When Supracondylar Fractures Must Be Treated With Open Reduction
Key Takeaway
Your ultimate guide to When Supracondylar Fractures Must Be Treated With Open Reduction starts here. A supracondylar fracture requiring open reduction cannot be effectively managed with closed reduction and percutaneous pinning. Indications include an open fracture, irreducible fractures by closed techniques, or a compromised vascular supply to the hand. These complex fractures are typically **treated with open** surgical methods, often involving a transverse anterior incision in the antecubital fossa, to restore proper alignment and protect neurovascular structures.
Introduction and Epidemiology
Supracondylar humeral fractures (SCHF) represent the most common elbow fracture in pediatric populations, typically occurring between the ages of 5 and 7 years. The predominant mechanism involves a fall onto an outstretched hand with the elbow in hyperextension, resulting in an extension-type fracture. These injuries account for approximately 60% of all pediatric elbow fractures and carry a significant risk of neurovascular compromise and long-term sequelae if not managed appropriately.
The Gartland classification system, which categorizes these fractures based on radiographic displacement, is universally employed to guide treatment decisions. Gartland type I fractures are non-displaced; type II involve displacement with an intact posterior cortex hinge; type III are completely displaced with no cortical contact; and type IV, a more recently recognized variant, exhibit multidirectional instability post-reduction attempts, implying complete periosteal disruption.
While the vast majority of displaced SCHF (Gartland type II, III, and IV) are amenable to closed reduction and percutaneous pinning (CRPP), which has become the gold standard due to its minimally invasive nature and excellent outcomes, a critical subset of these fractures necessitates open reduction. This typically occurs in situations where closed techniques fail to achieve or maintain an acceptable reduction, or when there are critical neurovascular complications. Open reduction of a supracondylar fracture of the humerus, though less common, is a technically demanding procedure requiring precise anatomical knowledge and surgical skill to mitigate potential complications and restore optimal elbow function. This chapter outlines the indications, surgical approaches, technical considerations, and potential pitfalls associated with open reduction for pediatric supracondylar humeral fractures.
Surgical Anatomy and Biomechanics
A thorough understanding of the regional anatomy, encompassing bony architecture, neurovascular structures, and surrounding soft tissues, is paramount for safe and effective open reduction. The inherent complexity of the distal humerus, combined with the susceptibility of pediatric bone to specific fracture patterns, mandates careful consideration during surgical planning and execution.
Bony Anatomy of the Distal Humerus
The distal humerus transitions from the relatively cylindrical shaft to the flattened condylar portion, forming the articular surface of the elbow. Key features include the medial and lateral epicondyles, the trochlea (articulating with the ulna), and the capitellum (articulating with the radial head). The supracondylar region, proximal to the olecranon and coronoid fossae, is a relatively thin and metaphyseal segment, making it susceptible to fracture. In extension-type fractures, the distal fragment typically displaces posteriorly, often with varus or valgus angulation and internal or external rotation relative to the proximal shaft. The metaphyseal flare provides intrinsic stability upon reduction, but significant comminution or displacement can disrupt this. Growth plates, particularly the capitellar physis and the distal humeral trochlear physis, must be recognized to avoid iatrogenic injury.
Neurovascular Anatomy of the Elbow Region
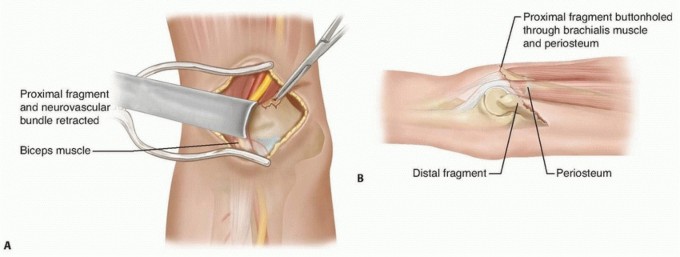
The neurovascular bundle in the antecubital fossa is particularly vulnerable in displaced supracondylar fractures, especially those with significant anterior displacement of the proximal fragment or posterior displacement of the distal fragment, leading to a "buttonholing" effect through the brachialis muscle.
