Modified Jones Procedure: EHL Transfer & IP Arthrodesis
Key Takeaway
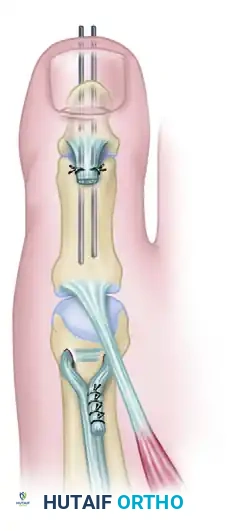
The Modified Jones procedure addresses severe clawing of the great toe, frequently seen in Charcot-Marie-Tooth disease and cavovarus foot deformities. It involves transferring the extensor hallucis longus (EHL) tendon to the first metatarsal neck to elevate a plantarflexed first ray, combined with interphalangeal joint arthrodesis to prevent hallux malleus. This guide details the biomechanical rationale, step-by-step surgical technique, and postoperative protocols for optimal deformity correction.
Introduction and Biomechanical Rationale
The tendon suspension of the first metatarsal combined with interphalangeal (IP) joint arthrodesis—widely recognized as the Modified Jones Procedure—is a cornerstone operation in the reconstructive armamentarium for complex foot deformities. Originally described by Sir Robert Jones for the management of paralytic equinovarus, the modern iteration of this procedure is most frequently deployed in the treatment of Charcot-Marie-Tooth (CMT) disease, poliomyelitis, and other neuromuscular conditions characterized by a cavovarus foot posture and a rigidly plantarflexed first ray.
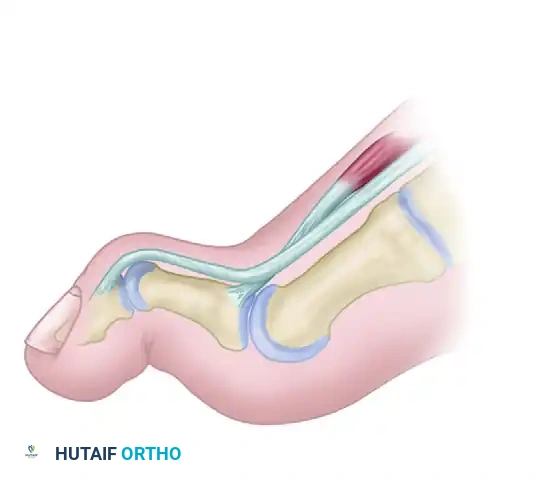
In the setting of a cavovarus foot, weakness of the tibialis anterior muscle leads to compensatory overactivity of the extensor hallucis longus (EHL) in an attempt to maintain ankle dorsiflexion during the swing phase of gait. Because the EHL inserts on the distal phalanx of the hallux, this "extensor overdrive" results in severe hyperextension of the metatarsophalangeal (MTP) joint and secondary flexion of the IP joint, creating a pathognomonic claw toe deformity.
Furthermore, the plantarflexed first ray acts as a mechanical kickstand during the stance phase, driving the hindfoot into a compensatory varus position. By transferring the EHL to the neck of the first metatarsal, the deforming force is eliminated, the first ray is dynamically elevated, and the MTP joint is allowed to relax. Arthrodesis of the IP joint is mandatory to prevent a subsequent hallux malleus (drop toe) deformity once the EHL is detached from the distal phalanx.
Clinical Pearl: The Modified Jones procedure is rarely performed in isolation. It is typically part of an "a la carte" reconstruction for the cavovarus foot, which may include plantar fascia release, first metatarsal basilar dorsiflexion osteotomy, calcaneal osteotomy, and peroneus longus to brevis transfer.
Indications and Patient Selection
Careful patient selection and preoperative clinical evaluation are paramount. The primary indications for the Modified Jones procedure include:
- Neuromuscular Claw Hallux: Driven by EHL overactivity secondary to tibialis anterior weakness (e.g., Charcot-Marie-Tooth disease, stroke, cerebral palsy, poliomyelitis).
- Flexible Plantarflexed First Ray: Where the first ray can be manually reduced to a neutral position. If the first ray is rigidly plantarflexed, a basilar closing wedge osteotomy of the first metatarsal must be performed concomitantly.
- Forefoot Equinovarus: As an adjunctive soft-tissue balancing procedure to elevate the medial column.
- Iatrogenic Hallux Cock-up Deformity: Following over-resection of the metatarsal head or excessive tightening of the dorsal capsule during prior forefoot surgery.
