Revision Total Knee Arthroplasty: A Comprehensive Surgical Guide
Key Takeaway
Revision total knee arthroplasty (TKA) addresses primary implant failure due to aseptic loosening, instability, polyethylene wear, or periprosthetic fracture. Successful revision demands meticulous preoperative planning, extensile surgical exposures like the rectus snip or tibial tubercle osteotomy, and precise component extraction to preserve bone stock. Implant selection relies on matching the degree of constraint to the patient's ligamentous incompetence, ensuring durable biomechanical stability and optimal functional recovery.
Epidemiology and Survivorship of Primary TKA
The rate of revision for primary total knee arthroplasty (TKA) remains relatively low, a testament to the biomechanical success and durability of modern implant designs. According to a comprehensive meta-analysis involving 9,879 patients by Callahan et al., a 3.8% revision rate was observed at four years following primary tricompartmental TKA. In a broader population-based study by Coyte et al., a similar revision rate, estimated between 4.3% and 8%, was documented at seven years postoperatively across a cohort of 18,530 patients. Longitudinal data extracted from the National Hospital Discharge Survey and the U.S. Census from 1990 to 2002 demonstrated a relatively constant 8.2% overall revision rate for TKA. However, as the absolute number of primary TKAs performed globally continues to rise exponentially, the corresponding burden of revision arthroplasty is increasing, necessitating advanced surgical proficiency among orthopedic surgeons.
Mechanisms of Failure in Total Knee Arthroplasty
Aseptic Loosening and Osteolysis
Aseptic failure of a TKA is a multifactorial process driven by component loosening, polyethylene wear with subsequent osteolysis, ligamentous laxity, periprosthetic fracture, arthrofibrosis, and patellofemoral complications. Historically and currently, tibial component loosening occurs more frequently than femoral component loosening.
Tibial subsidence and loosening are strongly associated with:
* Malalignment of the mechanical axis (particularly residual varus).
* Ligamentous laxity leading to eccentric loading.
* Duration of implantation and cumulative cyclic loading.
* High patient activity demands.
* Accelerated polyethylene wear generating particulate debris.
* Excessive component constraint transferring shear forces to the bone-implant interface.
Clinical Pearl: Polyethylene wear initiates a macrophage-induced inflammatory cascade, leading to aggressive periprosthetic osteolysis. While isolated modular polyethylene insert exchange may seem appealing for worn inserts, Babis, Trousdale, and Morrey warned that such limited revisions yield a 25% repeat revision rate at an average of only three years postoperatively. Isolated exchange is only viable if the baseplate is perfectly aligned, rigidly fixed, and devoid of undersurface wear.
Instability
Instability is an increasingly prevalent indication for revision TKA, accounting for approximately 20% of all revisions in longitudinal studies by Fehring and Valadie.
Fig. 6-74 Instability may be an indication for revision knee arthroplasty.
The primary etiologies of instability include:
1. Ligamentous Imbalance: Failure to balance the flexion and extension gaps during the index procedure.
2. Late Ligamentous Incompetence: Attenuation of the medial collateral ligament (MCL) or posterior cruciate ligament (PCL) over time.
3. Extensor Mechanism Deficiency: Patellar tendon rupture or severe patellofemoral maltracking.
4. Surgical Error: Improper bone cuts altering the joint line or component rotation.
Routine knee aspiration in unstable knees often reveals a preponderance of red blood cells (averaging 64,000/mm³), indicative of chronic synovial impingement and recurrent hemarthrosis.
Periprosthetic Fractures
Periprosthetic fractures demand a rigorous algorithmic approach based on component stability, fracture displacement, and host bone quality.

Fig. 6-69 A and B, LISS plate fixation of periprosthetic femoral fracture.
For supracondylar femoral fractures above a TKA, if the prosthesis remains stable, open reduction and internal fixation (ORIF) using locked plating (e.g., LISS plate) or intramedullary nailing is indicated. If the prosthesis is unstable, a stemmed revision TKA, often requiring distal femoral allografts or tumor mega-prostheses, is mandatory.