- Brachial Artery and Median Nerve: These structures course anteriorly over the distal humerus. The brachial artery typically lies medial to the median nerve in the upper arm, crossing anteriorly to the nerve as it enters the antecubital fossa. Both are often immediately subcutaneous anteriorly in cases of significant fracture displacement, placing them at high risk during the skin incision for an anterior approach. The median nerve also gives off the anterior interosseous nerve distally. Ischemic contracture (Volkmann's contracture) is a devastating complication arising from brachial artery compromise.
- Radial Nerve: The radial nerve courses from posterior to anterior in the spiral groove of the humerus, then pierces the lateral intermuscular septum approximately 10 cm proximal to the lateral epicondyle. It then lies anterior to the lateral epicondyle, dividing into deep (posterior interosseous) and superficial branches distal to the capitellum. It is at risk during lateral approaches or in fractures with lateral displacement.
- Ulnar Nerve: The ulnar nerve passes posteriorly in the cubital tunnel, behind the medial epicondyle. It is particularly vulnerable during medial approaches or with medial column fractures and medial pin placement during percutaneous pinning. Careful identification and protection are mandatory.
Muscular and Soft Tissue Considerations
The brachialis muscle originates from the anterior aspect of the distal humerus and inserts onto the coronoid process and ulnar tuberosity. In displaced supracondylar fractures, the proximal humerus fragment can pierce and become entrapped within the brachialis muscle, preventing closed reduction. Periosteum, typically the posterior periosteal hinge, often aids in closed reduction but can be completely disrupted in Gartland type IV fractures. In rare cases, a buttonholed periosteal sleeve can also obstruct reduction.
Biomechanics of Irreducibility
Irreducibility by closed techniques arises from several factors:
1. Soft Tissue Interposition: The most common cause, frequently involving the brachialis muscle, sometimes the median nerve or brachial artery itself.
2. Periosteal Entrapment: A torn periosteal flap can become incarcerated in the fracture site.
3. Significant Comminution: Extensive comminution, particularly of the columns, can preclude stable reduction.
4. Buttonholing: The proximal fracture fragment can penetrate and become "buttonholed" through the anterior soft tissues, including the brachialis muscle and sometimes the neurovascular bundle, making disengagement difficult.
5. Severe Displacement or Rotational Malalignment: Extreme displacement, especially with significant rotation, may be resistant to external manipulation.
These biomechanical considerations underscore the importance of a systematic approach to fracture assessment and reduction.
Indications and Contraindications
The decision to proceed with open reduction for a supracondylar humeral fracture is based on specific clinical and radiographic findings that preclude successful closed management. While closed reduction and percutaneous pinning (CRPP) remains the treatment of choice for the vast majority of displaced supracondylar fractures, open reduction is reserved for challenging scenarios to ensure anatomical reduction and minimize long-term morbidity.
Primary Indications for Open Reduction
- Irreducibility by Closed Techniques: This is the most common indication. Failure to achieve or maintain acceptable reduction after multiple, judicious closed attempts under general anesthesia is a clear mandate for open intervention. Acceptable reduction is generally defined as less than 3 mm of displacement, less than 5-10 degrees of varus/valgus angulation, and less than 10-15 degrees of sagittal plane angulation (extension/flexion) with adequate rotational control. Soft tissue interposition (e.g., brachialis muscle, median nerve, brachial artery, periosteum) is a frequent cause of irreducibility.
- Compromised Vascular Supply to the Hand:
- "Pulseless pale" hand with signs of ischemia: This is an orthopedic emergency. Immediate open exploration of the brachial artery is required. This involves identifying the site of compression or injury, releasing any soft tissue impingement, and if necessary, repairing a lacerated artery or performing a vascular bypass/graft. Fracture reduction and stabilization must occur concomitantly to prevent re-injury or kinking of the repair.
- "Pulseless pink" hand that does not reconstitute with closed reduction: If, after achieving what appears to be an acceptable closed reduction and pinning, the radial pulse (assessed by Doppler) remains absent, and there are other signs suggestive of compromised perfusion (e.g., increased capillary refill time, decreased temperature gradient), open exploration of the brachial artery should be considered. While some "pulseless pink" hands can be managed by observation, persistent absent pulses after stable reduction warrant cautious vigilance and a low threshold for exploration, particularly if a significant intimal tear or thrombosis is suspected.
