Arthroscopic Management of Ankle Instability, Fractures, and Arthrodesis
Key Takeaway
Arthroscopic management of ankle pathology has evolved significantly, offering minimally invasive solutions for chronic instability, impingement syndromes, osteochondral lesions, and end-stage arthritis. This comprehensive guide details evidence-based surgical techniques, including arthroscopic-assisted lateral ligament repair, syndesmotic evaluation, and arthroscopic ankle arthrodesis. By minimizing soft tissue compromise and addressing concomitant intraarticular pathology, these advanced arthroscopic interventions optimize functional outcomes and accelerate postoperative rehabilitation in complex foot and ankle surgery.
INTRODUCTION TO ADVANCED ANKLE ARTHROSCOPY
The evolution of ankle arthroscopy has transformed the management of complex foot and ankle pathology. Originally utilized primarily as a diagnostic adjunct, arthroscopic techniques have advanced to become the definitive therapeutic modality for a wide spectrum of conditions, ranging from chronic lateral ankle instability and impingement syndromes to complex intraarticular fractures and end-stage tibiotalar arthritis.
For the practicing orthopedic surgeon, mastering these techniques requires a profound understanding of ankle biomechanics, precise portal anatomy to avoid neurovascular injury, and a rigorous adherence to evidence-based indications. This masterclass expands upon the foundational principles of operative orthopedics to provide a comprehensive, step-by-step guide to arthroscopic interventions in the ankle.
ANKLE INSTABILITY
Chronic ankle instability (CAI) typically manifests following recurrent inversion injuries, leading to attenuation or rupture of the lateral ligamentous complex—primarily the anterior talofibular ligament (ATFL) and the calcaneofibular ligament (CFL). Surgical intervention is indicated when prolonged conservative management, including aggressive peroneal strengthening and proprioceptive rehabilitation, fails to provide dynamic stability.
Thermal Capsular Shrinkage
Historically, thermal capsular shrinkage was proposed as a minimally invasive adjunct for managing micro-instability and capsular laxity. The theoretical biomechanical advantage relied on the application of radiofrequency energy to denature type I collagen, thereby reducing capsular volume.
Evidence-Based Pitfall: There is sparse evidence in the contemporary orthopedic literature supporting the efficacy of thermal capsular shrinkage for ankle instability. High rates of recurrent laxity, coupled with the risk of iatrogenic thermal injury to the superficial peroneal nerve (SPN) and sural nerve, have led to a Grade C recommendation (poor evidence). This procedure has largely been abandoned in modern practice in favor of anatomic repair.
Arthroscopic-Assisted Lateral Ligament Repair
Arthroscopic and arthroscopic-assisted lateral ligament repairs (often termed the "Arthroscopic Broström") have gained significant traction. These techniques aim to replicate the anatomic restoration of the ATFL while minimizing the morbidity associated with open exposures.
Surgical Technique:
1. Diagnostic Arthroscopy: Standard anteromedial (AM) and anterolateral (AL) portals are established. A thorough diagnostic sweep is mandatory.
2. Accessory Portal Placement: An accessory anterolateral portal is established under direct visualization, typically slightly inferior and anterior to the standard AL portal, ensuring the superficial peroneal nerve branches are protected.
3. Preparation of the Fibular Footprint: The lateral gutter is cleared of synovitis, and the fibular footprint of the ATFL is decorticated using a motorized shaver or burr to promote a bleeding healing response.
4. Anchor Placement: Suture anchors (typically 2.5 mm to 3.0 mm) are placed into the distal fibula arthroscopically.
5. Suture Passage: Using specialized suture-passing devices through the accessory portal, the sutures are passed through the attenuated ATFL and the extensor retinaculum (incorporating the Gould modification).
6. Knot Tying: The sutures are tied with the ankle held in neutral dorsiflexion and slight eversion to appropriately tension the construct.
Although these arthroscopic procedures primarily correct the laxity of the anterior tibiofibular ligament and ATFL, excellent clinical outcomes and high return-to-sport rates have been reported.
Clinical Pearl: Concomitant intraarticular pathological processes—such as osteochondral lesions, loose bodies, and anterolateral impingement lesions—are highly associated with chronic ankle instability. Therefore, diagnostic arthroscopy is universally recommended before any open lateral ankle ligament surgery. Failure to address these intraarticular pathologies is a primary cause of persistent postoperative pain, chronic regional pain syndrome (CRPS), and perceived failure of the stabilization procedure.
ANTERIOR AND POSTERIOR IMPINGEMENT
Ankle impingement syndromes are characterized by painful mechanical limitations of tibiotalar motion, driven by either osseous exostoses (osteophytes) or hypertrophic soft tissue (synovitis, Bassett's ligament).
Surgical Positioning and Setup Challenges
When complex pathology dictates that access to both the anterior and posterior aspects of the joint is necessary, intraoperative repositioning (switching the patient from supine to prone) can be highly cumbersome, increasing operative time and compromising the sterile field.
