Acute Management of Pelvic Ring Fractures: A Surgical Guide
Key Takeaway
The acute management of unstable pelvic ring fractures requires rapid multidisciplinary intervention to control unrelenting hemorrhage. Initial stabilization utilizing a circumferential pelvic binder reduces pelvic volume and promotes tamponade. Comprehensive understanding of pelvic biomechanics, the posterior ligamentous tension band, and classification systems like Tile and Young-Burgess is essential for guiding definitive surgical fixation and optimizing patient survival in high-energy trauma.
INTRODUCTION TO PELVIC RING DISRUPTIONS
The acute management of a patient with a high-energy pelvic fracture and unrelenting hemorrhage remains one of the most formidable challenges to the orthopaedic trauma surgeon. These injuries are frequently the result of blunt, high-velocity trauma, such as motor vehicle collisions, motorcycle accidents, or falls from significant heights. Because the pelvis houses a rich vascular plexus and critical visceral structures, disruptions of the pelvic ring are associated with profound hemodynamic instability and high mortality rates.
A highly coordinated, multidisciplinary approach involving orthopaedic surgeons, general trauma surgeons, and anesthesiologists is critical to optimizing patient survival and functional outcomes. The "golden hour" of trauma resuscitation dictates that hemorrhage control and mechanical stabilization must occur simultaneously.
Clinical Pearl: The primary cause of early mortality in pelvic ring disruptions is exsanguinating hemorrhage, predominantly from the presacral venous plexus and branches of the internal iliac artery. Rapid mechanical stabilization of the pelvic volume is the most effective initial orthopaedic intervention.
SURGICAL ANATOMY AND BIOMECHANICS
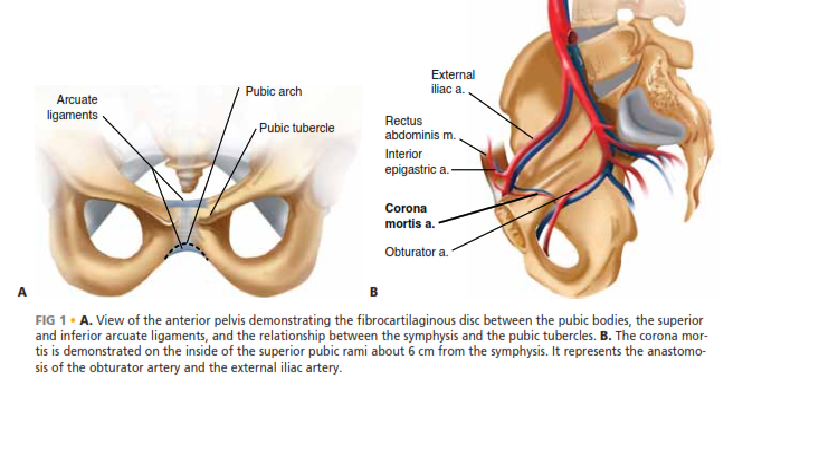
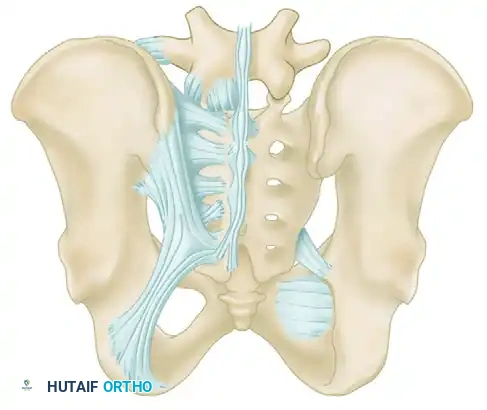
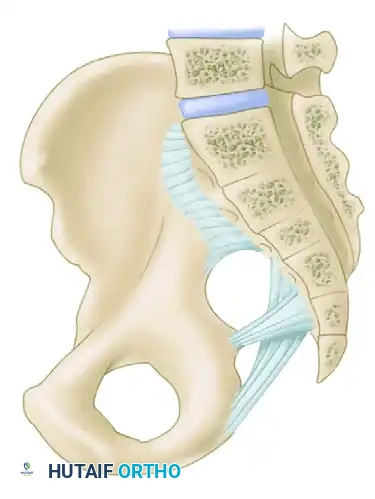
A profound understanding of pelvic osteoligamentous anatomy is the foundation of both classification and treatment. The pelvis is a ring structure composed anteriorly of the pubic and ischial rami connected at the symphysis pubis. A fibrocartilaginous disc separates the two pubic bodies, providing a degree of physiologic elasticity.
