Beyond Hemipelvectomy: Preservation of the Sciatic in Buttock Surgery
Key Takeaway
Here are the crucial details you must know about Beyond Hemipelvectomy: Preservation of the Sciatic in Buttock Surgery. Limb-sparing surgery is the primary treatment for most soft tissue sarcomas of the gluteus maximus, reducing the need for hemipelvectomy. This approach allows for effective tumor resection with minimal functional deficits, often facilitating the preservation of the sciatic nerve due to the gluteus maximus's anatomical detachment from underlying retrogluteal structures. This minimizes gait issues and avoids amputation in most cases.
Introduction and Epidemiology
The gluteus maximus and the enveloping buttock musculature constitute a frequent anatomic locus for the pathogenesis of both high-grade and low-grade soft tissue sarcomas. In the realm of orthopedic oncology, the gluteal compartment is classically designated as a "quiet area" or silent zone for soft tissue malignancies. Due to the vast potential volume of the gluteal fascial compartment and the deep, compliant nature of the musculature, neoplastic lesions in this region rarely manifest with compressive or localized symptoms until they achieve massive dimensions. Consequently, patients typically present with a painless, progressively enlarging mass; by the time of clinical detection, the tumor burden is often substantial, presenting significant reconstructive and oncologic challenges.
Historically, the oncologic standard of care for both low-grade and high-grade soft tissue sarcomas of the buttock was a posterior cutaneous flap hemipelvectomy (hindquarter amputation). This radical ablative procedure was considered an absolute necessity to achieve wide, negative surgical margins and mitigate the unacceptably high rates of local recurrence. However, the paradigm of orthopedic oncology has shifted dramatically over the past several decades. The advent of advanced cross-sectional imaging, coupled with the integration of neoadjuvant and adjuvant radiotherapy and targeted systemic chemotherapy, has facilitated a definitive transition toward limb-sparing surgical procedures.

In contemporary practice, function-preserving resections can reliably achieve safe, negative oncologic margins (R0 resection) in the vast majority of buttock sarcomas, rendering hemipelvectomy an operation of historical significance for all but the most locally advanced, invasive lesions. Tumors arising within the gluteus maximus are frequently confined to the primary muscle belly. They do not inherently violate the deep fascial boundaries extending into the underlying retrogluteal space, nor do they typically demonstrate direct osseous invasion of the sacrum, ilium, or proximal femur. The paramount anatomic structure within the retrogluteal space that dictates the feasibility of limb salvage is the sciatic nerve. With rigorous preoperative staging and meticulous surgical execution, the sciatic nerve can usually be preserved, yielding a functional, sensate lower extremity with surprisingly minimal reconstructive requirements.
Surgical Anatomy and Biomechanics
A profound, three-dimensional understanding of the cross-sectional and topographic anatomy of the gluteal region is indispensable for executing a safe oncologic resection. The surgeon must navigate complex fascial planes to achieve wide margins while preserving the sciatic nerve and maximizing postoperative biomechanical function.
Gluteus Maximus Origin and Insertion
The gluteus maximus is the largest, most superficial, and most coarsely fasciculated muscle of the gluteal region. Its broad origin encompasses the posterior aspect of the sacral lamina, the posterior gluteal line of the iliac crest, the aponeurosis of the erector spinae, the sacrotuberous ligament, and the ischium. The muscle fibers course obliquely and laterally toward their insertion points. The majority of the superior and deep fibers converge to insert into the proximal portion of the iliotibial tract of the fascia lata. The deeper, inferior fibers insert directly onto the gluteal tuberosity of the proximal femur. This robust femoral insertion begins just superior to the greater trochanter, extends approximately four to five centimeters inferiorly, and attaches securely to the linea aspera of the femoral shaft.

Retrogluteal Space and Sciatic Nerve
The anatomic interval situated deep to the gluteus maximus is clinically designated as the retrogluteal space. This critical potential space houses the posterior hip musculature, including the piriformis, superior gemellus, obturator internus, inferior gemellus, quadratus femoris, and the deeper portions of the gluteus medius and minimus muscles.