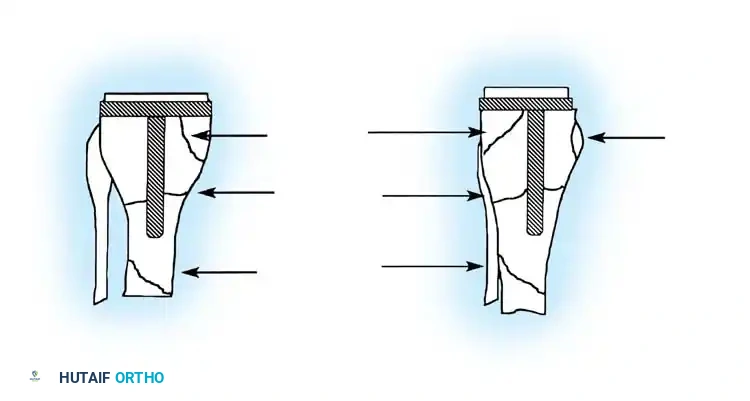
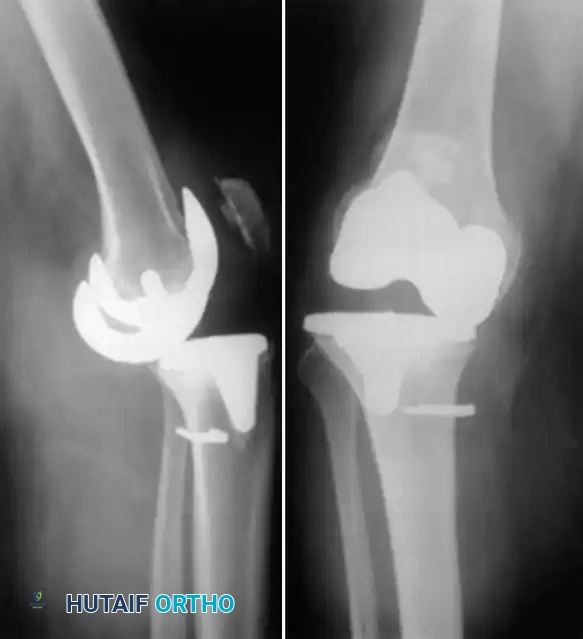
Fig. 6-71 Anatomical locations of tibial fractures associated with total knee arthroplasty.
Tibial periprosthetic fractures (Felix classification) are similarly managed based on the anatomical location of the fracture relative to the stem, the stability of the implant, and the timing of the fracture (intraoperative vs. postoperative).
Radiographic Evaluation of the Failed TKA
Meticulous radiographic analysis is the cornerstone of preoperative planning. Aseptic loosening of either component may manifest on standard radiographs as a complete radiolucent line of 2 mm or more at the bone-cement interface in cemented arthroplasties.

Fig. 6-72 Lucency at the entire bone-cement interface of the tibial component, with deformity and subsidence of the component.
Incomplete radiolucencies of less than 2 mm are common and do not necessarily correlate with poor clinical outcomes. However, radiolucent lines around uncemented implants indicate regions where osteointegration has failed. If these lines are extensive, progressive, or symptomatic, aseptic loosening is highly probable.

Fig. 6-73 Loose uncemented femoral component with subsidence into an extended position relative to the distal femur.
Surgical Warning: A radiolucent line under a metal-backed tibial component can be easily obscured by as little as 4 degrees of knee flexion. Fluoroscopic examination is highly recommended for patients with unexplained pain and seemingly "normal" static radiographs. Fluoroscopy allows the x-ray beam to be positioned perfectly parallel to the implant surfaces, unmasking subtle radiolucencies.
Surgical Exposures in Revision Arthroplasty
Exposure in revision TKA is notoriously challenging due to altered anatomy, arthrofibrosis, and compromised soft-tissue envelopes.
Incision Planning and Standard Arthrotomy
The surgeon should utilize the previous TKA skin incision whenever possible. Parallel longitudinal anterior knee incisions place the intervening skin bridge at severe risk for ischemic necrosis. If multiple previous incisions exist, the most lateral viable incision should be selected, as the superficial blood supply to the anterior knee predominantly arises from the medial side.
A standard medial parapatellar arthrotomy is the workhorse approach. However, the scarred capsule must often be thinned. Re-creation of the medial and lateral gutters, subperiosteal release of the medial soft tissues from the proximal tibia, and lateral retinacular release are frequently required to allow patellar eversion without avulsing the patellar tendon.