- Open Fractures: Any supracondylar fracture with a breach in the skin communicating with the fracture site necessitates open surgical debridement to reduce the risk of infection. This often dictates open reduction for cleaning, irrigation, and direct visualization of the fracture site before stabilization. The Gustilo-Anderson classification guides the extent of debridement.
- Concomitant Injuries Requiring Open Exposure: Rare instances, such as a severe compartment syndrome requiring fasciotomy or an open nerve injury requiring direct repair, may necessitate open reduction of the fracture through the same surgical field.
Relative Indications
- Delayed Presentation with Early Callus Formation: If a child presents several days after injury with significant swelling and early callus formation that prevents closed reduction, open reduction may be required. However, for chronic malunion, a formal corrective osteotomy is often a better approach than attempting open reduction through a healing fracture.
- Gartland Type IV Fractures: While initially attempted with closed reduction, the inherent multi-directional instability and complete periosteal disruption in type IV fractures frequently lead to irreducibility or instability post-reduction, requiring open techniques.
Contraindications for Open Reduction
- Successful Closed Reduction and Stable Percutaneous Pinning: This is the primary and preferred treatment for most displaced supracondylar fractures. If an anatomical or acceptably stable reduction can be achieved and maintained with percutaneous pins, open reduction is unnecessary and introduces additional risks.
- Stable Fracture Patterns: Gartland type I fractures, or those type II fractures with minimal displacement and a stable posterior hinge, can often be managed non-operatively with casting alone.
- Extremely Comminuted Fractures: In rare cases of severe comminution, particularly in the articular surface, open reduction may lead to excessive soft tissue stripping and devitalization of fragments, potentially worsening outcomes. While pin fixation is still typically performed, the extent of open reduction for truly comminuted fragments must be balanced against the risk of nonunion or avascular necrosis.
- Patient Unsuitability for General Anesthesia: While rare in pediatric trauma, severe comorbidities that contraindicate general anesthesia would preclude open surgery.
The following table summarizes the operative versus non-operative indications:
| Feature | Operative (Open Reduction) Indications | Non-Operative (Closed Reduction/Pinning) Indications |
|---|---|---|
| Fracture Type | Open fractures (Gustilo-Anderson) | Gartland Type I, II (stable/unstable), III (reducible), IV (reducible) |
| Reducibility | Irreducible by closed reduction techniques | Reducible by closed reduction maneuvers |
| Neurovascular Status | Compromised vascular status (ischemia, pulseless pale hand, pulseless pink hand not reperfusing with CR), iatrogenic neurovascular injury | Intact or transient neurological deficit (neurapraxia) with stable perfusion |
| Soft Tissue | Significant soft tissue interposition (e.g., brachialis) | Minimal to no soft tissue interposition |
| Other Injuries | Concomitant injuries requiring open exposure (e.g., compartment syndrome) | Isolated supracondylar fracture without other urgent operative indications |
| Timing | Urgent (vascular compromise, open fracture) or Elective (irreducibility) | Urgent (within 24 hours often preferred, up to 72 hours if no vascular compromise) |
Pre Operative Planning and Patient Positioning
Meticulous preoperative planning is essential for optimizing surgical outcomes and minimizing complications, particularly in cases requiring open reduction. This phase includes patient assessment, advanced imaging where necessary, discussion of timing, and careful setup of the operating room environment.
Initial Assessment and Resuscitation
For all pediatric trauma patients, an initial assessment following Advanced Trauma Life Support (ATLS) principles is paramount, especially for open fractures or those with vascular compromise. Pain management, temporary splinting, and assessment of potential concomitant injuries are performed. A detailed neurovascular examination, including palpation of radial and ulnar pulses, capillary refill time, and assessment of median, ulnar, and radial nerve function (motor and sensory), must be meticulously documented. This baseline assessment is critical for identifying new deficits post-operatively.
Imaging Studies
Standard imaging includes orthogonal AP and true lateral radiographs of the elbow. These films allow assessment of fracture type (Gartland), degree of displacement, angulation, and rotation. The anterior humeral line and Baumann's angle are key radiographic measurements for assessing fracture reduction. Oblique views may be helpful to further characterize comminution or displacement.