Crucially, the gluteus maximus possesses no direct muscular or tendinous attachments to these retrogluteal structures as it transverses them. The superficial and deep compartments are separated by a distinct layer of loose areolar tissue and multiple bursae (most notably the trochanteric and ischial bursae). This anatomic reality is the foundational cornerstone of limb salvage in this region. It permits the surgical development of a clear, avascular dissection plane, facilitating the en bloc elevation of the gluteus maximus away from the deep structures and allowing for the preservation of the sciatic nerve in most clinical scenarios.
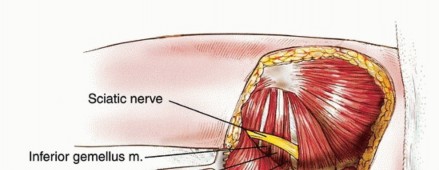
The sciatic nerve represents the most critical structure within the retrogluteal space. It exits the true pelvis via the greater sciatic foramen, typically passing inferior to the piriformis muscle (though anatomic variants, such as the nerve piercing the piriformis, must be anticipated). As it courses distally, it rests upon the short external rotators and the quadratus femoris. Topographically, the nerve can be reliably identified midway between the ischial tuberosity and the greater trochanter. Because the sciatic nerve lies in close proximity to the deep investing fascia of the gluteus maximus, large sarcomas of this muscle frequently abut or displace the nerve. However, true epineural invasion by the sarcoma is exceedingly rare; the nerve is most often displaced around the dense, reactive tumor pseudocapsule, allowing for careful neurolysis and structural preservation.
Vascular Supply and Innervation
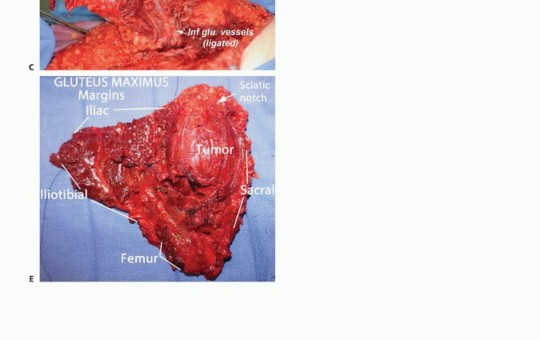
The vascular supply to the gluteus maximus is exceptionally robust, derived primarily from the superior and inferior gluteal arteries, both of which are terminal branches of the internal iliac artery. The inferior gluteal vessels exit the pelvis inferior to the piriformis muscle, in close association with the sciatic nerve, to enter the deep midportion of the gluteus maximus. During an en bloc resection, these inferior gluteal vessels are routinely identified, ligated, and transected to allow mobilization of the muscle belly. Innervation is provided exclusively by the inferior gluteal nerve (L5, S1, S2), which parallels the course of the inferior gluteal artery.
Biomechanics of Hip Extension
Despite the massive cross-sectional area of the gluteus maximus, its complete surgical extirpation results in a surprisingly minimal functional deficit in routine ambulation. The primary biomechanical role of the gluteus maximus is forceful hip extension and external rotation, particularly from a flexed position (e.g., stair climbing, rising from a deep seated position, or running). During normal, level-ground ambulation, the hamstrings and the ischial head of the adductor magnus act as the primary effectors of hip extension during the stance phase. Consequently, following a total gluteus maximus resection, patients typically maintain a normal, non-antalgic gait pattern on level surfaces. However, they will demonstrate measurable weakness and early fatigue during explosive hip extension activities or when ascending steep inclines.
Indications and Contraindications
The contemporary management of gluteal soft tissue sarcomas relies heavily on multidisciplinary tumor board consensus, integrating input from orthopedic oncology, medical oncology, radiation oncology, and musculoskeletal radiology. Approximately 90 percent of soft tissue sarcomas arising in the buttock can be adequately resected via limb-sparing surgery. Low-grade sarcomas generally require surgical resection alone, provided wide (R0) margins are achievable. High-grade sarcomas necessitate a multimodal approach, typically involving neoadjuvant radiotherapy to consolidate the pseudocapsule and maximize local control, occasionally followed by systemic chemotherapy for large (>5 cm), deep, high-grade lesions.
