Elbow Arthrodesis: Indications, Techniques, and Clinical Outcomes
Key Takeaway
Elbow arthrodesis is a salvage procedure primarily reserved for patients with painful arthritis, persistent infection, or failed total elbow arthroplasty who require a stable, painless joint for high-demand activities. While it sacrifices motion, a meticulously positioned fusion—typically at 90 degrees of flexion for unilateral cases—provides a durable solution. This guide details the biomechanical considerations, optimal positioning, and step-by-step surgical techniques, including the Steindler, Brittain, Staples, Arafiles, and AO methods.
Introduction and Epidemiology
Elbow arthrodesis is a formidable and rarely performed procedure in modern orthopaedic surgery, universally regarded as a salvage operation. Historically, the procedure was most frequently indicated for the management of tuberculous septic elbow arthritis. During that era, primary fusion rates were notoriously poor, hovering around a 50% success rate. The advent of modern internal fixation techniques, specifically the application of rigid compression plating, has significantly improved these outcomes. Contemporary literature demonstrates primary fusion rates improving from the historical 50% to approximately 86%, with final fusion rates—when accounting for subsequent revision surgeries—ranging from 83% to 100%.

Despite these improvements in osseous union, elbow arthrodesis remains fraught with challenges. The procedure is associated with an exceptionally high reoperation rate. Reintervention is frequently required to address nonunion, deep infection, wound healing complications, and symptomatic hardware prominence, with patients undergoing an average of 1.4 to 1.6 reoperations.
Furthermore, the functional consequences of a fused elbow are profound. Unlike arthrodesis of the ankle, hip, or knee—which generally allow for a relatively normal, albeit altered, gait pattern—elbow arthrodesis results in severe functional disability. The loss of the elbow's dynamic arc of motion is highly disabling and can only be partially compensated by compensatory hypermobility in the trunk, shoulder, forearm, and wrist. Consequently, the decision to proceed with elbow arthrodesis must be approached with extreme caution, exhaustive preoperative planning, and thorough patient counseling regarding the permanent functional limitations and high likelihood of surgical complications.
Surgical Anatomy and Biomechanics
The elbow joint represents a highly complex, highly constrained hinge joint that facilitates both flexion-extension and forearm rotation. Arthrodesis of this joint is biomechanically challenging primarily due to the long lever arm of the upper extremity and the massive bending forces exerted across the fusion site during activities of daily living.

Biomechanically, the hand acts as a terminal load-bearing device at the end of the forearm lever. Any force applied to the hand is magnified at the elbow joint. When the elbow is fused, the normal dampening effect of the articulation is lost, and these forces are transmitted directly to the osteosynthesis construct and the healing bone interface. The triceps and brachialis/biceps musculature, which normally act as dynamic stabilizers, further contribute to the compressive and shear forces across the joint depending on the angle of fusion.
Anatomically, the posterior soft tissue envelope of the elbow is notoriously thin and poorly vascularized, lacking significant subcutaneous fat or muscle coverage over the olecranon. This anatomical reality predisposes the surgical site to wound breakdown, particularly when bulky internal fixation devices, such as dual reconstruction plates, are utilized. The ulnar nerve, coursing through the cubital tunnel posterior to the medial epicondyle, is at high risk of iatrogenic injury, traction neuritis, or compression from scar tissue and hardware, necessitating meticulous handling and frequent transposition during the arthrodesis procedure.
Indications and Contraindications
Elbow arthrodesis should strictly be considered a salvage procedure when no other satisfactory surgical reconstructive option, such as total elbow arthroplasty (TEA) or osteochondral allografting, exists.

