Thumb Carpometacarpal Arthrodesis

Introduction and Epidemiology
Osteoarthritis of the trapeziometacarpal (thumb carpometacarpal or CMC) joint is a pervasive and debilitating condition, ranking as the second most common site of degenerative joint disease in the hand, superseded only by the distal interphalangeal (DIP) joint. However, due to the thumb's indispensable role in global hand function—contributing up to 40% of overall hand capability—arthrosis at the CMC joint is disproportionately disabling. Patients typically present with profound, localized pain at the base of the thumb, accompanied by a precipitous decline in both power grip and key pinch strength.
The surgical management of symptomatic thumb CMC joint arthrosis is highly nuanced. The algorithm is dictated by a constellation of factors, including the patient's chronological and physiological age, occupational demands, medical comorbidities, and the radiographic stage of degeneration. Since its initial description by Muller in 1949, thumb CMC arthrodesis has maintained a pivotal role in the orthopedic surgeon’s armamentarium. While the intervening decades have seen a surge in the popularity of excisional arthroplasty techniques—such as ligament reconstruction and tendon interposition (LRTI), hematoma distraction arthroplasty, and suspensionplasty—arthrodesis remains the undisputed gold standard for a specific demographic.
Thumb carpometacarpal arthrodesis is the procedure of choice for younger, high-demand patients (typically under 55 years of age) with moderate to advanced thumb CMC degeneration, whether primary or posttraumatic. For heavy manual laborers, mechanics, and patients anticipating high-load pinch and power grip requirements, arthrodesis provides superior long-term functional stability and preservation of peak pinch strength compared to excisional arthroplasty. This superior functional profile is contingent upon achieving solid osseous union and ensuring the adjacent joints (scaphotrapezial trapezoidal [STT] and metacarpophalangeal [MCP]) remain free of advanced degenerative disease.
Surgical Anatomy and Biomechanics
Osteology and Articular Geometry
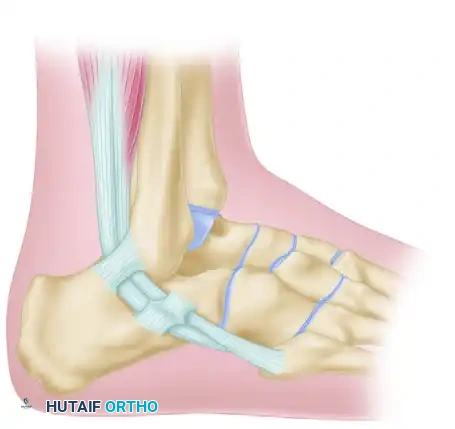
The thumb CMC joint is a highly specialized biconcave-convex, or "saddle," joint. This unique articular geometry permits complex, multiplanar kinematics, facilitating motion in three distinct planes: flexion-extension, abduction-adduction, and pronation-supination. The distal articular surface of the trapezium presents a concave geometry in the radioulnar plane and a convex geometry in the dorsovolar plane. These surfaces articulate with the perfectly reciprocal surfaces of the first metacarpal base.
This multiplanar excursion is the biomechanical foundation for power grip, key pinch, opposition, and delicate precision handling. However, the joint relies on an inherent lack of osseous constraint to achieve this vast range of motion. Consequently, the trapeziometacarpal articulation places an immense functional demand on the surrounding capsuloligamentous envelope to maintain dynamic stability under load.

Ligamentous Stabilizers
Given the minimal osseous constraint of the saddle joint, the ligamentous structures are the primary arbiters of stability. Anatomical studies have identified up to sixteen distinct ligaments surrounding the thumb CMC joint. Of these, seven are considered the primary stabilizers of the trapeziometacarpal articulation:
* Superficial anterior oblique ligament (sAOL)
* Deep anterior oblique ligament (dAOL)
* Dorsoradial ligament (DRL)
* Posterior oblique ligament (POL)
* Ulnar collateral ligament (UCL)
* Intermetacarpal ligament (IML)
* Dorsal intermetacarpal ligament (DIML)
The remaining capsuloligamentous structures stabilize the trapezium to the scaphoid, trapezoid, and second metacarpal, creating a stable osseous foundation for the thumb ray.
