ROM) and strengthening exercises.
- Progression: When robust quadriceps muscle control is regained and the patient can perform a straight-leg raise without an extensor lag or discomfort, the immobilizer is progressively discontinued.
Operative Management
For complete ruptures, operative repair is strictly indicated and should be performed as expeditiously as possible.
Surgical Warning: Delays in operative repair significantly complicate the surgical process and lead to inferior clinical outcomes. Without its distal tendinous insertion intact, the quadriceps apparatus begins to retract proximally within the first few days after injury. After 72 hours, muscle retraction and tissue edema can make anatomic apposition of the torn tendon ends exceedingly difficult, thereby increasing tension on the suture line and elevating the risk of postoperative gap formation or re-rupture.
SURGICAL TECHNIQUE: ACUTE QUADRICEPS TENDON REPAIR
Although various techniques have been described for the repair of acute quadriceps tendon ruptures, the fundamental goal remains the same: secure, anatomic reattachment of the tendon to the patella to allow for early, protected mobilization. Most traditional techniques involve repairing the tendon with heavy, nonabsorbable sutures passed through longitudinal transosseous holes drilled in the patella. Recently, suture anchors have gained popularity due to their biomechanical equivalence and the avoidance of transpatellar drilling.
Patient Positioning and Preparation
- Place the patient supine on the operating table.
- Apply a high thigh tourniquet.
- Administer prophylactic intravenous antibiotics prior to tourniquet inflation.
- Prep and drape the operative extremity in a standard sterile fashion, allowing for full flexion and extension of the knee.
Surgical Approach and Debridement
- Make a standard anterior midline longitudinal incision, extending from approximately 4 cm proximal to the palpable tendon defect down to the inferior pole of the patella.
- Dissect through the subcutaneous tissues to expose the ruptured quadriceps tendon, the superior pole of the patella, and the medial and lateral retinacular tears.
- Evacuate the fracture hematoma and thoroughly irrigate the joint to remove intra-articular debris.
- Carefully debride the frayed, degenerative edges of the ruptured tendon to healthy, viable tissue.
- Prepare the superior pole of the patella. Use a rongeur or a high-speed burr to decorticate the proximal pole, creating a bleeding cancellous bone trough. This trough is critical for optimizing the biologic environment for tendon-to-bone healing.
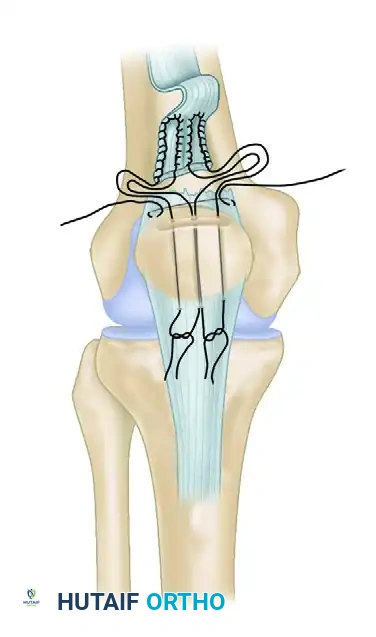
Suture Configuration and Passage (Transosseous Technique)
- Place two or three heavy, nonabsorbable sutures (e.g., #2 or #5 FiberWire or Ethibond) into the proximal tendon stump using a locked, running configuration (such as the Krackow, Bunnell, or Kessler technique). The Krackow technique is preferred for its superior biomechanical grip on longitudinally oriented tendon fibers.
- Ensure that the sutures grasp the rectus femoris, vastus lateralis, and vastus medialis components securely.
- Place separate horizontal mattress sutures in the deeper vastus intermedius stump if it has retracted proximally.
- Drill three parallel, longitudinal transosseous tunnels through the patella, starting from the prepared trough at the superior pole and exiting at the inferior pole. Use a 2.0-mm or 2.5-mm drill bit.
- Using a suture passer or a Beath pin, pass the free ends of the heavy sutures through the transosseous tunnels. The central sutures share the middle tunnel, while the medial and lateral sutures pass through their respective tunnels.
Tensioning, Tying, and Retinacular Repair
- Extend the knee fully.
- Apply distal traction to the quadriceps tendon to pull the tendon stump deeply into the prepared patellar trough.