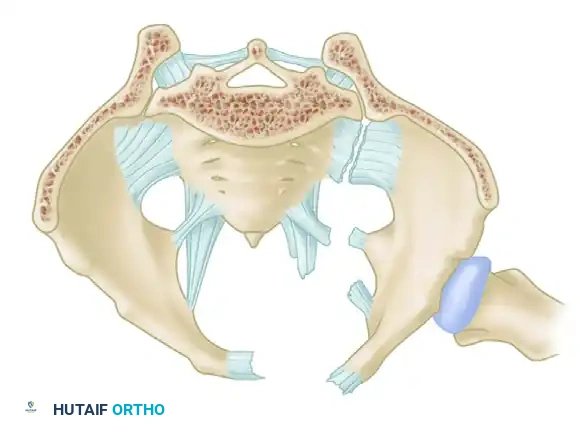
Posteriorly, the sacrum and the two innominate bones are joined at the sacroiliac (SI) joints. The SI joint itself possesses no inherent bony stability; its integrity relies entirely on a massive, complex ligamentous network.
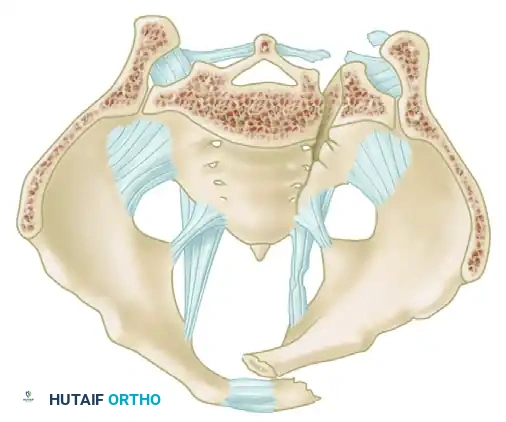
The Posterior Tension Band
The posterior ligamentous complex is the primary weight-bearing and stabilizing structure of the pelvis. Tile famously compared the relationship of the posterior pelvic ligamentous and bony structures to a suspension bridge, with the sacrum suspended securely between the two posterior superior iliac spines.
The critical ligaments include:
* Interosseous Sacroiliac Ligaments: The strongest ligaments in the body, forming the primary restraint to vertical shear forces.
* Anterior and Posterior Sacroiliac Ligaments: Provide rotational stability to the SI joint.
* Sacrotuberous Ligaments: Resist rotation in the sagittal plane (flexion of the sacrum).
* Sacrospinous Ligaments: The primary restraints to external rotation of the hemipelvis.
* Iliolumbar Ligaments: Connect the L5 transverse process to the iliac crest, augmenting vertical and rotational stability.
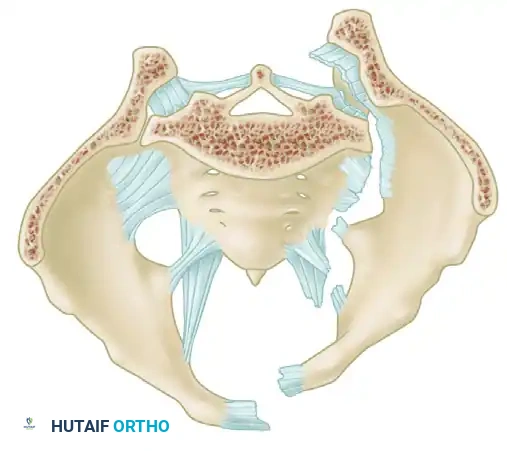
Biomechanical Restraints
Pelvic stability is determined by these ligamentous structures acting across various planes. The primary restraints to external rotation (the "open book" deformity) are the ligaments of the symphysis, the sacrospinous ligament, and the anterior sacroiliac ligament. Vertical displacement of the hemipelvis is controlled by all the aforementioned structures. However, if the anterior structures are disrupted, vertical stability may still be maintained by intact interosseous sacroiliac, posterior sacroiliac, and iliolumbar ligaments.
