Operative Management of Radial Head Dislocations & Galeazzi Fractures
Key Takeaway
Isolated radial head dislocations and Galeazzi fracture-dislocations are complex pediatric and adult injuries that are frequently misdiagnosed. Successful management relies on recognizing subtle radiographic markers, such as the ulnar bow sign, to identify occult instability. Treatment ranges from closed reduction with specific forearm positioning to open reduction via the Boyd approach, ensuring anatomic restoration of the radiocapitellar joint and distal radioulnar joint to prevent chronic instability and radioulnar synostosis.
INTRODUCTION TO FOREARM FRACTURE-DISLOCATIONS
The forearm functions as a complex, articulated ring composed of the radius, ulna, proximal radioulnar joint (PRUJ), distal radioulnar joint (DRUJ), and the interosseous membrane (IOM). Because of this ring-like biomechanical construct, an isolated fracture or dislocation is exceedingly rare; disruption in one area almost invariably necessitates a corresponding injury elsewhere in the ring.
Historically, "isolated" dislocations of the radial head and Galeazzi fracture-dislocations have been fraught with high rates of delayed diagnosis and mismanagement. In the pediatric population, the inherent plasticity of the immature skeleton further complicates the clinical picture, allowing for severe ligamentous disruption and joint dislocation with only subtle, plastic deformation of the adjacent bone. This masterclass provides an exhaustive, evidence-based review of the pathoanatomy, radiographic evaluation, and operative management of Galeazzi fracture-dislocations and radial head dislocations.
GALEAZZI FRACTURE-DISLOCATIONS IN THE PEDIATRIC SKELETON
A Galeazzi fracture-dislocation is defined as a fracture of the radial shaft with an associated disruption of the distal radioulnar joint (DRUJ). While relatively common in adults, these injuries are rare in children. Walsh et al. reported that less than 5% of all pediatric radial shaft fractures are associated with an obvious disruption of the DRUJ.
Pathoanatomy and Classification
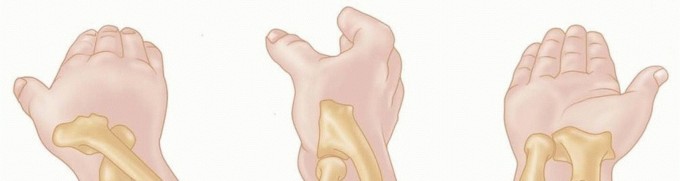
The deforming forces in a Galeazzi fracture are formidable. The brachioradialis exerts a proximal and deforming pull on the distal radial fragment, while the pronator quadratus pulls the distal fragment volarly and into pronation. The integrity of the DRUJ is compromised, involving tears of the triangular fibrocartilage complex (TFCC) and the volar/dorsal radioulnar ligaments.
Walsh et al. evaluated 41 pediatric Galeazzi fracture-dislocations and categorized them into two distinct biomechanical groups based on the level of the radial fracture and the direction of the ulnar head dislocation:
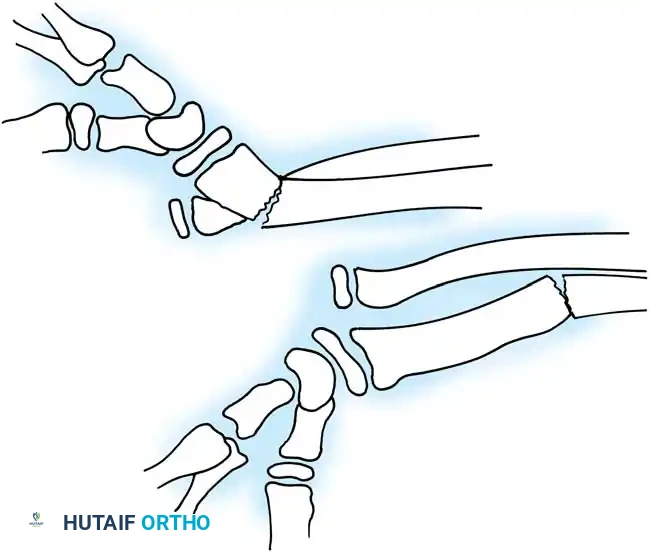
- Distal Third Fractures (Anterior Dislocation): Fractures occurring within the distal third of the radius are predominantly associated with an anterior dislocation of the ulnar head relative to the radius.