Extensile Exposures
If the medial fibers of the patellar tendon insertion begin to peel away from the tibial tubercle during flexion, tension must be immediately released, and an extensile approach must be employed.
The Quadriceps Turndown (V-Y Plasty)
Originally described by Coonse and Adams and modified by Scott and Siliski, this involves a standard medial parapatellar incision with an additional limb extending as an inverted "V" across the quadriceps tendon through the lateral retinaculum.
During closure, the inverted "V" is converted to a "Y" by advancing the patella distally, which is highly effective for knees with severe quadriceps contractures. Postoperatively, patients require a hinged knee brace locked in extension for 2 to 3 months, with a gradual return to active extension to prevent extensor lag.
The Rectus Snip
Described by Insall, the rectus snip is a highly versatile modification. The proximal extent of the medial parapatellar arthrotomy is extended laterally across the quadriceps tendon, incising the rectus femoris tendon and the underlying vastus intermedius.
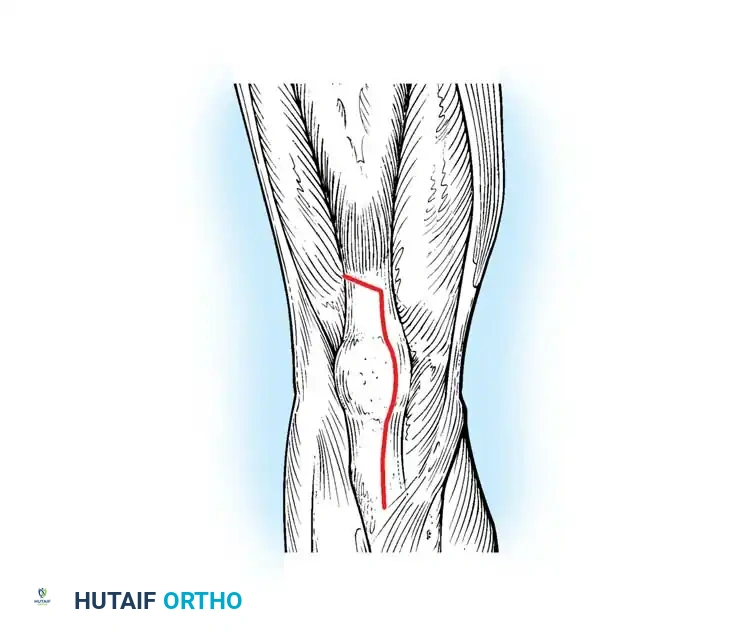
Fig. 6-76 Insall rectus snip modification of the quadriceps turndown procedure.
The lateral attachment of the vastus lateralis and the superior lateral geniculate vessels are preserved. Unlike the V-Y turndown, the rectus snip does not require altering the postoperative rehabilitation protocol, and outcomes are comparable to a standard arthrotomy.
Tibial Tubercle Osteotomy (TTO)
Modified by Whiteside and Ohl, the TTO provides unparalleled exposure of the diaphysis and joint space while relaxing the extensor mechanism.
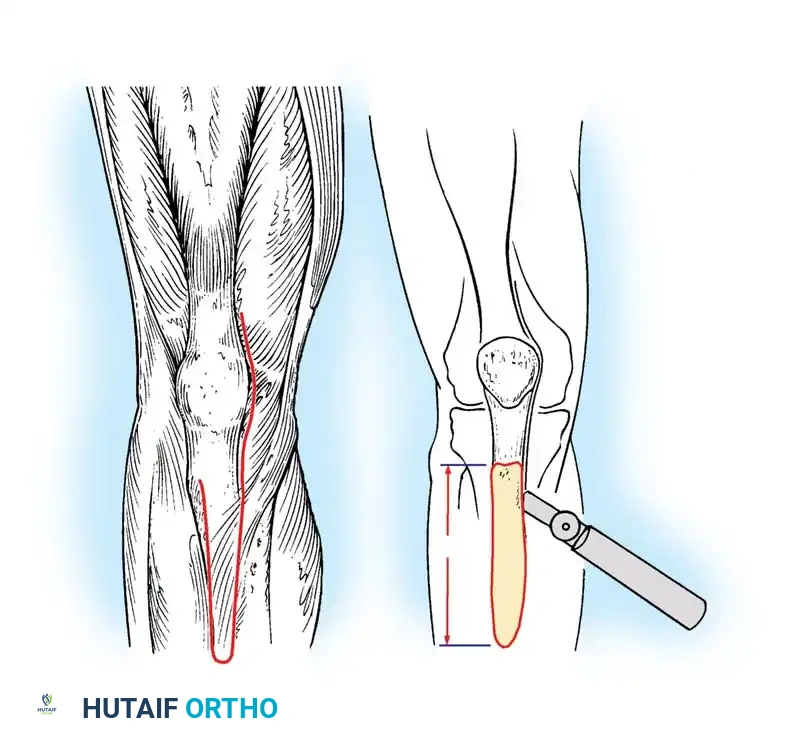
Fig. 6-77 Tibial tubercle osteotomy to relax quadriceps and improve exposure. An 8- to 10-cm segment is elevated.