Alternative Setup Strategies:
* The Supine External Rotation Technique: Perform the anterior ankle arthroscopy with the patient supine as standard. Once complete, externally rotate the leg maximally (often requiring a sandbag under the ipsilateral hip) to place two posteromedial portals. While this avoids repositioning, access to the far lateral aspect of the posterior compartment can be restricted.
* The Prone Flexion Technique: The patient is positioned prone for standard posterior arthroscopy (utilizing posteromedial and posterolateral portals adjacent to the Achilles tendon). To access the anterior ankle, the knee is flexed to 90 degrees, allowing the surgeon to reach over the top of the foot to establish anterior portals.
Posterior Impingement and Os Trigonum Syndrome
Posterior impingement is frequently seen in plantarflexion-dominant athletes (e.g., ballet dancers, fast bowlers). It is often associated with an os trigonum or a prominent Stieda process. Arthroscopic excision yields excellent functional results with lower morbidity than open posteromedial or posterolateral approaches. However, a systematic review of the literature currently suggests a Grade C recommendation (poor quality evidence) for the arthroscopic treatment of posterior ankle impingement, primarily due to the lack of high-level randomized controlled trials, despite widespread clinical acceptance.
OSTEOCHONDRAL LESIONS OF THE TALUS (OLT)
Osteochondral lesions of the talus represent a challenging pathology, often presenting as deep, aching ankle pain following a traumatic event. The current literature supports a Grade B recommendation (fair evidence) for the arthroscopic treatment of OLTs.
Arthroscopic Management Principles:
* Access and Distraction: The highly congruent nature of the tibiotalar joint makes accessing posterior or central dome lesions difficult. Noninvasive distraction (using a standardized ankle strap) is often necessary to allow sufficient room for instruments, preventing iatrogenic scuffing of the tibial plafond.
* Debridement and Bone Marrow Stimulation: The primary surgical goal is the excision of unstable cartilage, removal of the necrotic subchondral bone cyst, and penetration of the subchondral plate (via microfracture or retrograde drilling) to stimulate fibrocartilage infill.
* Instrument Trajectory: It is critical that subchondral penetration is performed perpendicular to the lesion. If the lesion is located far posteriorly, transmalleolar drilling or the use of specialized curved guides may be required.
ANKLE FRACTURES AND SYNDESMOTIC INJURIES
The integration of arthroscopy into the acute management of ankle fractures represents a paradigm shift toward anatomic perfection and the mitigation of post-traumatic arthritis.
Intraarticular Fractures
Arthroscopy can be utilized to assist with the anatomic reduction of complex articular fractures. Currently, the literature consists primarily of case reports and case series, with no large-scale outcome studies to definitively prove the efficacy of this technique over standard fluoroscopic reduction.
* Talar Fractures: Arthroscopy aids in assessing the reduction of the talar dome.
* Distal Tibial Fractures: Arthroscopy has been successfully used to assist in the reduction of pilon fractures, posterior malleolar fractures, and pediatric transitional fractures (triplane and Tillaux fractures), ensuring the articular surface is perfectly flush.
Syndesmotic Instability
The distal tibiofibular syndesmosis is critical for the stability of the ankle mortise.
* Diagnostic Superiority: Arthroscopic examination of the syndesmosis is significantly more sensitive for detecting subtle, dynamic instability than standard stress radiographs or MRI. A 3-mm probe is introduced into the tibiofibular articulation; widening greater than 2 mm under direct visualization confirms instability.
* Chronic Syndesmosis Injuries: Patients presenting with chronic syndesmotic pain can be treated with arthroscopic debridement of the associated intraarticular pathological process (often hypertrophic scar tissue in the syndesmotic recess).
* Without Talar Shift: If there is no lateral displacement of the talus, debridement alone without screw fixation is often sufficient.
* With Chronic Widening: Patients with chronic widening of the syndesmosis benefit from aggressive arthroscopic debridement of the gutter followed by percutaneous placement of syndesmotic screws across the articulation after anatomic reduction is achieved.
Surgical Warning: Arthroscopic evaluation of the joint before the fixation of an ankle fracture can detect latent syndesmosis injuries and occult chondral shear lesions. However, there remains controversy in the literature regarding whether the immediate treatment of these otherwise unknown pathological processes definitively improves long-term outcomes. Consequently, there is currently a Grade I (incomplete) recommendation for routinely supplementing standard ankle fracture fixation with arthroscopy.
ARTHROSCOPIC ANKLE ARTHRODESIS
End-stage tibiotalar arthritis, whether post-traumatic, degenerative, or inflammatory, is definitively managed via ankle arthrodesis. Arthroscopic ankle arthrodesis has emerged as the gold standard for patients with minimal to moderate deformity, offering fusion rates comparable to or exceeding open techniques, with drastically reduced morbidity.