- Middle/Distal Junction Fractures (Posterior Dislocation): Fractures occurring more proximally, at the junction of the middle and distal thirds of the radial shaft, are classically associated with a posterior dislocation of the ulnar head.
Clinical Pearl: Similar to Monteggia lesions, Galeazzi fracture-dislocations are frequently unrecognized in the emergency department. Walsh et al. noted that in 41% of their pediatric patients, the DRUJ injury was missed during the initial evaluation. Always obtain true orthogonal radiographs of the wrist and elbow in any forearm fracture.
Management of Pediatric Galeazzi Injuries
Unlike adults, where Galeazzi fractures are universally considered "fractures of necessity" requiring open reduction and internal fixation (ORIF), most of these injuries in children can be managed successfully with closed reduction.
Closed Reduction Technique:
1. Traction: Apply sustained longitudinal traction to overcome the deforming forces of the brachioradialis.
2. Correction of Angulation: The radius must be restored to its anatomic length, and all angular and rotational deformities must be corrected.
3. DRUJ Reduction: Once the radius is anatomically aligned, the DRUJ typically reduces spontaneously and becomes stable.
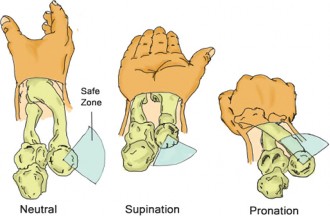
4. Immobilization: The forearm is immobilized in a long-arm cast. The position of the forearm (supination vs. pronation) depends on the direction of the DRUJ instability. Generally, supination stabilizes a dorsally unstable DRUJ, while pronation stabilizes a volarly unstable DRUJ.
Mikic reported uniformly good results following the conservative treatment of 14 Galeazzi fractures in children, a finding corroborated by Walsh et al., who reported excellent or good outcomes when anatomic reduction of the radius was achieved and maintained.
Variants and Blocks to Reduction
Occasionally, closed reduction of a pediatric Galeazzi fracture-dislocation is impossible due to soft tissue interposition. A well-documented variant involves the interposition of the periosteum or the extensor carpi ulnaris (ECU) tendon into the DRUJ, physically blocking the ulnar head from reducing into the sigmoid notch of the radius.
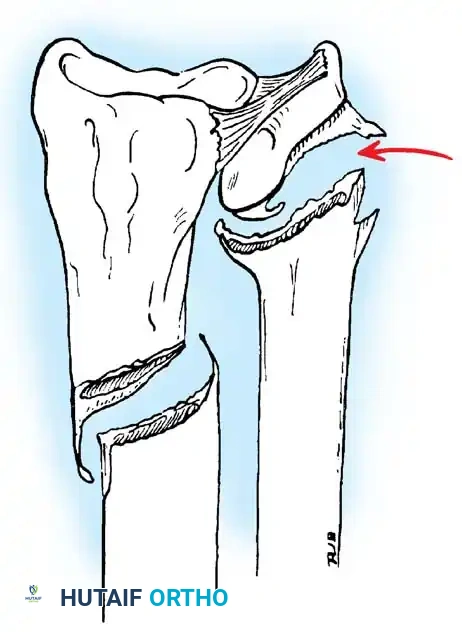
Surgical Warning: If the DRUJ remains widened or incongruent on post-reduction radiographs despite anatomic alignment of the radius, soft tissue interposition must be suspected. Repeated forceful closed reduction attempts are contraindicated as they may cause iatrogenic physeal injury or further chondral damage. Open exploration of the DRUJ via a dorsal approach is mandatory to extract the interposed periosteum or tendon.
"ISOLATED" DISLOCATIONS OF THE RADIAL HEAD
True isolated traumatic dislocations of the radial head without an associated fracture of the ulna are exceedingly rare. When they do occur, they are almost exclusively seen in children due to the unique plasticity of the pediatric bone. An acute "isolated" anterior, lateral, or posterior dislocation can theoretically occur, but the clinical diagnosis is notoriously difficult.
A delay in diagnosis ranging from 1 week to 18 months has been widely reported. This delay significantly increases the likelihood that the child will require complex open surgical intervention and is associated with markedly inferior long-term functional outcomes.