Historically, the anterior (palmar) oblique ligament—often referred to as the "beak ligament"—was erroneously considered the primary stabilizing restraint of the thumb. However, seminal biomechanical investigations by Pellegrini, Bettinger, and others have definitively established that the dorsal ligament complex (comprising the dorsoradial and posterior oblique ligaments) is the thickest, strongest, and most critical stabilizer of the thumb CMC joint. The dorsal complex acts as the primary restraint against dorsal subluxation of the metacarpal base during power grip or pinch. It also prevents the volar beak of the thumb metacarpal from disengaging from the volar recess of the trapezium. Conversely, the volar beak ligament is completely lax during opposition and only becomes taut in the retropulsed "hitchhiker" position.

Pathogenesis of Degeneration
The pathogenesis of CMC joint arthrosis is a multifactorial cascade involving biochemical, biomechanical, and genetic components. Epidemiologically, osteoarthritis of the thumb CMC joint is significantly more prevalent in post-menopausal females. This demographic distribution strongly suggests a hormonal influence on ligamentous laxity and cartilage homeostasis, predisposing the joint to micro-instability.
Arthritic degeneration characteristically initiates on the palmar aspect of the thumb metacarpal and the corresponding trapezium. This predictable wear pattern is a direct consequence of the immense compressive and rotational shear forces concentrated in the volar recess of the trapezium during power pinch and grip. Biomechanical models demonstrate that joint reaction forces (JRF) at the CMC joint can exceed 13 times the applied pinch force at the thumb tip.
Over decades of repetitive cyclical loading, the articular cartilage of the volar beak is subjected to critical shear stress, leading to eburnation. Concurrently, subtle instability develops during the "screw-home-torque" rotation intrinsic to thumb opposition. As the disease progresses and the critical dorsal ligament complex attenuates, the metacarpal inevitably subluxates dorsally and radially. This alters the instantaneous center of rotation, leading to global joint space narrowing, osteophyte formation, and eventual pantrapezial arthrosis.
Posttraumatic osteoarthrosis can also develop rapidly following direct disruption of the articular cartilage. Intra-articular fractures involving the base of the thumb metacarpal (e.g., Bennett or Rolando fractures) or the trapezium dramatically accelerate the timeline of arthrosis. This is driven by acute chondrocyte necrosis at the time of injury, compounded by residual articular incongruity and altered contact mechanics. While meticulous open reduction and internal fixation (ORIF) mitigates this risk, it rarely eliminates it entirely.
Indications and Contraindications
Rigorous patient selection is the single most critical determinant of clinical success in thumb CMC arthrodesis. The archetypal candidate is a younger patient (typically < 55 years old) with high functional and occupational demands (e.g., heavy manual laborers, carpenters, mechanics) who presents with isolated, symptomatic Eaton-Littler Stage II or III osteoarthritis or posttraumatic arthrosis.
A comprehensive clinical and radiographic evaluation must be performed to rule out concurrent pathology. Crucially, the presence of scaphotrapezial trapezoidal (STT) joint arthritis is an absolute contraindication to isolated CMC arthrodesis. Fusing the CMC joint inherently alters the kinematic chain of the thumb ray, significantly increasing mechanical stress and load transfer across the adjacent STT joint. Consequently, pre-existing STT arthrosis will rapidly become symptomatic postoperatively, leading to clinical failure and the necessity for revision surgery (e.g., pantrapezial arthroplasty).