Preoperative Evaluation: The Coleman Block Test
Before committing to a soft-tissue suspension, the surgeon must determine if the hindfoot varus is driven by the plantarflexed first ray (forefoot-driven varus) or if it is a fixed hindfoot deformity. The Coleman Block Test is essential:
1. The patient stands with the lateral border of the foot (heel and lateral rays) on a 1-inch wooden block.
2. The first ray is allowed to drop off the medial edge of the block into plantarflexion.
3. If the hindfoot varus corrects to neutral or valgus, the deformity is forefoot-driven, and elevating the first ray (via EHL transfer and/or osteotomy) will correct the hindfoot. If the hindfoot remains in varus, a concomitant calcaneal osteotomy is required.
Surgical Anatomy and Approaches
A thorough understanding of the dorsal forefoot anatomy is required to execute this procedure without causing iatrogenic injury to adjacent structures.
- Extensor Hallucis Longus (EHL): Originates from the middle half of the anterior fibula and interosseous membrane. It travels under the extensor retinaculum and inserts into the dorsal base of the distal phalanx of the great toe.
- Extensor Hallucis Brevis (EHB): Originates from the dorsal calcaneus and inserts into the dorsal base of the proximal phalanx. The EHB must be meticulously protected during EHL harvest to maintain some active extension of the MTP joint.
- Neurovascular Bundle: The deep peroneal nerve and dorsalis pedis artery run lateral to the EHL tendon over the midfoot and must be protected during the proximal dissection.
Patient Positioning and Preparation
- Positioning: The patient is placed in the supine position on a standard radiolucent operating table. A bump may be placed under the ipsilateral hip to internally rotate the leg to a neutral position, ensuring the patella and foot face directly anteriorly.
- Tourniquet: A pneumatic thigh or calf tourniquet is applied and inflated to 250-300 mmHg after exsanguination with an Esmarch bandage.
- Equipment: Mini C-arm fluoroscopy should be available to verify joint preparation and hardware placement. Have 0.062-inch Kirschner wires (K-wires) and 5/64-inch Steinmann pins available for the arthrodesis.
Step-by-Step Surgical Technique
1. Interphalangeal Joint Exposure and EHL Harvest
The procedure begins distally at the great toe to harvest the EHL tendon and prepare the IP joint for arthrodesis.
- Incision: Expose the interphalangeal joint of the great toe through a dorsal L-shaped incision or a transverse elliptical incision over the dorsal crease of the IP joint.
- Dissection: Carefully retract the flap of skin and subcutaneous tissue medially and proximally. Employ full-thickness flaps to prevent skin edge necrosis, a common complication in dorsal foot incisions.
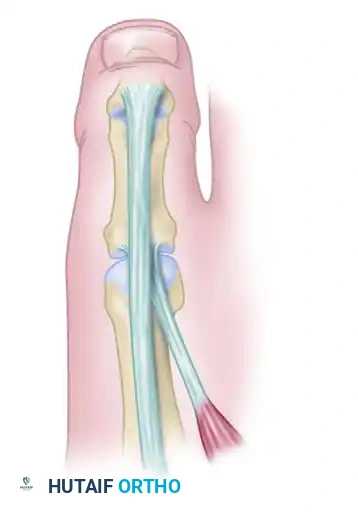
- Tendon Identification: Identify and expose the tendon of the extensor hallucis longus as it crosses the IP joint to insert on the distal phalanx.
- Tendon Transection: Cut the EHL tendon transversely approximately 1 cm proximal to the IP joint.
- Surgical Rationale: Leaving a 1 cm distal stump is critical. This stump will later be sutured to the soft tissues or the EHB over the proximal phalanx to provide additional stability to the arthrodesis site.
2. Interphalangeal Joint Arthrodesis
Once the EHL is transected, the IP joint is fully exposed for preparation.
- Joint Preparation: Sharply incise the dorsal capsule and collateral ligaments to fully plantarflex and open the IP joint.
- Cartilage Excision: Using a microsaw, rongeur, or sharp osteotome, cleanly excise the articular cartilage from both the head of the proximal phalanx and the base of the distal phalanx. Ensure that the subchondral bone is exposed to bleeding cancellous bone to promote fusion.
- Technique Variation: A "cup and cone" reamer system can be used to maintain length and allow for minor angular adjustments, though flat planar cuts are equally effective if parallel.