While limb salvage is the primary objective, specific oncologic and anatomic factors dictate when amputation or radical hemipelvectomy becomes an absolute oncologic necessity. Direct sacral or iliac bone involvement is rare but often necessitates an amputation or a complex composite bone and soft tissue resection.
| Clinical Variable | Indications for Limb Salvage (Gluteus Resection) | Indications for Hemipelvectomy or Amputation |
|---|---|---|
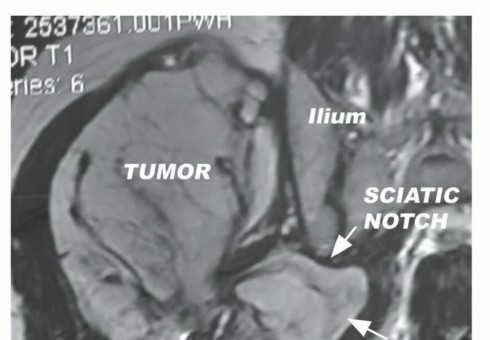
| Tumor Size and Location | Confined to gluteus maximus, displacing but not invading deep fascial structures | Massive tumors extending through the sciatic notch into the true pelvis or ischiorectal fossa |
| Sciatic Nerve Involvement | Nerve displaced by pseudocapsule; clear areolar tissue plane present on MRI | Circumferential encasement or direct epineural invasion by high-grade tumor precluding neurolysis |
| Bone Involvement | No osseous invasion; clear margins achievable at fascial boundaries | Direct invasion of the sacrum, ilium, or proximal femur requiring wide bony resection |
| Skin and Soft Tissue | Intact overlying skin or minimal involvement permitting primary closure or local flap | Massive fungation, ulceration, or gross infection precluding adequate soft tissue coverage |
| Vascular Involvement | Tumor confined above the level of the major pelvic vessels | Encasement of internal/external iliac vessels precluding safe reconstruction |
Pre Operative Planning and Patient Positioning
Thorough preoperative planning is critical to achieving negative oncologic margins while minimizing surgical morbidity and optimizing functional recovery.
Advanced Imaging and Biopsy Principles
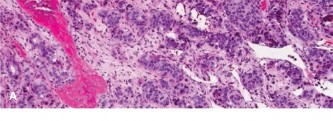
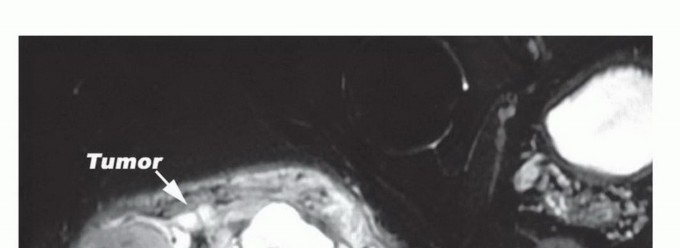
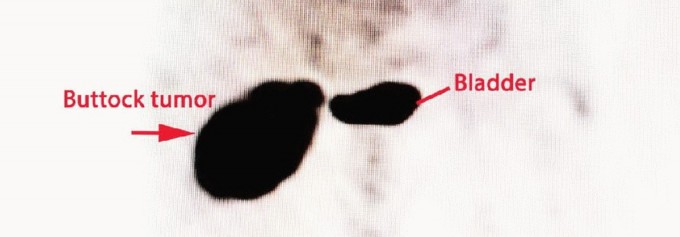
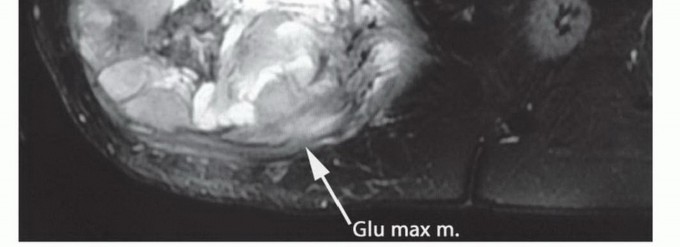
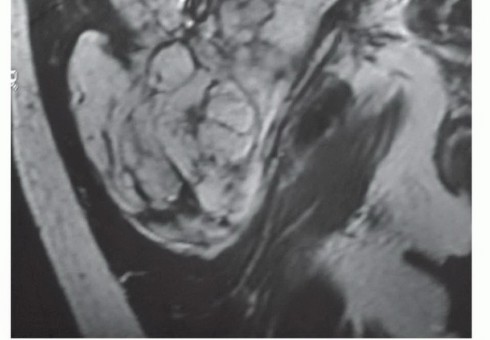
Magnetic Resonance Imaging (MRI) of the pelvis with and without intravenous contrast is the gold standard for local staging. T1-weighted images provide excellent anatomic detail regarding muscle involvement, fascial boundary integrity, and the displacement of the sciatic nerve. T2-weighted and STIR sequences are critical for highlighting peritumoral edema and the reactive zone, which must be encompassed within the surgical resection to avoid an intralesional margin. Contrast enhancement assists in differentiating viable tumor from a necrotic core. Computed Tomography (CT) of the chest is mandatory for systemic staging to rule out pulmonary metastasis, the most common site of dissemination for soft tissue sarcomas.