Operative vs Non Operative Management
| Management Strategy | Indications | Contraindications |
|---|---|---|
| Non-Operative | Mild to moderate pain, Eaton Stage I-II, low functional demands, medically unfit for surgery. Modalities include NSAIDs, rigid orthosis, and intra-articular corticosteroid injections. | Intractable pain failing conservative measures, progressive functional decline, severe instability, advanced deformity. |
| Thumb CMC Arthrodesis | High-demand laborers, young patients (<55), posttraumatic arthrosis, isolated Eaton Stage II/III OA. | STT joint arthritis, Eaton Stage IV OA, inflammatory arthropathies (e.g., Rheumatoid Arthritis), severe MCP hyperextension (>30 degrees) without concurrent stabilization, elderly/low-demand patients. |
| Excisional Arthroplasty (LRTI) | Older patients (>55), lower functional demands, Eaton Stage III/IV OA, concurrent STT arthritis (managed with partial or complete trapezoidectomy). | Young, heavy laborers requiring maximum power grip/pinch, patients requiring absolute length preservation to prevent abutment. |
Pre Operative Planning and Patient Positioning
Clinical and Radiographic Evaluation
Preoperative clinical evaluation must meticulously document thumb range of motion, grip strength, and key pinch strength using a dynamometer. The thumb metacarpophalangeal (MCP) joint demands careful scrutiny for compensatory hyperextension, a common consequence of chronic CMC volar flexion and adduction contracture. If MCP hyperextension exceeds 30 degrees, concurrent MCP joint volar capsulodesis, EPB transfer, or MCP arthrodesis must be incorporated into the surgical plan. Failure to address this will result in a debilitating zigzag deformity postoperatively, neutralizing the functional gains of the CMC fusion.
Standard radiographic evaluation mandates a true anteroposterior (AP) view of the thumb (Robert's view), a true lateral view, and stress views to quantify dynamic subluxation. A Bett's view may also be utilized to better profile the STT joint. The Eaton-Littler classification remains the standard for radiographic staging:
* Stage I: Normal articular contours, slight joint space widening (indicative of effusion or ligamentous laxity).
* Stage II: Joint space narrowing, presence of osteophytes < 2mm.
* Stage III: Significant joint space destruction, subchondral sclerotic changes, cystic formation, and osteophytes > 2mm.
* Stage IV: Pantrapezial arthritis involving the STT joint (absolute contraindication for isolated CMC fusion).

Fixation Selection
The optimal fixation construct for CMC arthrodesis remains a subject of ongoing academic debate. Options include Kirschner wires (K-wires), intra-osseous wiring, lag screws, locking plates, and shape-memory staples. Historically, K-wires were the standard; however, they are biomechanically inferior and associated with unacceptably high rates of nonunion and pin tract infections.
Modern surgical techniques heavily favor either low-profile titanium locking plates or crossed headless compression screws (HCS). Locking plates provide superior biomechanical rigidity, which is highly advantageous for achieving primary bone healing and permitting earlier postoperative mobilization. However, they carry a higher risk of symptomatic hardware prominence necessitating secondary removal. Crossed HCS constructs offer excellent compression and a zero-profile footprint, minimizing soft tissue irritation, but require precise trajectory planning to avoid STT joint penetration.

Patient Positioning
The patient is positioned supine with the operative extremity extended onto a radiolucent hand table. A well-padded proximal arm tourniquet is applied to ensure a bloodless field. Intraoperative fluoroscopy (mini C-arm) is positioned parallel to the hand table, allowing the surgeon to obtain orthogonal views of the thumb ray via simple pronation/supination of the arm, without moving the surgical field or compromising sterility. Regional anesthesia (supraclavicular or axillary brachial plexus block) is highly preferred, supplemented with monitored anesthesia care (MAC) or general anesthesia depending on patient anxiety and anticipated surgical duration.
