RASL Procedure: Mastering Scapholunate Instability Correction

Key Takeaway
Welcome to the OR, fellows. Today, we're tackling scapholunate instability with the Reduction and Association of the Scaphoid and Lunate (RASL) procedure. This masterclass covers comprehensive anatomy, meticulous preoperative planning, and a granular, real-time walkthrough of every surgical step. We'll emphasize precise instrument use, critical decision-making, and essential pearls to achieve optimal wrist stability and function.
Comprehensive Introduction and Patho-Epidemiology
Scapholunate instability represents the most frequently encountered carpal instability in clinical orthopedic practice, yet it remains one of the most challenging pathologies to manage effectively. The intrinsic complexity of carpal kinematics, combined with the often-delayed presentation of these injuries, creates a formidable reconstructive dilemma for the hand and upper extremity surgeon. When the primary constraint—the scapholunate interosseous ligament (SLIL)—is irreparably ruptured, the synchronous motion of the proximal carpal row is uncoupled, initiating a predictable and devastating cascade of degenerative changes known as Scapholunate Advanced Collapse (SLAC).
The Reduction and Association of the Scaphoid and Lunate (RASL) procedure was developed as a robust mechanical solution to this biomechanical failure. Originally conceptualized to address the shortcomings of soft-tissue reconstructions, which are notoriously prone to stretching and attenuation over time, the RASL procedure utilizes rigid internal fixation, typically via a headless compression screw, to re-establish the critical anatomical relationship between the scaphoid and lunate. By mechanically linking these two bones, the procedure aims to restore near-normal carpal kinematics, halt the progression of dorsal intercalated segment instability (DISI), and prevent the point-loading that drives the SLAC arthritis sequence.
Epidemiologically, SLIL injuries predominantly affect young, active individuals, typically occurring following a fall onto an outstretched hand (FOOSH). The mechanism of injury usually involves a combination of axial loading, wrist hyperextension, and ulnar deviation, which subjects the SLIL to supraphysiologic tensile and shear forces. Unfortunately, because the initial radiographs may appear normal in the dynamic or pre-dynamic stages of instability, these injuries are frequently misdiagnosed as simple wrist sprains. By the time the patient presents to a specialist with chronic pain, weakness, and a mechanical "clunk," the ligament is often retracted, scarred, and no longer amenable to primary repair, necessitating more complex interventions such as the RASL procedure.
While modern iterations of scapholunate management include various capsulodesis and tenodesis techniques (such as the modified Brunelli procedure), the RASL procedure remains a cornerstone technique, particularly when a stable fibrous union or formal limited arthrodesis is desired. The philosophy underlying RASL is that a rigid, metallic association allows for the formation of a dense, stabilizing fibrous non-union (or true bony fusion, depending on joint preparation), which can withstand the massive cyclic loads of daily wrist function far better than reconstructed soft tissues alone.
Detailed Surgical Anatomy and Biomechanics
A profound understanding of carpal anatomy and the intricate biomechanics of the proximal row is an absolute prerequisite for executing the RASL procedure successfully. The proximal carpal row—comprising the scaphoid, lunate, and triquetrum—functions as an intercalated segment. It has no direct tendon insertions; rather, its motion is entirely dictated by the mechanical forces exerted by the surrounding articular contours and the complex network of intrinsic and extrinsic carpal ligaments. The normal relationship between the scaphoid and the lunate is paramount for synchronized wrist motion, with the scapholunate angle typically measuring exactly 46 degrees in a neutral, uninjured wrist.

The Scapholunate Interosseous Ligament Complex
The SLIL is the primary stabilizer of the scapholunate articulation. It is not a monolithic structure but rather a complex, C-shaped ligamentous apparatus composed of three distinct histological and biomechanical regions. The dorsal component is the thickest (approximately 3 mm thick), composed of stout, transversely oriented Type I collagen fibers. It is the most biomechanically significant portion, acting as the primary restraint against translation and independent scaphoid flexion. The palmar component is thinner (approximately 1 mm) and provides secondary stability, primarily resisting rotational forces. Finally, the proximal component is a thin, membranous fibrocartilaginous structure that offers negligible mechanical strength but serves to separate the radiocarpal joint from the midcarpal joint.
Secondary Carpal Stabilizers
While the SLIL is the primary restraint, isolated sectioning of the SLIL in cadaveric models does not immediately produce a static DISI deformity. The manifestation of a static deformity requires the concomitant attenuation or failure of the secondary carpal stabilizers. These include the extrinsic palmar ligaments, such as the radioscaphocapitate (RSC) and the long radiolunate (LRL) ligaments, as well as the dorsal intercarpal (DIC) and dorsal radiocarpal (DRC) ligaments. The DIC, in particular, plays a crucial role in tethering the scaphoid to the triquetrum and stabilizing the proximal row. During the surgical approach for the RASL procedure, meticulous preservation of these secondary stabilizers is mandatory to ensure the long-term success of the reconstruction.
Pathokinematics of DISI Deformity
Normally, the scaphoid and lunate are intimately linked. With wrist flexion and radial deviation, the scaphoid naturally wants to flex, and via the intact SLIL, it pulls the lunate into flexion. Conversely, with wrist extension and ulnar deviation, the triquetrum extends, pulling the lunate and the scaphoid into extension. This synchronous motion is completely uncoupled following a complete SLIL rupture.