Primary indications include severe septic arthritis, postseptic arthrosis, and chronic osteomyelitis where the eradication of infection necessitates the resection of the articular surfaces. Complex traumatic injuries, including high-velocity ballistic or war injuries resulting in massive, unreconstructable bone and soft tissue defects, frequently require arthrodesis. Additionally, young, high-demand patients (e.g., heavy manual laborers) with end-stage degenerative joint disease or post-traumatic osteoarthritis are candidates, as they would rapidly wear out or loosen a total elbow arthroplasty. Other indications include painful and severe elbow instability, failed internal fixation resulting in recalcitrant nonunions or pseudarthrosis, and, rarely, the salvage of a multiply failed total elbow arthroplasty where bone stock is insufficient for revision.
Contraindications are primarily related to the inability to achieve a stable osseous fusion or the presence of severe functional deficits in adjacent joints. Massive bone loss that prevents adequate bone contact, even with structural allografting, precludes successful arthrodesis. Similarly, massive soft tissue loss that is not amenable to local or free flap reconstruction represents an absolute contraindication due to the certainty of hardware exposure and deep infection. Finally, compromised function of the ipsilateral hand, wrist, shoulder, or spinal column is a strong relative contraindication; a patient with a fused elbow relies entirely on these adjacent joints to position the hand in space.
Operative vs Alternative Management Indications
| Clinical Scenario | Primary Management Strategy | Rationale and Considerations |
|---|---|---|
| Young Laborer with End-Stage DJD | Elbow Arthrodesis | TEA is contraindicated due to lifting restrictions; arthrodesis provides a stable, painless limb for heavy manual labor. |
| Elderly Patient with Low Demand and DJD | Total Elbow Arthroplasty (TEA) | Arthrodesis is overly restrictive; TEA provides excellent pain relief and functional ROM for activities of daily living. |
| Chronic Osteomyelitis / Septic Joint | Staged Arthrodesis | Infection must be eradicated prior to definitive fusion; TEA is highly contraindicated in the setting of active or recent deep infection. |
| Massive Bone and Soft Tissue Loss | Amputation / Resection Arthroplasty | If flap coverage is impossible or bone gaps exceed grafting capabilities, arthrodesis will fail. Flail arm or amputation may be required. |
| Failed TEA with Adequate Bone Stock | Revision TEA | If the functional demand is low and bone stock allows for allograft-prosthesis composite, revision is preferred over arthrodesis. |
| Failed TEA with Massive Bone Loss | Elbow Arthrodesis (Salvage) | Utilizing dual plating and massive structural allografts to bridge the defect and provide a stable, albeit immobile, extremity. |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is the cornerstone of a successful elbow arthrodesis. The physical examination must meticulously evaluate the skin and soft tissue envelope. Previous surgical incisions, traumatic scarring, and radiation fields must be documented. The surgeon must anticipate the need for local or free soft tissue coverage preoperatively; if the posterior soft tissue envelope is deemed inadequate to cover bulky hardware, a formal plastic surgery consultation for a latissimus dorsi or radial forearm flap is highly recommended prior to the index procedure.

The quality and quantity of available bone stock must be rigorously assessed. The surgeon should anticipate the requirement for substantial autogenous bone graft (typically from the anterior or posterior iliac crest) or structural allograft. Furthermore, the range of motion and functional status of the ipsilateral shoulder, forearm, wrist, and spinal column must be evaluated, as these joints will provide the compensatory motion required for activities of daily living. A comprehensive neurovascular examination is mandatory, documenting any preexisting neurologic deficits (particularly ulnar neuropathy) and confirming adequate arterial inflow to the hand.

Imaging protocols should include standard orthogonal anteroposterior and lateral radiographs of the elbow. Computed tomography (CT) with 3D reconstructions is essential for detailing bony anatomy, assessing bone loss, and planning osteotomies. If there is any clinical suspicion of indolent infection (especially in the setting of previous trauma or failed hardware), a comprehensive infectious workup is required. This includes a complete blood count (CBC), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP). Joint aspiration for cell count, Gram stain, and culture, or advanced imaging such as an Indium-111 labeled leukocyte scan, should be performed to rule out active osteomyelitis.
Selection of the Fusion Angle
The intended position of fusion is of paramount importance, as there is no single optimal position for elbow arthrodesis. No single fusion angle will allow the patient to perform all necessary activities of daily living. Historically, a standard fusion position of 90 degrees was advocated. However, contemporary recommendations suggest tailoring the angle between 45 and 110 degrees based entirely on the specific needs of the patient.
Factors influencing the choice of fusion angle include patient gender, occupation, hand dominance, specific functional requirements, associated joint involvement, and whether the arthrodesis is unilateral or bilateral.
To optimize patient satisfaction, a preoperative trial of immobilization is strongly recommended. The patient's elbow is immobilized in a rigid cast or adjustable brace at various angles for several weeks. This allows the patient to experience the functional limitations of a specific angle in their own environment and confirm their preferred position before irreversible surgery.
Suggested fusion angles based on clinical experience and literature:
* Male, dominant arm: Typically fused at 90 degrees to balance lifting capability with reaching.
* Female patients: Often prefer the cosmetic appearance of lower fusion angles (45 to 70 degrees), which allows the arm to hang more naturally at the side.
* High Flexion Angles (100 to 110 degrees): Allow for better hand-to-mouth function, feeding, and facial hygiene. However, cosmesis is often perceived as poor, and reaching away from the body is severely restricted.
* Low Flexion Angles (50 to 70 degrees): Better suited for extrapersonal needs, reaching, and carrying objects, but significantly impairs feeding and hygiene.
* Bilateral Elbow Arthrodesis: The dominant arm is typically fused at 110 degrees to allow for feeding and hygiene, while the non-dominant arm is fused at approximately 65 degrees to facilitate perineal care and extrapersonal reaching.
Detailed Surgical Approach and Technique
The surgical execution of an elbow arthrodesis requires meticulous exposure, aggressive joint preparation, and robust rigid internal fixation to counteract the immense deforming forces. The procedure is typically performed with the patient in the lateral decubitus position with the arm draped over a radiolucent post, or in the prone position, allowing unimpeded access to the posterior elbow and facilitating fluoroscopic imaging. A sterile tourniquet is applied high on the brachium.

