Mastering Pinning of Supracondylar Fractures: A Surgical Guide
Key Takeaway
This article provides essential research regarding Mastering Pinning of Supracondylar Fractures: A Surgical Guide. Percutaneous **pinning of supracondylar** fractures of the humerus is a common treatment for these elbow injuries in children, typically aged 5-7. Following closed reduction, pins are inserted to fixate the fracture, which often results from a fall. This procedure stabilizes the distal humerus, addressing what are predominantly extension-type fractures.
Introduction and Epidemiology
Definition and Incidence
Supracondylar fractures of the humerus represent a significant proportion of pediatric orthopedic trauma, accounting for up to 67% of children hospitalized with elbow injuries and comprising 3% to 17% of all childhood fractures. The annual incidence is estimated at 177.3 per 100,000 children, with a distinct peak in occurrence between the ages of 5 and 7 years. During this developmental window, the structural anatomy of the distal humerus undergoes dynamic changes, rendering the supracondylar region particularly susceptible to mechanical failure under axial and bending loads.

Mechanism of Injury and Pathogenesis
The mechanism of injury is predominantly indirect trauma, most commonly a fall from a height onto an outstretched hand (FOOSH) with the elbow locked in full extension. This mechanism accounts for the extension-type supracondylar fracture, which constitutes approximately 98% of all cases. Flexion-type injuries, resulting from direct trauma to the posterior aspect of a flexed elbow, account for the remaining 2%.
During a fall with the elbow in full extension, the olecranon process engages tightly within the olecranon fossa, acting as a rigid fulcrum. The anterior joint capsule, inserting distal to the olecranon fossa and proximal to the physis, transmits substantial tensile forces to the anterior cortex. Concurrently, the anatomic narrowing of the distal humerus at the supracondylar region creates a stress riser. The combination of ligamentous laxity—often resulting in physiologic hyperextension of the pediatric elbow—and these concentrated bending forces leads to a consistent pattern of structural failure.

Open injuries are rare, occurring in approximately 1% of cases, typically secondary to the proximal metaphyseal fragment piercing the anterior brachialis muscle and overlying skin. Concurrent ipsilateral fractures, such as those involving the distal radius, scaphoid, or proximal humerus, are present in roughly 1% of patients and must be systematically ruled out during the secondary survey.
Surgical Anatomy and Biomechanics
Osteology and Periosteal Hinges
Understanding the periosteal hinge is paramount for achieving and maintaining a successful closed reduction. In extension-type fractures, the anterior periosteum fails first, while the posterior periosteum frequently remains intact, serving as a critical tension band during reduction maneuvers.
The integrity of the medial and lateral periosteal sleeves dictates the required rotational reduction maneuvers. With posteromedial displacement, the lateral periosteum tears while the medial periosteal hinge remains intact. Consequently, forearm pronation tension the intact medial hinge, thereby closing the fracture gap and stabilizing the reduction. Conversely, with posterolateral displacement, the medial periosteum fails while the lateral hinge remains intact; forearm supination is therefore required to tension the lateral periosteum and lock the fracture fragments.

FIG 1 Reduction of a posteromedially displaced supracondylar fracture of the humerus. Pronation of the forearm closes the hinge and aids in reduction.
Neurovascular Anatomy at Risk
The direction of fracture displacement directly correlates with specific neurovascular structures at risk, primarily due to the trajectory of the sharp proximal metaphyseal fragment. Associated neurovascular injuries are significant, with nerve palsies occurring in approximately 11% of cases and vascular insufficiency or compromise present in up to 20% of severe displacements.

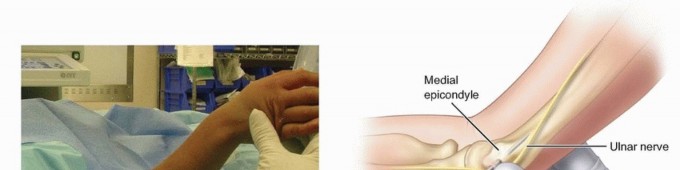
FIG 2 Cross-sectional representation of neurovascular structures at risk based on displacement vectors.
Medial displacement of the distal fragment (which means the proximal fragment translates laterally) places the radial nerve at significant risk as it pierces the lateral intermuscular septum. Lateral displacement of the distal fragment (proximal fragment translates medially) endangers the median nerve and the brachial artery. The anterior interosseous nerve (AIN), a branch of the median nerve, is the most frequently injured nerve in extension-type fractures. AIN function must be assessed preoperatively by evaluating the patient's ability to flex the interphalangeal joint of the thumb and the distal interphalangeal joint of the index finger (the "A-OK" sign).