Computed tomography (CT) scans are rarely indicated for standard supracondylar fractures but may be considered in very complex cases with suspected articular involvement, large osteochondral fragments, or if 3D planning is deemed beneficial for highly unusual fracture patterns. Magnetic resonance imaging (MRI) has no routine role. Arteriography is generally not required; in cases of suspected vascular injury, direct surgical exploration is often the most expeditious and diagnostic approach. A Doppler ultrasound can be useful pre- and intra-operatively to confirm arterial flow.
Timing of Intervention
The timing for surgical intervention in supracondylar fractures remains a topic of debate, but clear principles guide open reduction cases.
* Urgent Indications: Open fractures and all cases with compromised vascular supply (pulseless pale hand or pulseless pink hand not reconstituting with closed reduction) require immediate, emergent surgical intervention. Delay in these scenarios significantly increases the risk of infection, limb ischemia, and potential amputation.
* Elective Indications: For irreducible closed fractures without vascular compromise, the timing can be more flexible. While many surgeons advocate for prompt reduction, studies suggest that a delay of up to 12-24 hours, or even longer in select cases without significant swelling, does not significantly increase complication rates, provided the neurovascular status remains stable. This allows for adequate swelling reduction and optimization of surgical resources. However, undue delay, particularly with increasing swelling, can make even open reduction more challenging.
Anesthesia Considerations
General anesthesia is the standard for pediatric supracondylar fracture surgery. Regional anesthesia, such as a supraclavicular or axillary block, can be a useful adjunct for post-operative pain management, reducing opioid requirements. An anesthesiologist experienced in pediatric care is crucial.
Patient Positioning and Surgical Setup
The patient is positioned supine on a radiolucent operating table. The injured arm is placed on a hand table or arm board, allowing full range of motion of the shoulder and elbow. A well-padded tourniquet is applied to the upper arm. The C-arm fluoroscopy unit is positioned to allow immediate acquisition of true AP and lateral views of the elbow without requiring patient or arm repositioning. This is critical for efficient intraoperative assessment of reduction and pin placement. The entire arm, including the axilla and hand, should be prepped and draped to allow for potential extension of the incision, proximal vascular exposure, or assessment of distal neurovascular status.
A crucial preoperative step for children with a severe, potentially irreducible fracture, as noted in the seed content, is to make a provisional attempt at fracture reduction immediately after the induction of anesthesia. After milking the fracture from its entrapment in the brachialis muscle, standard reduction maneuvers are performed to reduce the distal fragment into generally good alignment. Although time should not be spent perfecting the reduction (which will likely be lost during prepping and draping), this provisional reduction of severe fractures after induction can alert the surgical team that open reduction may be necessary if closed methods are futile. This initial attempt helps confirm the diagnosis of irreducibility and prepares the team for potential open conversion.
Detailed Surgical Approach and Technique
When open reduction is mandated, selecting the appropriate surgical approach is critical to facilitate reduction, protect vital structures, and achieve stable fixation. The anterior approach (Henry approach) is generally favored for irreducible extension-type supracondylar fractures due to its direct access to the fracture site and the neurovascular bundle.
Tourniquet Application and Skin Preparation
After positioning, the upper arm is exanguinated, and the tourniquet is inflated to appropriate pressure. The entire arm is prepped and draped in a sterile fashion, ensuring the ability to visualize the shoulder, elbow, and hand to allow for neurovascular assessment and potential extension of the surgical field.
Incision Selection and Planning
-
Anterior Approach (Henry Approach): This is the most common and versatile approach for irreducible extension-type supracondylar fractures, particularly when neurovascular compromise or soft tissue interposition is suspected.
- Skin Incision: A longitudinal or gentle S-shaped incision is made on the anterior aspect of the distal humerus, centered over the antecubital fossa. It typically extends from approximately 5-7 cm above the fracture line to 2-3 cm distal to the elbow crease. Careful deepening of the incision is paramount.
- Subcutaneous Dissection: The subcutaneous tissue is incised, and meticulous hemostasis is achieved. The brachial artery and median nerve are often found immediately deep to the subcutaneous fat, especially with significant fracture displacement. They must be carefully identified and protected. The median nerve typically lies medial to the brachial artery at the level of the fracture.