Post-injury, the scaphoid, driven by the forces crossing the radioscaphoid joint and the pull of the trapezium/trapezoid, assumes an excessively flexed posture. Simultaneously, the lunate, now freed from the scaphoid but still attached to the triquetrum via the intact lunotriquetral ligament, falls into abnormal extension. This divergent rotation creates the classic Dorsal Intercalated Segment Instability (DISI) pattern. This unlinked lunate extension creates a widened scapholunate diastasis, alters carpal kinematics, and forces the capitate to migrate proximally and translate dorsally. This pathological alignment creates massive point stress at the radiostylo-scaphoid juncture, initiating the SLAC arthritis cascade.
Exhaustive Indications and Contraindications
The decision to perform a RASL procedure requires meticulous patient selection, relying heavily on a combination of patient history, physical examination, advanced imaging, and an understanding of the patient's functional demands. The procedure is not a panacea for all wrist pain; it is a highly specific intervention designed for a specific stage of carpal instability. The ideal candidate is a patient with a chronic, static scapholunate dissociation where the SLIL is completely irreparable, yet the carpal deformity remains manually or fluoroscopically reducible, and critically, the articular cartilage of the midcarpal joint remains pristine.
We typically categorize scapholunate instability into a spectrum: pre-dynamic, dynamic, and static. The RASL procedure is primarily indicated for static instability, where abnormal alignment is evident on routine resting radiographs (e.g., widened scapholunate interval >3mm, scaphoid cortical ring sign, scapholunate angle >60 degrees). It can also be considered in severe dynamic instability cases where arthroscopic evaluation confirms a complete, non-repairable tear (Geissler Grade IV) and the patient has failed conservative management.