A core needle biopsy is strictly required to establish the histologic diagnosis and grade prior to definitive surgical intervention. The biopsy tract must be meticulously planned by the operating surgeon, not the interventional radiologist in isolation. The tract must be placed within the planned surgical incision so that it can be excised en bloc with the tumor. Trans-gluteal biopsies must strictly avoid contaminating the retrogluteal space, the sciatic nerve, or previously uninvolved fascial compartments.
Patient Positioning and Preparation
The procedure can be performed with the patient in either the lateral decubitus or the prone position, depending on the exact topographic location of the tumor and surgeon preference. The lateral decubitus position allows for excellent access to the posterior ilium, the greater trochanteric insertion, and the anterior thigh if flap mobilization is required. The prone position provides symmetric access to the sacrum and bilateral gluteal regions, which is advantageous for massive, midline-approaching tumors.
The entire hemipelvis, lower back, and ipsilateral lower extremity down to the knee should be prepped and draped free. This allows for dynamic intraoperative manipulation of the hip (flexion and extension), which can relax the sciatic nerve and facilitate complex deep dissection. A Foley catheter is placed to monitor urine output and hemodynamic status during the procedure.
Detailed Surgical Approach and Technique
The overriding surgical objective is an en bloc resection of the gluteus maximus muscle, encompassing the tumor, its reactive pseudocapsule, and the biopsy tract, while meticulously preserving the sciatic nerve and underlying short external rotators.
Incision and Flap Elevation
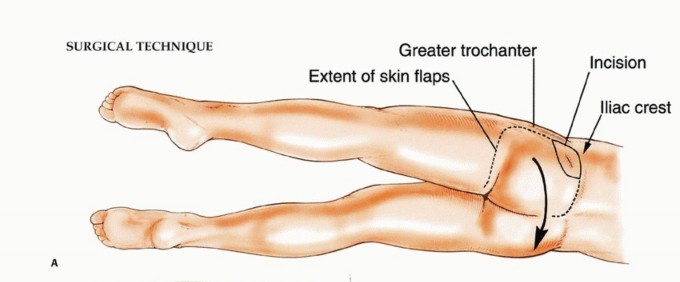
The skin incision is designed as a generous ellipse that unequivocally incorporates the previous biopsy tract. The orientation of the ellipse depends on the tumor geometry but generally follows the oblique fibers of the gluteus maximus, extending from the posterior superior iliac spine (PSIS) toward the greater trochanter and proximal femur.