- Pull the sutures anteriorly through the rectus and tie them securely at the inferior pole of the patella while the tendon is held in strict anatomical position.
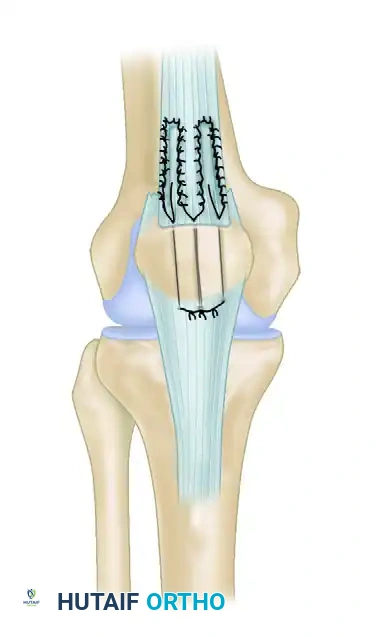
- Assess the tension of the repair. The patella should track centrally, and there should be no gap at the repair site.
- Meticulously repair the medial and lateral retinacular tears using interrupted #1 or #0 absorbable sutures. This step is vital for restoring the dynamic tracking of the patella and reinforcing the primary repair.
- If the tissue quality is exceptionally poor, or if the repair is under undue tension, consider reinforcement. The repair can be protected by a circumferential cerclage wire, strong nonabsorbable sutures, or a Bunnell pull-out wire routed through the medial and lateral retinaculum.
HAMSTRING AUTOGRAFT AUGMENTATION (MANDELBAUM, BARTOLOZZI, AND CARNEY)
In cases of neglected ruptures, chronic tears, or severe tendinopathy where primary end-to-end repair is impossible or biomechanically insufficient, tissue augmentation is required. The technique described by Mandelbaum, Bartolozzi, and Carney utilizes autologous semitendinosus and gracilis tendons to bridge defects and biologically augment the extensor mechanism.
Indications for Augmentation
- Chronic/neglected quadriceps tendon ruptures (>3-4 weeks old).
- Severe tendon retraction that cannot be mobilized despite extensive soft tissue releases.
- Revision surgery for failed primary repairs.
- Systemic connective tissue disorders resulting in friable, non-viable tendon edges.
Step-by-Step Surgical Technique
1. Approach and Joint Preparation
- Make an extensile anterior midline approach extending from the distal third of the thigh to the tibial tubercle.
- Perform a medial arthrotomy to allow for thorough inspection of the joint.
- Perform meticulous lysis of intra-articular and suprapatellar adhesions, which are universally present in chronic cases and restrict patellar mobility.
2. Tendon Mobilization and Realignment
- To address the contracted extensor mechanism, make a Z-lengthening incision in the quadriceps tendon and a corresponding Z-shortening incision through the patellar tendon.
- Crucial Step: Use extremely careful dissection to preserve the vascular pedicle in both the proximal and distal flaps. Ischemia of these flaps will lead to catastrophic necrosis and failure of the reconstruction.
- Place traction sutures in the mobilized tendon ends.
- Obtain an intraoperative anteroposterior (AP) and lateral radiograph. Compare these images with preoperative films of the uninvolved contralateral extremity to determine the appropriate, anatomic patellar height (avoiding iatrogenic patella alta or infera).
- Once a satisfactory position and patellar height are obtained, place multiple heavy absorbable sutures in the quadriceps and patellar tendons to temporarily secure the repair.
3. Hamstring Graft Harvest
- Expose the distal insertion of the pes anserinus on the anteromedial proximal tibia.
- Incise the sartorial fascia and identify the semitendinosus and gracilis tendons.
- Release the accessory bands (vincula) of the semitendinosus to prevent premature amputation of the graft.
- Using an open-ended tendon stripper, harvest the semitendinosus and gracilis tendons sequentially.
- Prepare the grafts on a back table by stripping residual muscle belly and suturing the two tendons together with multiple interrupted absorbable sutures to create a robust, unified graft complex.
4. Graft Routing and Fixation
- Create a transverse osseous tunnel through the mid-portion of the patella using a 4.5-mm or 5.0-mm cannulated drill over a guide pin. Ensure the tunnel is strictly in the coronal plane to avoid violating the articular surface.