Surgical Warning: A rotationally unstable hemipelvis may remain vertically stable due to an intact posterior tension band. Recognizing this distinction is paramount, as it dictates whether the patient requires simple anterior stabilization or complex posterior ring reconstruction.
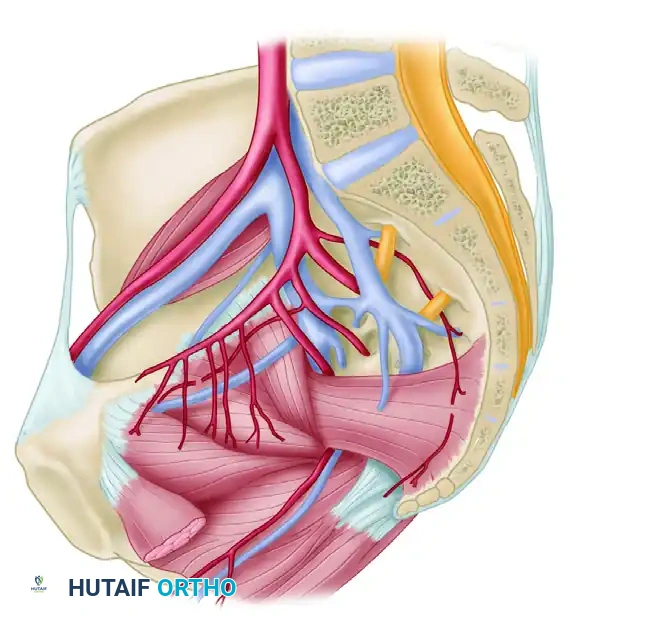
Vascular Anatomy
The internal iliac plexus of arteries and veins lies in intimate proximity to the anterior sacrum and sacroiliac joints. Disruption of the posterior ring frequently tears the thin-walled presacral venous plexus, leading to massive retroperitoneal hemorrhage. Arterial bleeding, typically from the superior gluteal or internal pudendal arteries, occurs in approximately 10-15% of hemodynamically unstable patients and requires emergent angioembolization.
INITIAL TRAUMA MANAGEMENT AND RESUSCITATION
The initial trauma workup must strictly adhere to Advanced Trauma Life Support (ATLS) protocols. Following the primary survey (Airway, Breathing, Circulation), the identification of a mechanically unstable pelvis in a hypotensive patient demands immediate action.
Diagnostic adjuncts, including a portable anteroposterior (AP) radiograph of the pelvis, Focused Assessment with Sonography for Trauma (FAST) of the abdomen, and potentially supraumbilical diagnostic peritoneal lavage (DPL), must rapidly rule out other sources of bleeding. If the patient is hemodynamically stable, a high-resolution CT scan of the chest, abdomen, and pelvis is mandatory.
The Circumferential Pelvic Binder
Upon clinical or radiographic recognition of an unstable pelvic ring injury, the immediate application of a circumferential pelvic binder is routine. First described in the literature by Routt et al., this technique involves wrapping a bed sheet or a commercially available binder around the pelvis.
Application Technique:
1. The binder must be centered directly over the greater trochanters, not over the iliac crests or abdomen.
2. Circumferential tension is applied to internally rotate the hemipelves.
3. The binder is clamped or secured via its proprietary mechanism.
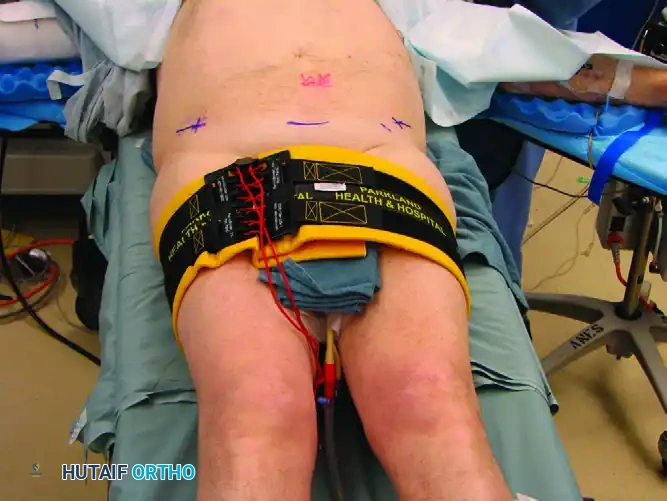


Mechanism of Action:
Binding theoretically reduces intrapelvic volume, stabilizes raw bleeding fracture surfaces, and encourages retroperitoneal tamponade. In the acute resuscitation stage, circumferential pelvic binding is preferred over external fixation due to its ease, non-invasiveness, and rapid application. Croce et al. demonstrated a significantly decreased need for blood transfusions following the implementation of institutional binding protocols.