Incision and Exposure
A straight posterior midline incision is utilized, typically incorporating or excising previous surgical scars. Full-thickness fasciocutaneous flaps are elevated to preserve the tenuous blood supply to the skin. The ulnar nerve must be identified proximally, traced through the cubital tunnel, and neurolysed distally into the flexor carpi ulnaris. Given the extensive posterior dissection and the placement of bulky hardware, an anterior subcutaneous or submuscular transposition of the ulnar nerve is routinely performed to prevent postoperative compression and traction neuritis.

The triceps mechanism is mobilized. Depending on the remaining bone stock and surgeon preference, a triceps-splitting, triceps-reflecting, or olecranon osteotomy approach can be utilized. Because the joint is being sacrificed, an extensile exposure that completely denudes the distal humerus and proximal ulna is required. The collateral ligaments and anterior capsule are excised to allow complete mobilization of the joint.
Articular Preparation and Bone Grafting
The remaining articular cartilage and subchondral bone of the distal humerus, proximal ulna, and radial head are aggressively resected using an oscillating saw and high-speed burr. The goal is to create broad, flat, and bleeding cancellous bone surfaces. Various geometric cuts can be employed, including flat planar cuts, chevron-shaped osteotomies, or step-cut configurations, to maximize surface area contact and inherent rotational stability. The radial head is typically excised or decorticated and fused to the proximal ulna to prevent painful radiocapitellar or proximal radioulnar impingement.

Once the bone ends are prepared and the desired fusion angle is achieved, the resulting voids must be filled. Copious amounts of autogenous cancellous bone graft, typically harvested from the iliac crest, are packed into the fusion site. If there is significant structural bone loss, a tricortical iliac crest strut graft or structural fibular allograft may be required to bridge the defect and maintain ulnohumeral length.
Fixation Strategies
Rigid internal fixation is the critical determinant of successful union. Modern techniques rely heavily on dual-plate osteosynthesis to neutralize both bending and torsional forces.

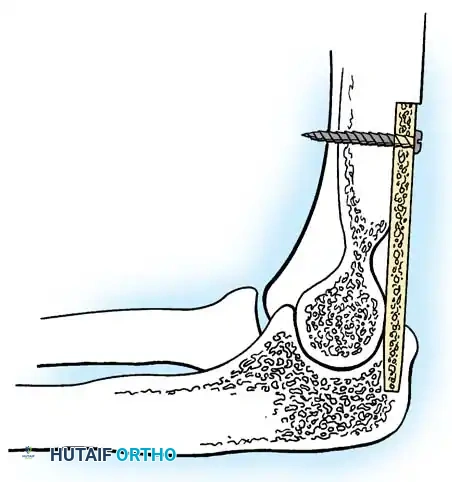
Provisional fixation is achieved with heavy Kirschner wires or Steinmann pins once the exact preoperative target angle is confirmed with a sterile goniometer and fluoroscopy.
Definitive fixation typically involves the application of a stout 3.5mm or 4.5mm dynamic compression plate (DCP) or locking compression plate (LCP) applied to the posterior aspect of the humerus and extending down the posterior or lateral aspect of the ulna. The plate must be carefully contoured to match the chosen fusion angle. A second plate is frequently applied in an orthogonal plane (e.g., medially or laterally) to create a highly rigid 90-90 construct.

Compression across the arthrodesis site is achieved using articulated tensioning devices or eccentrically placed screws before the locking screws are engaged. Interfragmentary lag screws can also be placed across the osteotomy site independent of the plates to enhance compression.
Following rigid fixation, the tourniquet is deflated, and meticulous hemostasis is obtained. The triceps mechanism is repaired over the hardware if possible, though muscle coverage is often deficient. Closed suction drains are placed, and the skin is closed in layers. If skin tension is excessive, immediate plastic surgery intervention for flap coverage is executed. Incisional negative pressure wound therapy (iNPWT) is frequently applied to mitigate postoperative edema and enhance wound healing.
Complications and Management
Elbow arthrodesis carries one of the highest complication profiles of any elective orthopaedic procedure. The surgeon and patient must anticipate a protracted clinical course. The average time to radiographic fusion is approximately 6 months, and reoperation to achieve this fusion is exceedingly common.