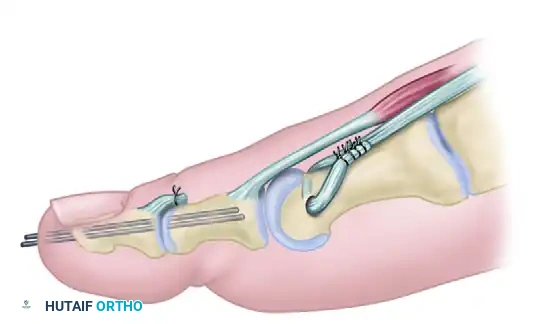
- Fixation: Approximate the joint surfaces in neutral rotation and 0 to 5 degrees of plantarflexion. Insert a 5/64-inch medullary Steinmann pin or two retrograde medullary 0.062-inch Kirschner wires for rigid fixation.
- Retrograde Technique: Drive the K-wire distally through the center of the distal phalanx to exit the tip of the toe just plantar to the nail bed. Reduce the joint, then drive the wire proximally into the medullary canal of the proximal phalanx.
- Wire Management: Clip the wire off just beneath the skin to prevent pin tract infections, or leave it protruding with a protective cap if early removal in the clinic is planned.
Surgical Warning: Avoid driving the K-wire across the MTP joint. The wire should terminate within the proximal phalanx to allow for MTP joint motion postoperatively.
3. Proximal Exposure and Tendon Preparation
Attention is now turned to the first metatarsal to prepare the suspension site.
- Incision: Expose the neck of the first metatarsal through a 2.5-cm dorsomedial longitudinal incision. This incision should extend distally to the proximal extensor skin crease.
- Tendon Retrieval: Identify the proximal stump of the EHL tendon. Pass a curved hemostat from the proximal incision, deep to the extensor retinaculum, to retrieve the EHL tendon from the distal wound. Pull the tendon into the proximal wound.
- Protecting the EHB: Dissect free the extensor hallucis longus tendon, but meticulously identify and protect the short extensor tendon (EHB). The EHB will provide the necessary residual extension to the MTP joint.
- Sheath Excision: Cleanly and carefully excise the sheath of the extensor hallucis longus tendon throughout the length of the proximal incision.
- Surgical Rationale: Removing the sheath prevents postoperative tethering and scarring, ensuring smooth excursion of the tendon and a direct tenodesis effect on the bone.
4. Tendon Suspension to the First Metatarsal
The core biomechanical correction is achieved by anchoring the EHL to the metatarsal neck.
- Bone Tunnel Preparation: Beginning on the inferomedial aspect of the first metatarsal neck, drill a hole transverse to the long axis of the bone. The drill bit should emerge on the dorsolateral aspect of the neck.
- Drill Size: Typically, a 3.2 mm or 3.5 mm drill bit is sufficient, depending on the caliber of the EHL tendon. Ensure the hole is placed centrally in the metatarsal neck to avoid creating a stress riser that could lead to a postoperative fracture.
- Tendon Passage: Place a running locking stitch (e.g., Krackow technique using 0-Vicryl or FiberWire) into the distal end of the EHL tendon. Pass the suture and the tendon through the osseous hole from medial to lateral.
- Tensioning and Fixation:
- Hold the ankle in a strictly neutral position (0 degrees of dorsiflexion).
- Apply upward pressure on the plantar aspect of the first metatarsal head to elevate the first ray to a neutral position relative to the lesser metatarsals.
- With the bone held in this corrected position, pull the EHL tendon taut.
- Suture the tendon to itself with interrupted non-absorbable sutures (e.g., 2-0 Ethibond or FiberWire).
Pitfall: Under-tensioning the EHL transfer will result in recurrent plantarflexion of the first ray and persistent cavovarus deformity. Over-tensioning can lead to a rigid dorsal elevation of the first ray, causing transfer metatarsalgia to the second metatarsal head. Tensioning with the ankle exactly at neutral is the most critical step of the procedure.
5. Final Construct and Closure
- Distal Stump Management: Return to the distal incision. Suture the distal 1-cm stump of the EHL tendon to the soft tissues over the proximal phalanx or directly to the EHB tendon. This reinforces the dorsal capsule and aids in preventing MTP joint subluxation.
- Closure: Irrigate both wounds copiously with sterile saline. Close the subcutaneous tissues with 3-0 absorbable sutures and the skin with 4-0 nylon or staples.