Detailed Surgical Approach and Technique
Incision and Superficial Dissection
The CMC joint is typically accessed via a standard Wagner approach or a dorsal-radial incision. The dorsal-radial incision is frequently favored as it provides excellent, extensile exposure to the CMC joint while mitigating the risk of painful palmar scarring in the glabrous skin. A 4 to 5 cm longitudinal incision is made centered over the CMC joint, curving slightly volar at its proximal extent.
Meticulous superficial dissection is paramount. The terminal branches of the superficial branch of the radial nerve (SBRN) and the lateral antebrachial cutaneous nerve (LABCN) are highly variable in this anatomical zone. These neural structures must be carefully identified using blunt dissection, mobilized with vessel loops, and gently retracted. Iatrogenic injury or excessive traction on the SBRN is a devastating complication that can induce Wartenberg's syndrome or a debilitating neuroma, often completely overshadowing the functional benefits of a successful osseous fusion.
Deep Dissection and Arthrotomy
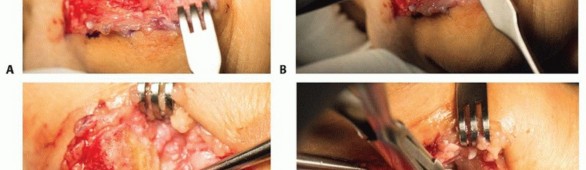
Upon incising the deep fascia, the first dorsal compartment is identified. The interval between the abductor pollicis longus (APL) and the extensor pollicis brevis (EPB) is carefully developed. The APL is retracted volarly, and the EPB is retracted dorsally. The radial artery, which courses dorsally over the scaphoid and trapezium, must be protected during the proximal extent of the dissection.
The dorsal capsule of the trapeziometacarpal joint is then identified and cleared of overlying soft tissue. A longitudinal or T-shaped capsulotomy is performed, preserving robust capsular flaps for subsequent closure. Subperiosteal elevation is carried out along the base of the first metacarpal and the distal aspect of the trapezium to achieve circumferential exposure of the articular surfaces. Hohmann or Sen retractor placement must be precise to avoid excessive tension on the adjacent neurovascular structures.

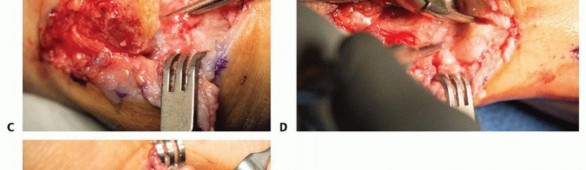
Joint Preparation
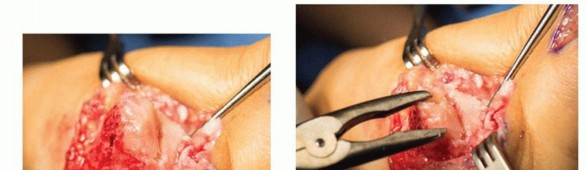
Thorough and aggressive joint preparation is the most critical technical variable in preventing nonunion. All sclerotic, eburnated cartilage must be entirely excised down to healthy, bleeding subchondral bone. Two primary techniques exist for joint surface preparation:
1. Planar Resection: An oscillating saw is utilized to make flat, parallel cuts on the metacarpal base and the distal trapezium. While this provides excellent, broad cancellous bone contact, it invariably sacrifices joint length and limits the surgeon's ability to fine-tune the final fusion angle in multiple planes.
2. Cup and Cone Reaming: Hand reamers or a high-speed burr (under copious cold saline irrigation to prevent thermal necrosis) are utilized to create a concave "cup" surface on the trapezium and a convex "cone" on the metacarpal base. This technique is biomechanically superior; it maximizes the surface area for osteogenesis, preserves thumb ray length, and acts as a ball-and-socket, allowing for multiplanar micro-adjustments during final positioning.
Regardless of the chosen technique, the exposed subchondral bone should be aggressively shingled, fish-scaled, or fenestrated using a 1.0mm K-wire or a small drill bit. This promotes marrow egress, introducing osteoprogenitor cells and osteoinductive factors into the fusion site.