- Fascial Incision: The bicipital aponeurosis and deep fascia are incised longitudinally.
-
Medial Approach: Less commonly used for typical extension-type fractures, this approach is reserved for specific situations like severe medial column comminution, medial epicondyle involvement, or persistent medial displacement. The primary risk is to the ulnar nerve. An incision is made along the medial supracondylar ridge. The ulnar nerve must be identified and carefully retracted posteriorly within the cubital tunnel.
-
Lateral Approach: Also less common, indicated for severe lateral column involvement or lateral displacement. An incision is made along the lateral supracondylar ridge. The radial nerve (posterior interosseous nerve branch) and brachioradialis/brachialis muscles are at risk.
Soft Tissue Dissection and Release (Anterior Approach)
After carefully identifying and protecting the median nerve and brachial artery, these structures are gently retracted, usually medially or laterally depending on the pathology. The brachialis muscle, which often entraps the proximal fragment, is visualized. The torn and interposed fibers of the brachialis muscle are carefully dissected and released from the fracture site. Any interposed periosteum or hematoma is debrided. This direct visualization of the fracture site and release of soft tissue impediments are the key advantages of open reduction.

Figure: Illustration of an anterior approach revealing the entrapped brachial artery and median nerve within the fracture site, typical for irreducible supracondylar fractures.
Fracture Reduction
With direct visualization, the fracture fragments can be manipulated using gentle traction, reduction clamps, or small bone hooks. The goal is an anatomical reduction, restoring the anterior cortical alignment and minimizing gapping at the fracture site.
1. Disengagement: Apply longitudinal traction to disengage the proximal fragment from the brachialis muscle.
2. Correction of Rotational Deformity: Visualize the columns and correct any internal or external rotation.
3. Restoration of Alignment: Correct varus/valgus angulation and restore sagittal plane alignment. The anterior cortical line should be re-established.
4. Impacted Fractures: If the fracture is impacted, it may need to be disimpacted prior to reduction.
Once reduced, the fracture should appear stable to gentle manipulation. The integrity of the neurovascular structures must be reassessed after reduction.
Internal Fixation Strategy
Even after open reduction, percutaneous K-wire fixation remains the primary method of stabilization for pediatric supracondylar fractures. The choice between cross-pinning and lateral-entry pinning often depends on surgeon preference and the specific fracture pattern.
-
Cross-Pinning: Involves placing a lateral K-wire and a medial K-wire.
- Lateral Pin: Inserted from the lateral epicondyle, traversing the capitellum, across the fracture site, and into the medial column of the proximal humerus.
- Medial Pin: Inserted from the medial epicondyle, traversing the trochlea, across the fracture site, and into the lateral column of the proximal humerus. Crucially, the ulnar nerve must be identified and protected during medial pin insertion, often requiring a small incision for direct visualization of the nerve before pin placement.
- Advantages: Biomechanically very stable, particularly against rotational forces.
- Disadvantages: Risk of iatrogenic ulnar nerve injury with medial pin.
-
Lateral-Entry Pinning: Involves placing two or three divergent K-wires from the lateral epicondyle.
- Placement: Pins are inserted from the lateral epicondyle, aiming proximally and medially, ensuring divergence to achieve rotational stability. The first pin usually engages the medial cortex of the proximal humerus, while the second or third may engage the anterior or posterior medial cortex.
- Advantages: Minimizes the risk of ulnar nerve injury.
- Disadvantages: Potentially less rotational stability than cross-pinning if pins are not widely divergent.
K-wire size typically ranges from 1.6 mm to 2.0 mm, depending on the child's age and bone size. Pins should be placed bicortically for optimal stability. After pin placement, the ends are bent and cut, leaving them exposed or buried beneath the skin. Exposed pins facilitate easier removal in the clinic.

Figure: Fluoroscopic image demonstrating stable fixation with cross-pinning after open reduction, with acceptable alignment of the anterior humeral line.
Intraoperative Assessment
After fixation, the fracture reduction and stability are meticulously assessed using fluoroscopy in AP, lateral, and oblique views. The Baumann's angle and anterior humeral line are checked for appropriate alignment. The elbow is gently moved through a range of motion to confirm stability of the fixation.