Absolute and Relative Contraindications
The most critical contraindication to the RASL procedure is the presence of advanced degenerative joint disease, specifically SLAC Stage II (involving the entire scaphoid fossa) or SLAC Stage III (involving the capitolunate joint). If significant midcarpal arthritis is present, attempting to reduce and associate the scaphoid and lunate will only exacerbate the patient's pain by increasing pressure across already damaged cartilaginous surfaces. In such scenarios, salvage procedures like a proximal row carpectomy (PRC) or a four-corner arthrodesis are the gold standard.
Furthermore, a fixed, irreducible carpal deformity is an absolute contraindication. If the scaphoid and lunate cannot be anatomically reduced due to severe, chronic soft-tissue contractures, the RASL screw cannot be placed in the correct biomechanical axis, leading to inevitable hardware failure and persistent pain. Poor bone stock, active infection, and non-compliance with post-operative rehabilitation are also significant contraindications. Notably, focal arthritis limited to the tip of the radial styloid (SLAC Stage I) is not a contraindication, as a radial styloidectomy is a routine and necessary component of the RASL procedure.
Summary Table of Indications and Contraindications
| Category | Specific Criteria | Rationale |
|---|---|---|
| Indications | Chronic SLIL tear (>6 weeks) | Primary repair is no longer biologically feasible due to tissue retraction. |
| Static SL dissociation | Radiographic evidence of diastasis and DISI requires rigid structural correction. | |
| Reducible carpal deformity | Anatomical alignment must be achievable to allow proper screw trajectory. | |
| Intact midcarpal cartilage | Preservation of the capitolunate joint is essential for post-operative motion and pain relief. | |
| Contraindications | SLAC Stage II or III arthritis | Degenerated cartilage will not tolerate the altered forces; requires salvage procedure. |
| Fixed, irreducible DISI | Inability to reduce the joint precludes the mechanical goals of the RASL procedure. | |
| Inadequate scaphoid/lunate bone stock | Prevents secure purchase of the headless compression screw. | |
| Inflammatory arthropathies | Systemic disease compromises ligamentous integrity and bone quality globally. |
Pre-Operative Planning, Templating, and Patient Positioning
Thorough pre-operative planning is the foundation of a successful RASL procedure. The surgeon must meticulously evaluate a complete series of plain radiographs, including neutral posteroanterior (PA), true lateral, scaphoid view, and clenched-fist PA views in pronation to accentuate dynamic diastasis. Crucially, contralateral wrist films must always be obtained for comparison, as some individuals exhibit constitutional ligamentous laxity with a naturally widened SL interval.
Advanced imaging, particularly high-resolution MRI or MR arthrography, is highly recommended to assess the vascularity of the proximal pole of the scaphoid, evaluate the integrity of the secondary carpal ligaments, and rule out subtle chondral defects in the midcarpal joint that might not be visible on plain radiographs. Diagnostic wrist arthroscopy often serves as the final, definitive pre-operative step, allowing direct visualization of the SLIL remnants, probing of the cartilage surfaces, and dynamic assessment of the instability.
Radiographic Templating
Pre-operative templating is essential to estimate the appropriate trajectory and length of the headless compression screw. Using digital templating software on true PA and lateral radiographs, the surgeon should measure the combined width of the scaphoid and lunate along the intended axis of fixation. The goal is to select a screw length that provides maximum thread purchase in both bones while ensuring the screw is completely buried beneath the subchondral bone at both the entry (scaphoid) and exit (lunate) points. Typically, a screw length between 22 mm and 26 mm is required. We must also plan the amount of radial styloid to be resected to prevent impingement.
Patient Positioning and Fluoroscopy Setup
The patient is positioned supine on the operating table with the affected arm extended onto a standard, radiolucent hand table. A pneumatic tourniquet is applied to the proximal arm, over copious cast padding, to ensure a pristine, bloodless surgical field. The tourniquet is typically inflated to 250-300 mmHg after exsanguination with an Esmarch bandage.
The positioning of the fluoroscopy unit (C-arm) is a critical logistical step that must be coordinated before the incision is made. The C-arm should be positioned parallel to the longitudinal axis of the hand table, allowing it to easily swing 90 degrees to obtain true AP and lateral views without requiring the surgeon to awkwardly reposition the patient's arm. The hand table itself may need to be rotated 90 degrees from the main operating table to facilitate this seamless fluoroscopic arc. Standard sterile prep from the fingertips to above the elbow is performed, a sterile stockinette covers the forearm, and the hand is draped free to allow full, unimpeded range of motion during the procedure.
Step-by-Step Surgical Approach and Fixation Technique
The execution of the RASL procedure demands meticulous soft-tissue handling, precise spatial awareness, and exact fluoroscopic corroboration. The procedure blends delicate ligament-sparing exposure with robust osseous fixation.
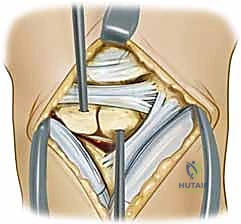
Step 1: Dorsal Ligament-Sparing Capsulotomy
We begin with a longitudinal dorsal incision, approximately 4-5 cm in length, centered just ulnar to the tubercle of Lister. This specific placement minimizes the risk of injuring the terminal branches of the superficial radial nerve (SRN) and the dorsal sensory branch of the ulnar nerve, while providing direct access to the interval between the third and fourth extensor compartments.

Subcutaneous dissection is carried out with tenotomy scissors, carefully identifying and retracting the prominent dorsal venous network to minimize post-operative edema. The extensor retinaculum is identified, and an oblique incision is made through it, running parallel to the course of the Extensor Pollicis Longus (EPL) tendon.

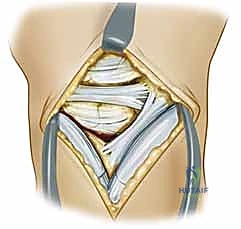
The EPL is transposed radially, and the tendons of the fourth compartment (extensor digitorum communis and extensor indicis proprius) are retracted ulnarly. This exposes the underlying dorsal wrist capsule. To preserve the critical secondary stabilizers, we utilize a ligament-sparing capsulotomy (often referred to as the Berger approach). An oblique incision is made through the dorsal capsule, running parallel and just proximal to the dorsal intercarpal (DIC) ligament.

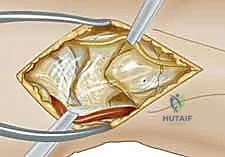
This capsular flap is elevated radially and distally, providing wide, panoramic exposure of the scapholunate interval, the proximal scaphoid pole, and the dorsal lunate.

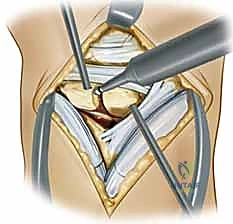
Step 2: Joint Preparation and Debridement
Upon exposing the joint, the remnants of the torn SLIL are visualized.
Clinical & Radiographic Imaging Archive