Positioning the Arthrodesis
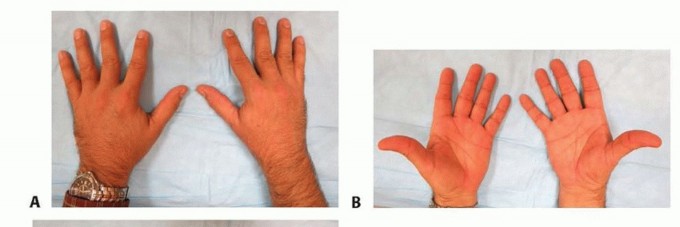
Achieving the precise fusion angle is paramount for maximizing postoperative function. Malpositioning can severely limit opposition (preventing pulp-to-pulp pinch) or prevent the thumb from clearing the palm during power grip. The optimal, biomechanically proven position for thumb CMC arthrodesis is:
* 30 to 40 degrees of palmar abduction
* 10 to 15 degrees of radial abduction
* 15 to 20 degrees of pronation
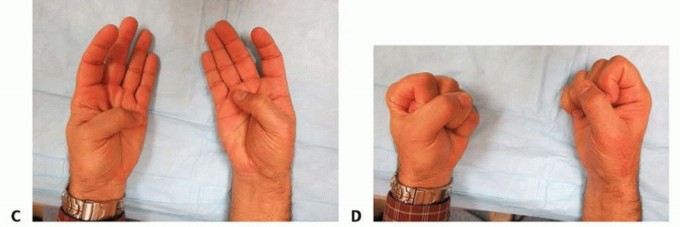
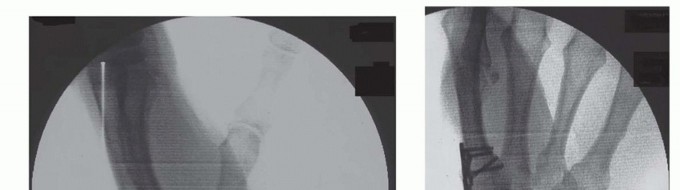
Intraoperatively, this alignment is verified clinically by the "fist position" check. When the fingers are passively flexed into a fist, the pulp of the thumb should rest comfortably against the radial aspect of the proximal interphalangeal (PIP) joint of the index finger. Once the optimal spatial orientation is achieved, the joint is provisionally stabilized with one or two 0.045-inch K-wires driven from the metacarpal into the trapezium. Fluoroscopy is utilized to confirm anatomic alignment, ensure proper hardware trajectory, and verify the absence of joint gapping.
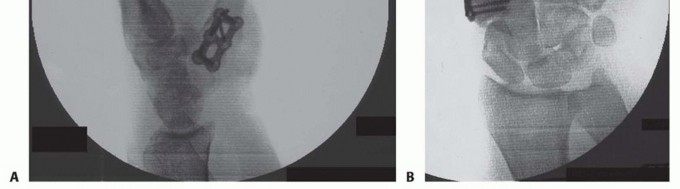
Internal Fixation
If a plate construct is selected, a low-profile titanium locking plate (typically a 5-hole or 6-hole T-plate, Y-plate, or straight plate) is contoured to the dorsal-radial aspect of the fusion mass. The plate must sit completely flush against the bone to minimize tendon irritation. Cortical or locking screws are placed into the trapezium and the metacarpal. It is absolutely critical to utilize fluoroscopy to ensure that the proximal screws do not penetrate the STT joint, which would rapidly induce secondary arthrosis.
If screw fixation is utilized, two headless compression screws (typically 2.4mm or 3.0mm) are placed in a crossed configuration. The first screw is usually directed from the dorsal-radial base of the metacarpal, crossing the joint space, and anchoring into the volar-ulnar aspect of the trapezium. The second screw is placed in a divergent trajectory to provide maximum rotational stability and uniform compression across the arthrodesis site.