Nonunion is the most frequent major complication, driven by the massive biomechanical forces acting on the hardware before osseous integration occurs. Hardware failure, including plate fracture or screw pullout, is a direct consequence of delayed union or nonunion. Deep infection is also prevalent, secondary to the compromised local soft tissue envelope, prolonged operative times, and the frequent history of prior surgeries or sepsis in these salvage limbs.
Common Complications and Salvage Strategies
| Complication | Estimated Incidence | Pathophysiology | Management and Salvage Strategy |
|---|---|---|---|
| Nonunion / Pseudarthrosis | 10% - 20% | High bending moments; inadequate rigid fixation; poor biological environment. | Revision open reduction internal fixation (ORIF) with dual orthogonal locking plates; exchange of bone graft (use of rhBMP-2 or massive ICBG); consideration of external fixation. |
| Deep Surgical Site Infection | 5% - 15% | Thin posterior soft tissue envelope; poor vascularity; history of prior septic arthritis. | Aggressive serial surgical debridement; retention of hardware if stable until union occurs; targeted intravenous antibiotics; delayed hardware removal once fused. |
| Wound Breakdown / Hardware Exposure | 10% - 25% | Prominent posterior hardware directly under thin fasciocutaneous tissues; excessive skin tension. | Early plastic surgery consultation; local rotational flaps (e.g., anconeus, FCU) or regional/free flaps (e.g., latissimus dorsi, radial forearm flap). |
| Ulnar Neuropathy | 5% - 10% | Iatrogenic traction during exposure; compression from hematoma, scar tissue, or hardware. | Prevention via routine anterior transposition during index surgery. Postoperative management includes neurolysis and revision transposition if symptoms persist. |
| Hardware Failure (Plate Fracture) | 5% - 10% | Fatigue failure of the plate prior to osseous union due to cyclic loading. | Revision surgery with thicker, more robust plates; optimization of bone grafting to accelerate union; strict postoperative immobilization. |
Post Operative Rehabilitation Protocols
The postoperative rehabilitation following elbow arthrodesis is distinct from other elbow surgeries because the primary goal is strict immobilization of the elbow rather than early mobilization.

Immediately postoperatively, the arm is placed in a well-padded, rigid posterior splint or a bivalved cast. Depending on the rigidity of the internal fixation and the quality of the patient's bone stock, this immobilization is typically maintained for 6 to 8 weeks.
While the elbow is immobilized, aggressive physical therapy is initiated for the adjacent joints. Active and passive range of motion exercises for the shoulder, wrist, and hand are critical and must begin within the first postoperative week. Preventing adhesive capsulitis of the shoulder and stiffness in the digits is paramount, as the patient will rely entirely on these joints for upper extremity function once the elbow is permanently fused.
Serial radiographs are obtained at 2, 6, 12, and 24 weeks to monitor hardware integrity and the progression of osseous bridging. Clinical union is typically assessed by the absence of pain with loading, while radiographic union is defined by crossing trabeculae on orthogonal views. The average time to complete radiographic fusion is 6 months.
Return to heavy labor or high-impact activities is strictly prohibited until definitive radiographic union is confirmed. Even after successful fusion, patients are counseled that the limb will fatigue more quickly due to the altered biomechanics and the increased energy expenditure required by the shoulder and trunk to position the hand.
Summary of Key Literature and Guidelines
The literature surrounding elbow arthrodesis underscores its status as a definitive salvage procedure reserved for the most complex clinical scenarios.

Historical reviews highlight the evolution of the procedure from the era of tuberculous arthritis, where single-plate or simple screw fixation yielded dismal 50% union rates. Modern retrospective cohorts and biomechanical studies have definitively established that rigid, dual-plate osteosynthesis—specifically utilizing compression techniques and orthogonal plate placement—is the gold standard, driving primary union rates up to 86% and final union rates near 100%.
Despite these technical advancements, clinical guidelines consistently emphasize the severe functional penalty associated with the procedure. Biomechanical and kinematic studies have mapped the compensatory motions required for activities of daily living, proving that no single fusion angle provides comprehensive functionality. The literature strongly supports the necessity of individualized preoperative planning, utilizing trial immobilization to determine the optimal fusion angle tailored to the patient's specific vocational and personal needs.
Ultimately, elbow arthrodesis remains a highly demanding procedure for both the surgeon and the patient. Optimizing outcomes relies on meticulous soft tissue management, aggressive articular resection, robust multi-planar fixation, and comprehensive patient education regarding the inevitable functional limitations and the high probability of requiring subsequent surgical interventions.
Clinical & Radiographic Imaging
You Might Also Like