Thick fasciocutaneous flaps are raised medially and laterally. It is critical to maintain a robust thickness of the subcutaneous fat on the skin flaps to prevent postoperative skin necrosis, particularly in the setting of neoadjuvant radiotherapy where microvascular compromise is already present. The dissection is carried down to the superficial investing fascia of the gluteus maximus, ensuring the fascia remains intact on the specimen side.

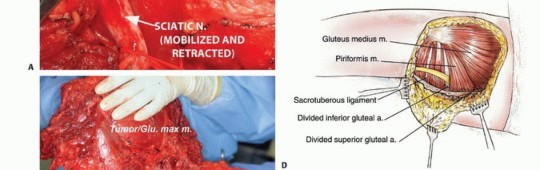
Identification and Isolation of the Sciatic Nerve
The most critical and technically demanding step in the procedure is the safe identification and mobilization of the sciatic nerve. The standard oncologic principle is to identify the nerve in an area of normal, unviolated anatomy, away from the tumor mass, and trace it toward the lesion. The nerve is typically located distally, deep to the inferior border of the gluteus maximus and superficial to the adductor magnus, midway between the ischial tuberosity and the greater trochanter.
Once identified distally, the nerve is carefully traced proximally into the retrogluteal space. Vessel loops can be used for gentle retraction, avoiding excessive traction neuropraxia. As the dissection proceeds proximally, the loose areolar tissue separating the deep surface of the gluteus maximus from the sciatic nerve and short external rotators is gently separated. If the tumor pseudocapsule intimately approaches the nerve, meticulous epineural dissection under loupe magnification may be required. Sharp dissection with a scalpel or dissecting scissors is strongly preferred over blunt avulsion to prevent nerve injury and ensure a clean oncologic margin.
En Bloc Resection of the Gluteus Maximus
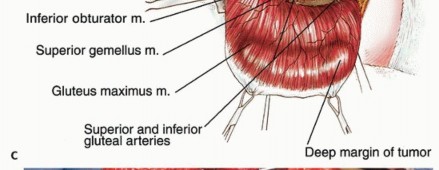
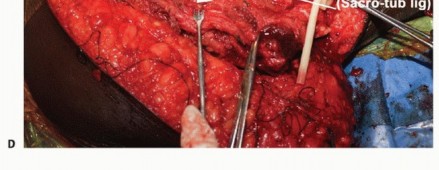
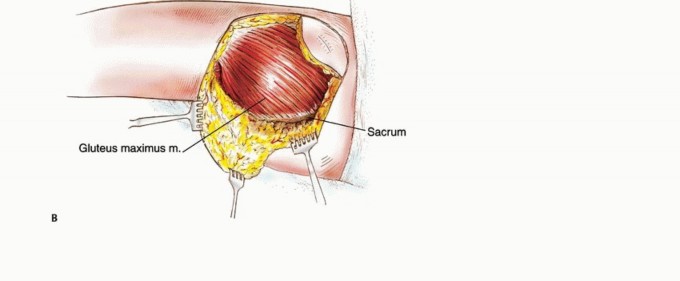
With the sciatic nerve fully protected and under direct visualization, the muscular attachments of the gluteus maximus are sequentially divided. The superior and lateral dissection involves dividing the broad insertion of the muscle into the iliotibial tract and the gluteal tuberosity of the femur. Releasing these lateral attachments first often allows the muscle belly to be reflected medially, dramatically improving visualization of the deep neurovascular structures.
Medially, the origin of the muscle is detached from the sacrum, the sacrotuberous ligament, and the posterior ilium using electrocautery. The inferior gluteal artery and vein are identified as they exit the greater sciatic foramen inferior to the piriformis. These vessels are carefully isolated, ligated with heavy silk sutures or titanium surgical clips, and transected. The entire gluteus maximus, containing the sarcoma surrounded by a cuff of normal muscle, is then removed en bloc. The specimen is immediately oriented and sent for pathologic margin assessment.
Hemostasis and Dead Space Management
Resection of the entire gluteus maximus creates a massive anatomic dead space over the posterior pelvis. Meticulous hemostasis is mandatory to prevent massive postoperative hematoma. The retroglute
Clinical & Radiographic Imaging

You Might Also Like