The Myth of the Isolated Dislocation: The Ulnar Bow Sign
Lincoln and Mubarak fundamentally challenged the existence of the "isolated" traumatic radial head dislocation. In a landmark study of traumatic radial head dislocations, they demonstrated that what appears to be an isolated injury is, in reality, a minimal Monteggia fracture-dislocation accompanied by plastic deformation of the ulna.
To quantify this, they developed the "Ulnar Bow Sign."
How to Measure the Ulnar Bow Sign:
1. Obtain a true lateral radiograph of the forearm.
2. Draw a straight line along the dorsal border of the ulna, extending from the level of the olecranon proximally to the distal ulnar metaphysis.
3. Measure the maximum distance (bowing) between this straight line and the dorsal cortex of the ulna.
Key Findings by Lincoln and Mubarak:
* In a normal control group, maximal ulnar bowing is less than 1 mm.
* In patients with "isolated" radial head dislocations, the ulna consistently demonstrated plastic deformation.
* The location of maximal ulnar bowing uniformly occurred near the mid-ulna (mean distance of 45 mm ± 2% from the proximal end).
* The average magnitude of the bow was 3.9 ± 0.4 mm.
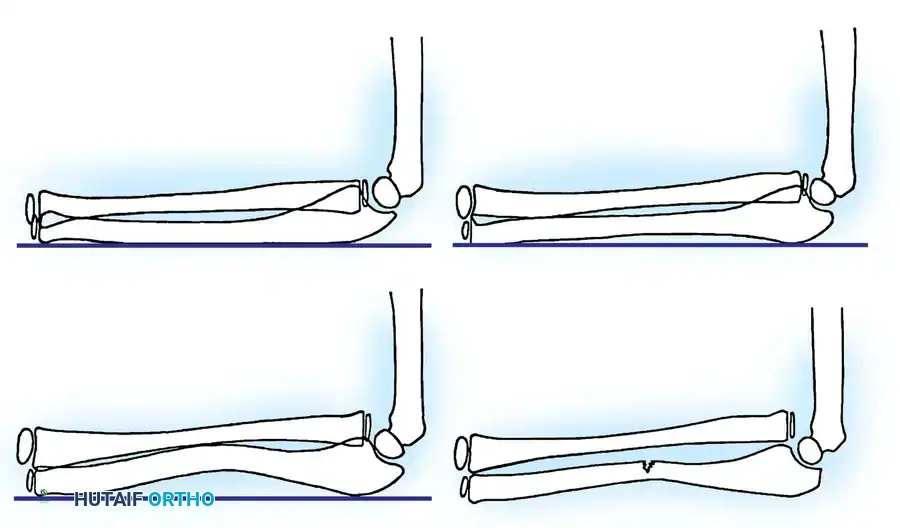
Clinical Pearl: Lincoln and Mubarak asserted that ulnar bowing of more than 1 mm is pathologic. It signifies a serious injury to the forearm ring and must alert the physician to an undetected radial head dislocation. The term "isolated radial head dislocation" is a misnomer; these injuries should be accurately classified and treated as minimal Monteggia fracture-dislocations.
OPERATIVE MANAGEMENT OF RADIAL HEAD DISLOCATIONS
The direction of the radial head dislocation dictates the reduction maneuver. Vesely reported on 17 cases of radial head dislocations (13 anterior, 3 lateral, and 1 posterior), noting that only four required open reduction.
Closed Reduction Techniques
Immediate closed reduction under conscious sedation or general anesthesia is the first line of treatment for acute injuries.
- Anterior Dislocation: The forearm is subjected to longitudinal traction and placed in supination with the elbow flexed to 90 degrees. Supination rotates the radial tuberosity anteriorly, clearing it from the ulna, while flexion relaxes the biceps tendon, which otherwise acts as a deforming force pulling the radius anteriorly.
- Posterior Dislocation: The forearm is subjected to traction and held in pronation with the elbow flexed to 90 degrees.
- Lateral Dislocation: Direct manual pressure is applied over the radial head from lateral to medial while the forearm is manipulated through a range of pronation and supination to find the most stable position.
Following reduction, the elbow is immobilized in a long-arm cast for 3 to 4 weeks.