Crucially, the neurovascular status of the hand must be re-evaluated. Radial and ulnar pulses are checked by palpation and Doppler ultrasound. Capillary refill and skin color are observed. If a vascular exploration was performed, the patency of the repair is confirmed. Any iatrogenic neurovascular injury must be identified immediately.

Figure: Postoperative lateral radiograph illustrating a well-reduced supracondylar fracture with internal fixation, demonstrating restoration of the anterior humeral line.
Wound Closure
The tourniquet is deflated, and meticulous hemostasis is achieved. The wound is irrigated. The deep fascia is closed, followed by the subcutaneous layers and skin, using absorbable sutures. A sterile dressing is applied, and the elbow is immobilized in a well-padded, bulky posterior plaster splint at approximately 60-90 degrees of flexion, tailored to maintain reduction and accommodate swelling.
Complications and Management
Open reduction of supracondylar humeral fractures, while often necessary, carries a higher rate of complications compared to closed reduction and percutaneous pinning. Vigilant monitoring and prompt management are crucial for mitigating adverse outcomes.
Neurovascular Injury
- Iatrogenic Nerve Injury: The most frequent nerve injured during open reduction is the median nerve due to its anterior location. The ulnar nerve is at risk with medial approaches or medial pin placement. The radial nerve is less commonly injured but is vulnerable with lateral approaches. Most iatrogenic nerve injuries are neurapraxias, which tend to resolve spontaneously over weeks to months. Persistent or severe deficits may warrant electrodiagnostic studies and, rarely, surgical exploration and repair.
- Vascular Injury: Brachial artery injury (laceration, transection, intimal tear, thrombosis) is a severe complication. A "pulseless pale" hand warrants immediate re-exploration and vascular surgical consultation for repair (e.g., primary repair, vein graft). Even after successful repair, compartment syndrome can develop, necessitating fasciotomy.
Infection
- Pin Site Infection: Superficial pin site infections are relatively common (5-10%), usually managed with local wound care and oral antibiotics.
- Deep Surgical Site Infection: Rare (<1%) but serious, requiring aggressive debridement, intravenous antibiotics, and potentially hardware removal once the fracture is stable. Open fractures inherently carry a higher infection risk.
Malunion and Nonunion
- Cubitus Varus (Gunstock Deformity): This is the most common long-term complication, occurring in 5-10% of cases, often due to inadequate initial reduction, particularly rotational or sagittal plane malalignment, or growth disturbance. While primarily a cosmetic deformity, it can rarely lead to tardy ulnar nerve palsy. Corrective osteotomy is reserved for severe, symptomatic deformities.
- Cubitus Valgus: Less common, typically resulting from growth disturbance of the medial physis or overgrowth of the lateral column.
- Torsional Deformities: Can lead to compensatory forearm rotation and functional limitations.
- Nonunion: Extremely rare in supracondylar fractures due to the rich blood supply and metaphyseal nature of the bone. When it occurs, it's typically associated with severe open injuries, infection, or inadequate fixation. Management involves debridement, bone grafting, and rigid internal fixation.
Loss of Reduction
Occurs in 2-5% of cases, primarily due to unstable fixation, early mobilization, or insufficient post-operative immobilization. Requires re-reduction and re-fixation.
Stiffness and Range of Motion Loss
Some degree of stiffness, particularly loss of terminal extension, is common post-open reduction, often resolving with time and physical therapy. Aggressive passive stretching should be avoided due to the risk of myositis ossificans. Persistent severe stiffness may require manipulation under anesthesia or, rarely, arthrolysis.
Myositis Ossificans
The formation of heterotopic bone within the soft tissues, especially the brachialis muscle, can occur, leading to decreased range of motion. It is associated with repeated forceful manipulations, excessive soft tissue dissection, and prolonged immobilization. Management is typically conservative, involving gentle range of motion exercises. Surgical excision is considered only after the heterotopic bone has matured (typically 6-12 months post-injury).
Compartment Syndrome
While not exclusive to open reduction, compartment syndrome is a critical complication that can arise from the initial injury, particularly with associated vascular compromise, or following surgical manipulation and swelling. Increased pain out of proportion to the injury, pain with passive stretch, paresthesia, pallor, and paralysis are hallmark signs. Requires emergency fasciotomy.