Pitfall: Placing the pelvic binder too high (over the iliac wings) can paradoxically open the true pelvis further, exacerbating hemorrhage and worsening the deformity in lateral compression injuries.
EVALUATION OF OPEN PELVIC FRACTURES
Open pelvic fractures carry a mortality rate approaching 30-50%, primarily due to the combination of massive hemorrhage and overwhelming pelvic sepsis. Routine vaginal and rectal examinations are mandatory in all patients with suspected pelvic fractures, as sharp bony fragments can easily penetrate these structures. Failure to recognize an occult open fracture can lead to devastating necrotizing infections.
Fecal Diversion and Faringer Zones
The decision to perform a diverting colostomy depends on the anatomical location of the open wound. Faringer et al. anatomically classified open pelvic wounds into three distinct zones to guide selective fecal diversion:
- Zone I (Perineum, Rectum, Anus): High risk of fecal contamination. Routine diverting colostomy is strongly indicated.
- Zone II (Anterior Groin, Medial Thigh): Selective diversion is recommended, particularly if wounds extend deep into the subcutaneous fat or if large avulsion flaps with ischemic tissue are present.
- Zone III (Posterior Gluteal, Iliac Crest): Diversion is rarely required unless there is direct communication with the rectum.



Early application of an external fixator in open fractures minimizes fracture motion, protects the fragile soft tissue envelope, and facilitates nursing care and repeated wound debridements.
CLASSIFICATION OF PELVIC RING INJURIES
Classification systems are essential for predicting associated morbidities, guiding resuscitation, and determining definitive surgical management.
The Bucholz Classification
In a classic postmortem study of 150 fatal motor vehicle accidents, Bucholz identified pelvic fractures in 31% of victims and separated them into three foundational groups:
* Group I: Displaced anterior ring injuries with minimally displaced, stable sacral fractures or incomplete tearing of the anterior sacroiliac ligament.
* Group II: Anterior injuries associated with a rotational opening of the sacroiliac joint (disruption of anterior SI ligaments), but sparing the posterosuperior sacroiliac ligament complex.
* Group III: Complete disruption of both the anterior and posterior hemipelvis.
The Tile Classification
Tile modified the mechanistic Pennal system to create a comprehensive alphanumeric classification based on the concept of pelvic stability. This system remains the gold standard in modern orthopaedic literature.
Type A: Stable (Posterior Arch Intact)
* A1: Avulsion injuries (e.g., ASIS, AIIS, ischial tuberosity) not involving the true pelvic ring.
* A2: Stable fractures of the pelvic ring with minimal displacement (common in low-energy geriatric falls).
* A3: Transverse lesions of the sacrum and coccyx (often treated as spinal injuries).
Type B: Rotationally Unstable, Vertically Stable
* B1 (Open Book): External rotation or anteroposterior compression forces disrupt the symphysis and anterior SI ligaments. The posterior interosseous ligaments remain intact, preventing vertical shear.
* B2 (Lateral Compression): Internal rotation forces implode the hemipelvis.
* B2-1: Ipsilateral anterior and posterior injuries.
* B2-2: Contralateral (bucket-handle) injuries.
* B3: Bilateral rotationally unstable injuries.
Type C: Rotationally and Vertically Unstable
Complete disruption of the posterior arch, including the interosseous SI ligaments.
* C1: Unilateral complete disruption (iliac fracture, SI fracture-dislocation, or sacral fracture).
* C2: Bilateral injury, with one side Type B and one side Type C.
* C3: Bilateral Type C injuries (complete dissociation of the sacrum from the pelvis).
The Young and Burgess Classification
Young and Burgess proposed a mechanistic classification based on the primary energy vectors: Anteroposterior Compression (APC), Lateral Compression (LC), and Vertical Shear (VS). This system correlates strongly with resuscitation needs; for example, APC II and III injuries have the highest transfusion requirements, while LC injuries are highly associated with closed head injuries and visceral trauma.