The ulnar nerve courses through the cubital tunnel posterior to the medial epicondyle. It is highly susceptible to iatrogenic injury during the placement of medial pins, particularly if the elbow is hyperflexed. Flexion of the elbow causes the ulnar nerve to subluxate anteriorly in a significant percentage of the pediatric population. Therefore, if a medial pin is deemed biomechanically necessary, the elbow must be extended to at least 90 degrees (or relatively extended) to allow the nerve to fall posteriorly away from the medial epicondyle.
Biomechanical Considerations in Pediatric Elbows
The physis of the distal humerus contributes minimally to the longitudinal growth of the humerus, accounting for only 20% of overall humeral length. Because of this limited growth potential, the remodeling capacity for angular deformities—particularly in the coronal plane (cubitus varus)—is exceptionally poor. Sagittal plane deformities (extension/flexion) have slightly better remodeling potential in very young children, but near-anatomic reduction remains the absolute surgical objective to prevent long-term functional and cosmetic deficits.

Indications and Contraindications
Operative vs Non Operative Management
The management of supracondylar fractures is dictated by the degree of displacement, the presence of neurovascular compromise, and the stability of the fracture pattern. The modified Gartland classification system remains the standard framework for guiding treatment decisions.
| Treatment Modality | Indications | Contraindications |
|---|---|---|
| Non-Operative (Cast/Splint) | Gartland Type I (nondisplaced). Select Gartland Type II with minimal swelling, intact anterior humeral line, and no medial comminution. |
Displaced fractures (Type III/IV). Neurovascular compromise. Significant soft tissue swelling precluding safe casting. |
| Closed Reduction Percutaneous Pinning (CRPP) | Gartland Type II with extension deformity (anterior humeral line misses capitellum). Gartland Type III (completely displaced). Gartland Type IV (multidirectional instability). |
Irreducible fractures. Open fractures requiring debridement. Vascular injury requiring exploration (white, pulseless hand). |
| Open Reduction Internal Fixation (ORIF) | Irreducible by closed means (e.g., brachialis interposition). Open fractures. Dysvascular limb failing to perfuse after closed reduction. Severe multi-trauma requiring rigid fixation. |
Medically unstable patient. Undisplaced fractures. Severe overlying skin compromise (relative). |

The Gartland Classification System
The Gartland classification categorizes extension-type fractures into three primary types, with a fourth added by Leitch et al.
* Type I: Nondisplaced or minimally displaced (<2 mm). The anterior humeral line intersects the middle third of the capitellum.
* Type II: Displaced with an intact posterior cortex (hinge). The anterior humeral line passes anterior to the capitellum.
* Type III: Completely displaced with no cortical contact. Subclassified into posteromedial or posterolateral displacement.
* Type IV: Multidirectionally unstable fractures due to circumferential periosteal disruption. Diagnosed intraoperatively when the fracture demonstrates instability in both flexion and extension.
Pre Operative Planning and Patient Positioning
Clinical Evaluation and Imaging
A meticulous preoperative clinical evaluation is mandatory. The anterior cubital fossa must be inspected for the "pucker sign," a dimpling of the skin indicating that the proximal metaphyseal fragment has penetrated the brachialis muscle and subcutaneous tissues. This sign often heralds a difficult closed reduction and a higher likelihood of requiring an open approach.

Vascular assessment is critical. The limb must be categorized as well-perfused (warm, pink, palpable radial pulse), pink and pulseless (warm, capillary refill < 2 seconds, Dopplerable pulse), or white and pulseless (cold, delayed capillary refill, absent Doppler signals). A white, pulseless hand is an orthopedic emergency requiring immediate reduction and possible vascular exploration.
Standard imaging includes true anteroposterior (AP) and lateral radiographs of the elbow. In cases of severe trauma, imaging of the ipsilateral forearm and wrist is required to rule out concomitant injuries. On the lateral radiograph, the anterior humeral line and the teardrop angle should be assessed. On the AP radiograph, Baumann's angle (normal range 70 to 75 degrees) must be evaluated to assess coronal plane alignment and prevent cubitus varus.
Operating Room Setup and Positioning
The patient is positioned supine on the operating table. General anesthesia is required to ensure complete muscle relaxation, which is essential for a traumatic closed reduction. The C-arm fluoroscope is typically brought in perpendicular to the operating table.
Two primary setups are utilized: the arm board technique and the C-arm as table technique. Using the C-arm image intensifier as the operative table allows for excellent visualization and easy transition between AP and lateral imaging by rotating the C-arm 90 degrees, thereby minimizing movement of the unstable fracture. The shoulder is abducted to 90 degrees, and the elbow is positioned over the center of the image intensifier.