Indications and Biomechanical Advantages
The primary advantage of the arthroscopic approach is the preservation of the soft tissue envelope. This is particularly critical in patients with a poor soft tissue envelope, such as those with long-standing diabetes mellitus, severe vascular compromise, or extensive scarring from previous trauma. By avoiding large anterior or transfibular incisions, the periosteal blood supply is preserved, minimizing the risk of wound dehiscence and deep infection.
Surgical Technique: Step-by-Step
1. Setup and Portal Placement:
The patient is positioned supine with a thigh tourniquet. Standard anteromedial and anterolateral portals are established. A noninvasive distractor is applied to open the joint space.
2. Joint Preparation:
Aggressive synovectomy is performed to visualize the entire articular surface. The remaining articular cartilage is removed using ring curettes and elevators.
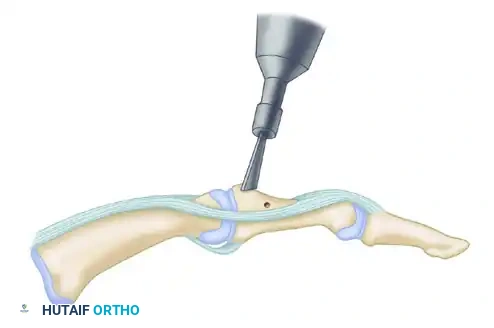
FIGURE 50-11 Ankle arthrodesis. Motorized burr used to remove thin layer of subchondral bone (approximately 2 mm).
As demonstrated in Figure 50-11, a motorized burr is systematically utilized to remove a thin layer of the subchondral bone plate (approximately 2 mm). The goal is to expose healthy, bleeding, punctate cancellous bone while strictly preserving the anatomic contour of the talar dome and the tibial plafond. Maintaining the ball-and-socket architecture provides intrinsic stability to the construct.
3. Positioning the Arthrodesis:
Once preparation is complete, the distractor is removed. The ankle is positioned in the optimal alignment for fusion:
* Neutral dorsiflexion (0 degrees)
* 0 to 5 degrees of valgus
* 5 to 10 degrees of external rotation (matching the contralateral limb)
* Slight posterior translation of the talus under the tibia.
4. Percutaneous Fixation:
Rigid compression is paramount for primary bone healing. Fixation is typically achieved using two or three large-diameter (6.5-mm or 7.3-mm) cannulated, partially threaded screws.

FIGURE 50-12 Fixation with two 6.5-mm cannulated screws (Anteroposterior View).
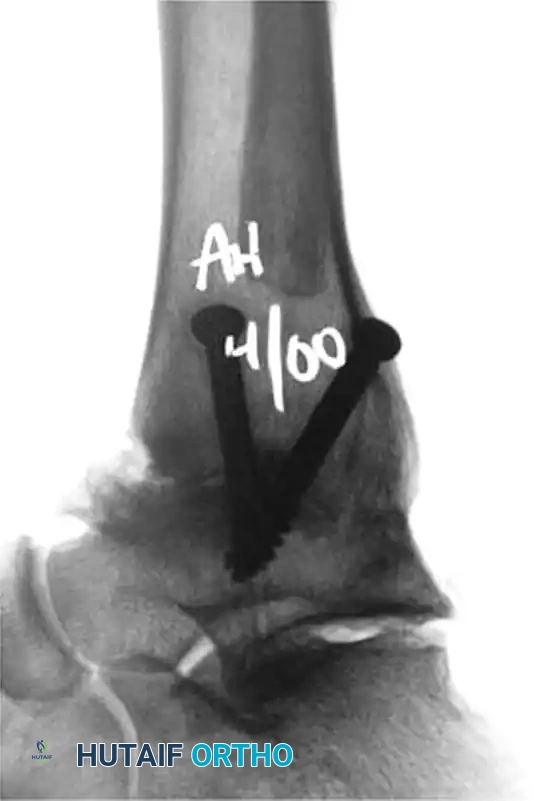
FIGURE 50-13 Fixation with two 6.5-mm cannulated screws (Lateral View).
As seen in the radiographic imaging (Figures 50-12 and 50-13), a standard crossed-screw configuration is employed.
* The First Screw (Home Run Screw): Typically directed from the posterior aspect of the distal tibia, aiming anteriorly and inferiorly into the neck of the talus.
* The Second Screw: Directed from the medial malleolus into the lateral aspect of the talar body.
* Optional Third Screw: If rotational stability is questionable, a third screw can be placed from the anterolateral tibia into the central talus.
Postoperative Protocol
Postoperatively, the patient is placed in a well-padded short leg splint and maintained strictly non-weight-bearing for 2 to 4 weeks. Following initial soft tissue healing, the patient is transitioned to a rigid cast or controlled ankle motion (CAM) boot. Progressive weight-bearing is initiated based on radiographic evidence of trabecular bridging, typically observed between 6 to 10 weeks postoperatively. The arthroscopic approach significantly accelerates the rehabilitation timeline compared to traditional open arthrodesis, primarily due to the absence of massive soft tissue dissection and the preservation of the extensor retinaculum.
You Might Also Like