The following table summarizes common complications, their approximate incidence, and salvage strategies:
| Complication | Incidence (Approximate) | Salvage Strategy |
|---|---|---|
| Neurovascular Injury | 5-15% (iatrogenic or existing) | Observation (neurapraxia), exploration/repair (laceration), vascular repair/graft, fasciotomy |
| Cubitus Varus (Malunion) | 5-10% | Observation, corrective osteotomy for significant deformity |
| Pin Site Infection | 5-10% | Local wound care, oral antibiotics, pin removal |
| Deep Infection | <1% | Debridement, IV antibiotics, hardware removal (if stable fracture) |
| Loss of Reduction | 2-5% | Re-reduction, re-fixation, improved immobilization |
| Stiffness/ROM Loss | Up to 20% (initially) | Physical therapy, dynamic splinting, watchful waiting |
| Myositis Ossificans | <1% | Observation, gentle ROM, surgical excision (late, after maturation) |
| Compartment Syndrome | <1% | Emergency fasciotomy |
| Nonunion | Extremely rare | Debridement, bone grafting, rigid internal fixation |
Post Operative Rehabilitation Protocols
Post-operative rehabilitation following open reduction and internal fixation (ORIF) of a supracondylar humeral fracture is crucial for restoring function and preventing long-term complications. The protocol must balance protection of the healing fracture with early, controlled mobilization to prevent stiffness.
Immediate Postoperative Care
- Immobilization: The elbow is immediately immobilized in a well-padded, bulky posterior plaster splint or above-elbow cast. The elbow is typically maintained at approximately 60-90 degrees of flexion, and the forearm in neutral rotation, tailored to the fracture stability and reduction. The splint must not be too tight to avoid compromising circulation or increasing swelling.
- Elevation and Ice: The limb is kept elevated above heart level, and ice packs are applied intermittently to minimize swelling.
- Neurovascular Monitoring: Frequent neurovascular checks (hourly for the first 24-48 hours, then every 4 hours) are paramount. Assessment includes pain, pallor, pulses (radial, ulnar, brachial via Doppler), paresthesia, and paralysis (the "5 Ps"). Any changes must be reported immediately.
- Pain Management: Appropriate pain control with analgesics is administered.
- Pin Care: If K-wires are left exposed, meticulous pin site care is performed daily to prevent infection.
Immobilization Period (Typically 3-6 Weeks)
- Cast/Splint Changes: The initial splint may be converted to a lighter cast once initial swelling subsides, typically within the first week.
- Radiographic Follow-up: Serial radiographs (AP and lateral) are taken at regular intervals (e.g., 1, 2, 4 weeks) to monitor fracture healing and ensure maintenance of reduction and pin integrity.
- Pin Removal: K-wires are typically removed in the clinic once there is clinical and radiographic evidence of adequate fracture healing, usually around 3-4 weeks post-surgery. Premature removal can lead to loss of reduction; delayed removal increases the risk of pin site infection and re-fracture during removal.
Rehabilitation Post-Pin Removal
The goal of this phase is to gradually restore full, pain-free range of motion (ROM) and strength.
- Gentle Active Range of Motion (AROM): Once pins are removed, the child is encouraged to begin gentle, active range of motion exercises of the elbow and forearm. This includes flexion, extension, pronation, and supination. These exercises should be initiated without pain or resistance.
- Avoid Aggressive Passive Stretching: Aggressive passive stretching or forced manipulation should be strictly avoided in the early phase to minimize the risk of myositis ossificans, especially after open reduction. The focus is on natural, gentle restoration of motion.
- Progressive Loading: As ROM improves and pain subsides, strengthening exercises for the elbow, forearm, and grip can be introduced gradually. This might include light resistance bands or putty exercises.
- Return to Activity:
- Light Activities: Children can typically return to light activities and school once pins are removed and a good functional ROM is achieved (usually 6-8 weeks post-op).
- Sports: Return to contact sports or activities involving repetitive overhead motions (e.g., throwing) is generally permitted around 8-12 weeks post-surgery, or when the fracture is fully consolidated, and full, pain-free ROM and strength are regained.