Indications for Open Reduction
Open reduction of the radial head is strictly indicated under the following circumstances:
1. The dislocation has persisted for more than 3 weeks (chronic/neglected dislocation).
2. Closed manipulation has failed to achieve or maintain a concentric reduction.
3. There is radiographic evidence of soft tissue interposition (e.g., annular ligament or capsule blocking the joint).
Surgical Technique: The Boyd Approach
When open reduction is required, the Boyd approach provides excellent, extensile exposure to the proximal radius and the radiocapitellar joint.
Step 1: Positioning and Incision
The patient is positioned supine with the arm draped over the chest. A longitudinal incision is made beginning 2 cm proximal to the lateral epicondyle, extending distally over the lateral epicondyle, and continuing along the subcutaneous border of the ulna.
Step 2: Internervous Plane
The deep fascia is incised. The internervous plane lies between the anconeus (supplied by the radial nerve) and the extensor carpi ulnaris (supplied by the posterior interosseous nerve [PIN]).
Step 3: Deep Dissection and PIN Protection
The supinator muscle is identified.
Surgical Warning: The PIN runs through the substance of the supinator. To protect the PIN, the forearm must be fully pronated. Pronation moves the PIN anteriorly and medially, safely away from the surgical field.
The supinator is subperiosteally elevated off the proximal ulna and reflected laterally, exposing the radial head and neck.
Step 4: Joint Clearance and Reduction
The radiocapitellar joint is inspected. Any interposed tissue (often the torn, inverted annular ligament or joint capsule) is meticulously excised or retracted. The radial head is directly reduced onto the capitellum.
Step 5: Ligamentous Repair and Fixation
The annular ligament should be repaired if sufficient tissue remains. If the reduction is unstable, temporary transarticular fixation is required. A smooth Kirschner wire (K-wire) can be placed obliquely across the radioulnar joint or directly transcapitellar (from the posterior capitellum into the radial head).
Step 6: Closure and Postoperative Protocol
The supinator is loosely reapproximated to cover the exposed bone, minimizing the risk of radioulnar synostosis. The arm is immobilized in a long-arm cast at 90 degrees of flexion.
* The K-wire is removed at 3 weeks.
* The cast is maintained for an additional 3 weeks (total 6 weeks of immobilization) before initiating a structured range-of-motion rehabilitation program.
Complications of Open Reduction
As noted by Vesely, open reduction of the proximal radioulnar joint is not benign. The two most devastating complications are:
1. Redislocation: Often due to failure to recognize and correct underlying ulnar plastic deformation (the minimal Monteggia variant). If the ulna is bowed, the radius will inevitably subluxate.
2. Proximal Radioulnar Synostosis: Cross-union between the radius and ulna obliterates forearm rotation. This is mitigated by meticulous hemostasis, avoiding aggressive subperiosteal stripping of the interosseous membrane, and ensuring the supinator muscle belly is interposed between the radius and ulna during closure.
MANAGEMENT OF CHRONIC POSTTRAUMATIC DISLOCATIONS
Neglected radial head dislocations present a formidable reconstructive challenge. Over time, the radial head becomes hypertrophic and deformed, the capitellum flattens, and the soft tissues contract. Simple open reduction is universally doomed to fail due to the contracted interosseous membrane and the shortened, deformed ulna.
The Hirayama Ulnar Osteotomy
For chronic dislocations, addressing the ulnar deformity is the cornerstone of treatment. Hirayama et al. pioneered a technique that relies on the biomechanical tethering effect of the interosseous membrane (IOM).
Surgical Rationale:
Instead of directly attacking the contracted radiocapitellar joint, an osteotomy of the proximal third of the ulna is performed. The ulna is intentionally overcorrected (angulated dorsally and laterally) and elongated.
Because the central band of the interosseous membrane connects the radius to the ulna, elongating and angulating the ulna places the IOM under extreme tension. This tension acts as a distal and medial pull on the radius, effectively dragging the dislocated radial head distally and reducing it anatomically against the capitellum without requiring direct exposure of the radial head itself.
Outcomes:
Hirayama et al. reported excellent results in nine chronic posttraumatic dislocations using this ulnar osteotomy technique. They concluded that the interosseous membrane of the forearm is the single most important anatomic structure in maintaining the corrected position of the radial head in chronic settings. Rigid plate fixation of the ulnar osteotomy, often supplemented with structural iliac crest bone grafting to maintain the elongation, is mandatory to prevent collapse and recurrent dislocation.
You Might Also Like