Detailed Surgical Approach and Technique
Closed Reduction Maneuvers
The goal of closed reduction is to restore anatomic alignment with minimal trauma to the surrounding soft tissues and neurovascular structures. The reduction sequence must systematically address the three dimensions of displacement: length, translation/rotation, and angulation.
- Traction: With the elbow in slight flexion (20 to 30 degrees) and the forearm in supination, longitudinal traction is applied to disengage the fracture fragments and restore length. Counter-traction is applied by an assistant holding the proximal humerus.
- Coronal Plane Correction: While maintaining traction, medial or lateral translation and varus/valgus angulation are corrected. The carrying angle must be restored to match the contralateral limb.
- Sagittal Plane Correction: The surgeon places their thumb on the posterior aspect of the olecranon and their fingers over the anterior aspect of the proximal humeral fragment. The elbow is then smoothly hyperflexed while anterior pressure is applied to the olecranon to correct the extension deformity.
- Rotational Lock: Depending on the fracture pattern, the forearm is pronated (for posteromedial displacement) or supinated (for posterolateral displacement) to tension the intact periosteal hinge and lock the reduction.

The reduction is immediately assessed under fluoroscopy. An AP view is obtained by externally rotating the shoulder (Jones view), and a lateral view is obtained by internally rotating the shoulder. The elbow joint itself should not be rotated, as this can destabilize the reduction.
Percutaneous Pinning Configurations
Once an anatomic reduction is confirmed, percutaneous pinning is performed using smooth Kirschner wires (typically 1.6 mm or 2.0 mm, depending on patient size). The standard of care emphasizes the use of lateral-entry pins to avoid iatrogenic injury to the ulnar nerve.
Lateral Pin Construct:
Two or three divergent lateral pins are placed. The starting point is the lateral epicondyle and the capitellum. The pins should be directed proximally and medially, engaging the medial cortex of the proximal fragment. Biomechanical stability is maximized by achieving maximum separation of the pins at the fracture site and ensuring that at least one pin crosses proximal to the olecranon fossa. If the two pins are too close together, the construct acts as a single axis of rotation, leading to instability. A third lateral pin can be added for highly unstable fractures or if the initial two pins do not achieve optimal spread.

Medial Pin Placement and Ulnar Nerve Protection
If intraoperative evaluation reveals persistent instability (particularly medial column comminution or Gartland Type IV multidirectional instability) despite optimal lateral pin placement, a crossed-pin construct may be necessary.
To safely place a medial pin, the ulnar nerve must be protected. The elbow is extended to approximately 45 to 60 degrees to allow the ulnar nerve to subluxate posteriorly into the cubital tunnel. A mini-open approach is mandatory. A small incision is made over the medial epicondyle, and blunt dissection is carried down to the bone using a hemostat. A tissue protector or drill sleeve is placed directly on the medial epicondyle to prevent the wire from wrapping the nerve. The medial pin is then driven proximally and laterally, crossing the lateral pins proximal to the fracture site to avoid creating a stress riser at the fracture level.

Management of the Pulseless Pink Hand
The management of a supracondylar fracture presenting with a pink but pulseless hand remains a topic of academic debate. The initial step is always an emergent closed reduction and percutaneous pinning. In the majority of cases, anatomic reduction relieves the kinking or spasm of the brachial artery, and the radial pulse returns.
If the hand remains pink and well-perfused (capillary refill < 2 seconds) but the pulse is absent following rigid fixation, current literature supports close observation. Collateral circulation around the elbow is robust, and aggressive vascular exploration in a well-perfused hand carries risks of iatrogenic injury and infection. However, the patient must be admitted for strict neurovascular monitoring. If perfusion deteriorates (the hand becomes white and cold), immediate vascular exploration is indicated.

Open Reduction Techniques
Open reduction is indicated for irreducible fractures, open fractures, or cases requiring vascular exploration. The anterior approach is standard for vascular exploration. A transverse incision is made in the antecubital crease, allowing access to the brachial artery and median nerve. The brachialis muscle is often found to be torn, with the proximal humeral spike protruding through it.
For fractures irreducible closed but without vascular compromise, a medial or lateral approach may be utilized depending on the direction of displacement and the location of the suspected soft tissue interposition. The lateral approach provides excellent access to the lateral column and capitellum, while the medial approach allows for direct visualization of the medial column and ulnar nerve.