- Immobilization: Apply sterile dressings and a well-padded short-leg walking cast or a rigid posterior splint with the ankle locked in a neutral position.
(Note: The same tendon suspension and arthrodesis procedure can be performed on adjacent lesser toes utilizing the extensor digitorum longus tendons in cases of severe lesser toe clawing, often referred to as the Hibbs procedure.)
Adjunctive Procedures: The Rigid First Ray
The Modified Jones procedure relies on the flexibility of the first tarsometatarsal (TMT) joint. If preoperative assessment or intraoperative examination reveals that the plantarflexed first ray is rigid and cannot be elevated to neutral with manual pressure, soft-tissue suspension alone will fail.
In skeletally mature patients with a rigid deformity, a basilar closing wedge osteotomy of the first metatarsal (dorsiflexion osteotomy) must be performed.
1. A dorsal wedge of bone is removed from the base of the first metatarsal.
2. The osteotomy is closed, elevating the metatarsal head.
3. Fixation is achieved with a dorsal plate or crossed K-wires.
4. If the hallux remains in a clawed position after the osteotomy, the transfer of the EHL to the neck of the first metatarsal and the arthrodesis of the IP joint are then completed to address the dynamic component of the deformity.
Postoperative Care and Rehabilitation
Strict adherence to postoperative protocols is necessary to ensure tendon-to-bone healing and successful IP joint arthrodesis.
- 0 to 3 Weeks:
- The patient is placed in a short-leg cast or rigid splint with the ankle in neutral.
- Walking on crutches is allowed within a few days, but the patient must remain strictly non-weight-bearing on the operative extremity to protect the tendon transfer and arthrodesis site.
- Elevation of the limb is critical to manage edema and promote wound healing.
- At 3 Weeks:
- The patient is seen in the clinic. The initial cast and skin sutures are removed.
- Clinical and radiographic evaluation is performed to check the alignment of the IP joint.
- A new short-leg walking cast or a rigid controlled ankle motion (CAM) boot is applied. The patient may begin progressive partial weight-bearing as tolerated.
- At 6 Weeks:
- The walking cast is removed.
- Radiographs are obtained to confirm consolidation of the IP joint arthrodesis.
- If clinical and radiographic union is evident, the percutaneous Kirschner wires or Steinmann pin are removed in the clinic.
- The patient is transitioned to a supportive stiff-soled shoe.
- Active and passive range-of-motion exercises for the ankle and MTP joints are initiated. Physical therapy focuses on gait retraining and strengthening the transferred EHL to function as an elevator of the first ray.
Complications and Management
While highly effective, the Modified Jones procedure carries specific risks that the orthopedic surgeon must anticipate:
- Nonunion of the IP Joint: Occurs in up to 5-10% of cases. Risk factors include inadequate cartilage resection, poor compression, and early weight-bearing. Asymptomatic nonunions require no intervention. Symptomatic nonunions may require revision arthrodesis with rigid screw fixation and bone grafting.
- Hardware Migration or Infection: Percutaneous K-wires can migrate or become infected. If superficial pin tract infection occurs, oral antibiotics are usually sufficient. If deep infection or loosening occurs, the pins must be removed immediately, and the toe protected in a rigid splint until fusion occurs.
- Transfer Metatarsalgia: Over-elevation of the first metatarsal transfers weight-bearing forces to the lesser metatarsal heads, leading to intractable plantar keratosis and pain. This underscores the importance of tensioning the EHL with the first ray perfectly aligned with the lesser rays.
- Recurrent Deformity: Usually the result of under-tensioning the EHL transfer, failure to recognize a rigid first ray (omitting the basilar osteotomy), or progressive neurological decline in conditions like CMT.
- Skin Necrosis: The dorsal skin of the foot is thin and has a tenuous blood supply. Excessive retraction, undermining, or tight closure can lead to wound breakdown. Full-thickness flaps and meticulous soft-tissue handling are mandatory.
Conclusion
The tendon suspension of the first metatarsal combined with interphalangeal joint arthrodesis remains a highly reliable and biomechanically sound procedure for correcting the dynamic claw hallux and flexible plantarflexed first ray. By meticulously executing the EHL transfer, achieving rigid IP joint fusion, and respecting the delicate dorsal soft tissues, the orthopedic surgeon can restore a plantigrade, functional foot and significantly improve the patient's gait mechanics and quality of life.
You Might Also Like