Closure
Following final fluoroscopic verification of hardware placement and fusion site compression, the tourniquet is deflated, and meticulous hemostasis is obtained. The wound is copiously irrigated. The capsule is closed over the hardware if possible, utilizing an absorbable suture (e.g., 3-0 Vicryl) to provide a soft tissue buffer for the overlying APL and EPB tendons. The extensor retinaculum is repaired if it was divided during the approach. The skin is closed with non-absorbable monofilament sutures (e.g., 4-0 or 5-0 Nylon), and a sterile compressive dressing is applied, followed immediately by a rigid volar thumb spica splint.

Complications and Management
While thumb CMC arthrodesis provides excellent functional outcomes in properly selected patients, it is technically demanding and carries a unique complication profile compared to excisional arthroplasty.
Common Complications and Salvage Strategies
| Complication | Incidence | Etiology | Management / Salvage Strategy |
|---|---|---|---|
| Nonunion | 5% - 20% | Inadequate joint preparation, thermal necrosis from aggressive reaming, poor fixation rigidity, patient non-compliance, active tobacco use. | Asymptomatic nonunions (fibrous unions) often require no intervention. Symptomatic nonunions require revision arthrodesis with autologous bone grafting (iliac crest or distal radius) and rigid plate fixation. Alternatively, salvage via conversion to trapeziectomy with LRTI. |
| Hardware Prominence | 10% - 30% | Low-profile soft tissue envelope over the dorsal-radial thumb; utilization of bulky plate constructs. | Hardware removal after definitive radiographic confirmation of solid osseous union (typically > 6 to 9 months post-op). |
| Adjacent Joint Arthrosis | 15% - 25% | Altered kinematics and increased mechanical stress transferred to the STT or MCP joints following rigid CMC fusion. | STT arthrosis may require isolated STT fusion or conversion to pantrapezial excisional arthroplasty. Progressive MCP hyperextension requires volar capsulodesis or MCP arthrodesis. |
| SBRN Neuroma | 2% - 5% | Iatrogenic sharp injury, thermal injury, or excessive traction on the superficial branch of the radial nerve during exposure. | Prevention via meticulous dissection is paramount. Established neuromas require surgical excision, nerve capping, or targeted muscle reinnervation (TMR) / proximal transposition into the brachioradialis muscle belly. |
| Malunion | < 5% | Failure to achieve or maintain the optimal 30-40° palmar abduction, 10-15° radial abduction, and 15-20° pronation. | If functionally limiting (inability to oppose or clear the palm during grip), requires a corrective closing-wedge osteotomy and revision internal fixation. |
Nonunion remains the most frequently cited major complication of CMC arthrodesis. The evolution from K-wire fixation to modern locking plates and crossed compression screws has significantly reduced the nonunion rate, though it remains a substantial risk, particularly in active smokers. Meticulous joint preparation down to bleeding bone, combined with rigid compression, is the most critical surgeon-controlled variable in preventing this complication.
Post Operative Rehabilitation Protocols
Postoperative rehabilitation following CMC arthrodesis requires a delicate balance: maintaining rigid immobilization to facilitate osseous union while preventing stiffness in the adjacent, uninvolved joints of the hand and wrist.
- Phase I (0-2 Weeks): The patient is placed in a rigid, well-padded thumb spica splint in the operating room. Elevation and immediate active range of motion (AROM) of the fingers (MCP, PIP, DIP joints) and the interphalangeal (IP) joint of the thumb are aggressively encouraged to reduce edema and prevent extensor tendon adhesions.
- Phase II (2-6 Weeks): At the first postoperative visit (10-14 days), sutures are removed. The patient is transitioned to a short-arm thumb spica cast or a custom-molded thermoplastic rigid orthosis. Immobilization of the CMC joint is strictly maintained to protect the fixation construct during the early phases of primary bone healing.
- **Phase III (6-
You Might Also Like