RADIOGRAPHIC EVALUATION
Standard radiographic evaluation begins with the AP pelvis view in the trauma bay. Once the patient is stabilized, specialized views and advanced imaging are required.
- Inlet View: Directed 45 degrees caudally. Excellent for assessing posterior displacement of the hemipelvis, sacral impaction, and internal/external rotational deformity.
- Outlet View: Directed 45 degrees cephalad. Ideal for evaluating vertical displacement of the hemipelvis and sacral foraminal fractures.
The Role of Computed Tomography (CT)
CT is an absolute requirement for the evaluation of any significant pelvic injury. It allows precise evaluation of the posterior pelvic ring, which is often obscured by bowel gas or patient habitus on plain radiographs. CT identifies minimally displaced fracture lines extending into the acetabulum, sacral dysmorphism, and the exact location of posterior ring comminution, all of which dictate the surgical approach and implant selection.
Radiographic Signs of Instability:
* Symphyseal widening > 2.5 cm correlates with rupture of the sacrospinous ligament and rotational instability.
* Avulsion fractures of the lateral sacrum or ischial spine indicate severe ligamentous failure.
* L5 transverse process fractures indicate avulsion of the iliolumbar ligament, a hallmark of vertical instability (Tile C / Vertical Shear).
PATIENT POSITIONING AND SURGICAL APPROACHES
Definitive surgical management is undertaken once the patient is hemodynamically optimized, the "lethal triad" (coagulopathy, hypothermia, acidosis) is corrected, and soft tissues are amenable to incision.
Positioning
The choice of patient positioning depends entirely on the fracture pattern and the planned surgical approach.
- Supine Position: Utilized for anterior ring fixation (symphyseal plating, superior pubic ramus screws) and percutaneous iliosacral screw fixation. A radiolucent table is mandatory to allow unobstructed fluoroscopic imaging (Inlet, Outlet, and Lateral sacral views).
- Prone Position: Indicated for direct open reduction and internal fixation of displaced sacral fractures or complex sacroiliac joint fracture-dislocations requiring posterior tension band plating.
- Lithotomy Position: Occasionally utilized for complex perineal debridements or combined urologic/orthopaedic procedures.
Surgical Approaches
- Pfannenstiel Approach: The workhorse for symphysis pubis diastasis. A transverse incision is made 2 fingerbreadths proximal to the symphysis. The rectus abdominis is split along the linea alba to expose the pubic bodies.
- Modified Stoppa Approach: An extensile anterior intrapelvic approach used for complex anterior ring fractures extending into the quadrilateral plate or acetabulum.
- Posterior Approaches: Longitudinal or transverse incisions over the PSIS and sacrum allow direct visualization of the SI joint and sacral lamina for decompression and plating.
POSTOPERATIVE PROTOCOLS AND REHABILITATION
The postoperative management of pelvic ring injuries requires a delicate balance between protecting the surgical fixation and mobilizing the polytraumatized patient to prevent systemic complications.
- Weight-Bearing Status: Patients with isolated anterior ring injuries (Tile B1/B2) treated with rigid fixation may be allowed protected toe-touch weight-bearing. Patients with vertically unstable injuries (Tile C) typically require strict non-weight-bearing precautions on the affected side for 8 to 12 weeks to prevent catastrophic hardware failure and loss of reduction.
- DVT Prophylaxis: Pelvic trauma patients are at an exceptionally high risk for deep vein thrombosis and fatal pulmonary embolism. Chemical prophylaxis (e.g., Low Molecular Weight Heparin) should be initiated as soon as intracranial and intrapelvic bleeding risks have normalized, typically within 24-48 hours post-injury, and continued for a minimum of 4 weeks.
- Radiographic Follow-up: Serial radiographs (AP, Inlet, Outlet) are obtained at 2, 6, and 12 weeks to monitor for hardware loosening, loss of reduction, and progressive fracture consolidation.
By adhering to strict ATLS protocols, utilizing rapid mechanical stabilization techniques, and applying a deep understanding of pelvic biomechanics, the orthopaedic surgeon can successfully navigate the acute management of these devastating injuries and set the stage for optimal definitive reconstruction.
You Might Also Like