Complications and Management
Neurologic and Vascular Complications
Neurologic injuries are common but are typically neuropraxias that resolve spontaneously within 3 to 6 months. The anterior interosseous nerve is most frequently injured in extension-type fractures, while the ulnar nerve is at risk in flexion-type fractures and during medial pin placement. Iatrogenic ulnar nerve injury requires immediate pin removal and repositioning if recognized intraoperatively. If recognized postoperatively, observation is generally recommended initially, as most are traction or compression neuropraxias rather than complete transections.
Vascular compromise can lead to Volkmann ischemic contracture, a devastating complication resulting from untreated compartment syndrome of the forearm. Signs of compartment syndrome (pain out of proportion, pain with passive stretch of the fingers) require emergent fasciotomy.

Malunion and Cubitus Varus
Cubitus varus (gunstock deformity) is the most common late complication, occurring due to malreduction in the coronal plane (failure to correct medial impaction) or internal rotation of the distal fragment. While primarily a cosmetic deformity with minimal functional impairment, severe cases can lead to tardy posterolateral rotatory instability (PLRI) or ulnar neuropathy. Treatment, if desired by the patient or family, involves a corrective lateral closing-wedge osteotomy or a dome osteotomy of the distal humerus.
| Complication | Incidence | Etiology and Management Strategy |
|---|---|---|
| Pin Tract Infection | 1% - 2% | Superficial infections managed with oral antibiotics. Deep infections require early pin removal and IV antibiotics. |
| Neuropraxia (AIN/Radial) | 10% - 15% | Typically occurs at the time of injury. Management is expectant observation; majority resolve in 3-6 months. |
| Iatrogenic Ulnar Nerve Injury | 2% - 4% | Associated with blind medial pin placement. Prevented by mini-open technique and elbow extension. Requires pin removal if symptomatic. |
| Cubitus Varus | 3% - 5% | Results from malreduction (decreased Baumann's angle). Cosmetic deformity. Salvage with corrective osteotomy if severe. |
| Compartment Syndrome | < 1% | High energy trauma, severe swelling. Requires emergent forearm fasciotomy and rigid fracture fixation. |

Post Operative Rehabilitation Protocols
Immobilization Phase
Following secure percutaneous pinning, the pins are bent and cut outside the skin to facilitate easy removal in the clinic. Sterile dressings are applied around the pin sites. The limb is immobilized in a long-arm posterior splint or a bivalved cast. The elbow should be immobilized in 70 to 90 degrees of flexion. Hyperflexion (greater than 90 degrees) must be strictly avoided in the immediate postoperative period, as it increases intra-articular and compartmental pressures, exacerbating the risk of vascular compromise and compartment syndrome. The forearm is placed in neutral rotation.
The patient is typically observed overnight for neurovascular checks and pain control. Discharge is appropriate when pain is well-controlled on oral medications and neurovascular status is stable.
Mobilization and Functional Recovery
The patient returns to the orthopedic clinic at 3 to 4 weeks postoperatively. Radiographs are obtained out of the splint to confirm the maintenance of reduction and the presence of early callus formation. At this stage, clinical healing is usually sufficient, and the percutaneous pins are removed in the clinic setting. No anesthesia is typically required for pin removal, though child life specialists and distraction techniques are highly beneficial.
Following pin removal, the patient is transitioned to a sling for comfort and encouraged to begin active range of motion exercises. Passive range of motion and aggressive physical therapy are contraindicated, as they can induce heterotopic ossification and paradoxically increase joint stiffness. Parents should be counseled that full extension is often the last motion to return and may take up to 6 months to fully normalize. Return to contact sports and high-impact activities is generally restricted for 8 to 12 weeks post-injury, pending radiographic union and full restoration of strength and motion.
Summary of Key Literature and Guidelines
Evidence Based Pinning Strategies
The debate between crossed-pin constructs and lateral-only pin constructs has been a focal point of orthopedic literature for decades. Seminal biomechanical studies demonstrated that crossed pins offer superior torsional stability compared to parallel lateral pins. However, clinical studies, notably those by Skaggs et al., have shown no significant difference in the maintenance of reduction or clinical outcomes between crossed pins and properly placed divergent lateral pins. The critical factor for lateral pins is maximizing the distance between the pins at the fracture site. Given the zero risk of iatrogenic ulnar nerve injury with a lateral-only construct, the American Academy of Orthopaedic Surgeons (AAOS) and the Pediatric Orthopaedic Society of North America (POSNA) strongly advocate for attempting a robust lateral pin construct as the initial fixation strategy.
AAOS Clinical Practice Guidelines
The AAOS Clinical Practice Guidelines for the Management of Pediatric Supracondylar Humerus Fractures provide several strong recommendations based on high-quality evidence. These include the recommendation against routine open reduction for completely displaced fractures that can be anatomically reduced closed. Furthermore, the guidelines support
Clinical & Radiographic Imaging
You Might Also Like