- Create a second transverse osseous tunnel through the tibial tuberosity.
- Pass the unified hamstring graft through the transverse hole in the patella and then route it distally through the transverse hole in the tibial tuberosity in a figure-of-eight fashion. This configuration provides exceptional biomechanical stability and acts as an internal splint for the healing extensor mechanism.
- Tension the graft with the knee in full extension.
- Use running interlocking sutures, as described by Krackow, Thomas, and Jones, to suture the hamstring tendon graft to itself at the crossover points of the figure-of-eight.
- Tack the hamstring tendons securely to the underlying native patellar tendon and quadriceps tendon using multiple interrupted nonabsorbable sutures.
- Thoroughly irrigate the wound, achieve hemostasis, and close the retinaculum, subcutaneous tissue, and skin in a layered fashion.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative rehabilitation protocol must balance the need to protect the fragile surgical repair with the necessity of preventing arthrofibrosis. The protocol for an acute repair and a hamstring-augmented reconstruction follows a similar phased trajectory, though augmented or chronic repairs may require a slightly more conservative progression.
Phase I: Maximum Protection (Weeks 0 to 2)
- Immobilization: The knee is locked in full extension in a hinged knee brace or cylinder cast immediately postoperatively.
- Weight-Bearing: Weight-bearing as tolerated (WBAT) with the knee locked in extension using crutches.
- Exercises: Isometric quadriceps sets, ankle pumps, and straight-leg raises (only if the brace is locked in extension). Active knee flexion is strictly prohibited to prevent tension on the repair.
Phase II: Early Controlled Motion (Weeks 2 to 6)
- Immobilization: The hinged knee brace remains locked in extension for ambulation.
- Range of Motion: Begin passive and active-assisted knee flexion. The brace is unlocked for ROM exercises.
- Weeks 2-4: Flexion limited to 0° - 45°.
- Weeks 4-6: Flexion gradually progressed to 0° - 90°.
- Exercises: Continue isometric strengthening. Begin gentle multi-angle isometrics.
Pitfall: Pushing flexion past 90 degrees before 6 weeks places excessive strain on the healing osteotendinous junction and is a primary cause of early gap formation or catastrophic re-rupture.
Phase III: Strengthening and Progression (Weeks 6 to 12)
- Immobilization: The brace is gradually unlocked for ambulation as quadriceps control improves. Once the patient can perform a straight-leg raise without an extensor lag, the brace can be discontinued.
- Range of Motion: Progress to full, symmetric active and passive ROM.
- Exercises: Initiate closed kinetic chain exercises (e.g., mini-squats, leg presses limited to 0°-45°). Begin stationary cycling for ROM and light endurance. Avoid open kinetic chain knee extension against resistance.
Phase IV: Return to Activity (Months 3 to 6+)
- Exercises: Advance closed kinetic chain strengthening. Initiate proprioceptive training and functional activities.
- Return to Sport: Return to heavy manual labor or high-impact sports is typically delayed until 6 months postoperatively, contingent upon the patient achieving at least 85-90% quadriceps strength compared to the contralateral limb and demonstrating no extensor lag.
COMPLICATIONS
Orthopedic surgeons must be vigilant regarding potential complications following extensor mechanism reconstruction:
1. Arthrofibrosis and Stiffness: The most common complication. Loss of terminal flexion is frequent, particularly in delayed reconstructions or augmented repairs. Aggressive, protocol-driven physical therapy is the primary prevention.
2. Re-rupture: Occurs in 1% to 2% of acute repairs, usually due to patient non-compliance, premature aggressive physical therapy, or failure to recognize poor tissue quality intraoperatively.
3. Extensor Lag: A residual extensor lag of 5° to 10° may persist, especially if the retinacular repair was inadequate or if the tendon healed in an elongated position.
4. Infection: Superficial and deep surgical site infections require prompt recognition, aggressive antibiotic therapy, and potential surgical debridement to protect the repair and the joint space.
5. Patellofemoral Pain: Altered patellar kinematics, especially if patellar height was not anatomically restored during a Z-lengthening/shortening procedure, can lead to chronic anterior knee pain.
You Might Also Like