- Expected Outcomes: Most children regain excellent functional outcomes following open reduction, although a minor loss of terminal extension (5-10 degrees) is common but usually not functionally limiting. Close monitoring for complications like cubitus varus or persistent stiffness is essential during this period.
Summary of Key Literature and Guidelines
The management of supracondylar humerus fractures has evolved significantly over the past century, with a clear paradigm shift from open reduction to closed reduction and percutaneous pinning (CRPP) as the preferred treatment for displaced fractures. However, open reduction remains an indispensable technique for specific challenging scenarios.
Evolution of Management
Historically, supracondylar fractures were primarily managed with closed reduction and casting, often leading to unacceptably high rates of malunion (cubitus varus) and neurovascular compromise. The early 20th century saw the introduction of open reduction, which improved anatomical alignment but carried higher risks of infection and stiffness. The mid-to-late 20th century marked the widespread adoption of CRPP, championed for its ability to achieve anatomical reduction and stable fixation with minimal soft tissue disruption, thus reducing operative morbidity. This evolution cemented CRPP as the gold standard for most displaced Gartland type II, III, and IV fractures.
Current Evidence-Based Recommendations
Current guidelines strongly advocate for CRPP for reducible displaced supracondylar fractures. Open reduction is strictly reserved for a select subset of complex cases. Key literature supports the following principles:
- Irreducibility: Numerous studies highlight irreducibility as the most common indication for open reduction. Soft tissue interposition, particularly the brachialis muscle or periosteum, is a frequently cited cause. Open reduction in these cases allows for direct visualization and removal of impediments, leading to successful reduction and fixation.
- Vascular Compromise: The management of "pulseless pink" versus "pulseless pale" limbs is critical. While a "pulseless pink" hand after a stable reduction may often be observed, a "pulseless pale" hand, or any signs of ischemia not improving with reduction, warrants immediate open exploration of the brachial artery. Early literature often advocated for open reduction and exploration for all pulseless injuries, but more recent data suggests careful observation for a truly "pulseless pink" hand that reperfuses and maintains good perfusion after a successful closed reduction. However, a low threshold for exploration in any equivocal case is maintained.
- Open Fractures: Open supracondylar fractures are rare but mandate thorough debridement, often requiring open reduction, to minimize infection risk.
- Outcomes of Open Reduction: While generally effective in achieving reduction, open reduction has been associated with a slightly higher incidence of complications compared to CRPP, including increased rates of infection, stiffness, and occasionally cubitus varus. However, in carefully selected cases where closed methods fail, open reduction offers excellent outcomes.
- Surgical Approach: The anterior (Henry) approach is widely recognized as the safest and most effective for most irreducible extension-type fractures, offering direct access to the neurovascular bundle and fracture site. Medial and lateral approaches are reserved for specific fracture patterns or associated injuries.
- Fixation: Percutaneous K-wire fixation remains the preferred method, even after open reduction. The debate between cross-pinning (medial and lateral) and lateral-entry pinning continues, with proponents of cross-pinning citing superior biomechanical stability and proponents of lateral pinning emphasizing reduced risk of iatrogenic ulnar nerve injury. Meticulous technique, regardless of the method, is paramount.
Future Directions
Advances in fluoroscopic imaging, including 3D fluoroscopy, may offer enhanced intraoperative visualization and potentially reduce the need for formal open reduction in some borderline cases. The development of more minimally invasive techniques that combine arthroscopic assistance or smaller incisions with fluoroscopic guidance could further refine the approach for complex soft tissue interposition. Research into optimal rehabilitation strategies to mitigate stiffness while preventing complications like myositis ossificans is ongoing.
Concluding Remarks
Open reduction for supracondylar fractures of the humerus, though less frequently performed than CRPP, remains a vital procedure in the armamentarium of the pediatric orthopedic surgeon. It addresses specific and critical indications such as irreducibility, vascular compromise, and open fractures, where the alternative of failed closed management carries far greater morbidity. A deep understanding of the surgical anatomy, meticulous surgical technique, and vigilant post-operative care are essential to achieve optimal functional outcomes and prevent long-term complications in these challenging cases.
Clinical & Radiographic Imaging

You Might Also Like