An 8- to 10-cm segment of bone including the tubercle and anterior tibial crest is elevated from medial to lateral, leaving the anterior compartment musculature attached laterally to preserve vascularity.

Fig. 6-78 Proximal advancement of tibial tubercle osteotomy for the treatment of patella baja.
The tubercle can be advanced proximally to correct patella baja or joint line elevation. Fixation is achieved with cerclage wires or bicortical screws. Complications include nonunion, proximal migration, and prominent hardware.
The Femoral Peel
For severe bony or fibrous ankylosis, Windsor and Insall described the femoral peel.
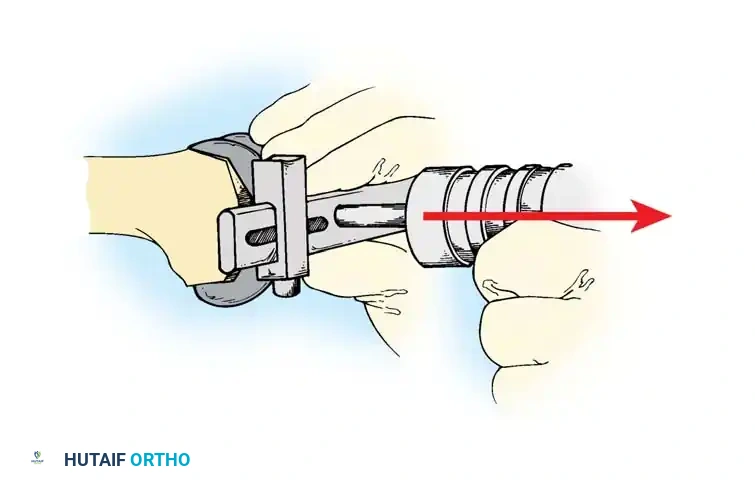
Fig. 6-79 The Femoral Peel technique for severe ankylosis.
The soft tissues around the distal femur are subperiosteally dissected away, including the origins of the collateral ligaments, allowing the femur to be skeletonized and delivered into the wound.
Component Extraction Techniques
The overarching goal of component removal is the absolute preservation of host bone stock. Brute force must be avoided.
Removing the Tibial Component
With all-polyethylene tibial components, the interface can be disrupted using an oscillating saw to cut directly through the polyethylene stem, allowing access to the bone-cement interface.
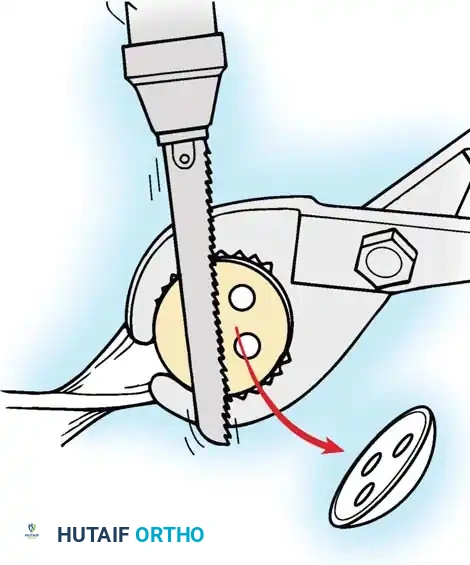
Fig. 6-80A Disruption of the polyethylene interface using an oscillating saw.
For metal-backed tibial components, freeing the undersurface of the baseplate with thin osteotomes or a Gigli saw usually allows extraction.
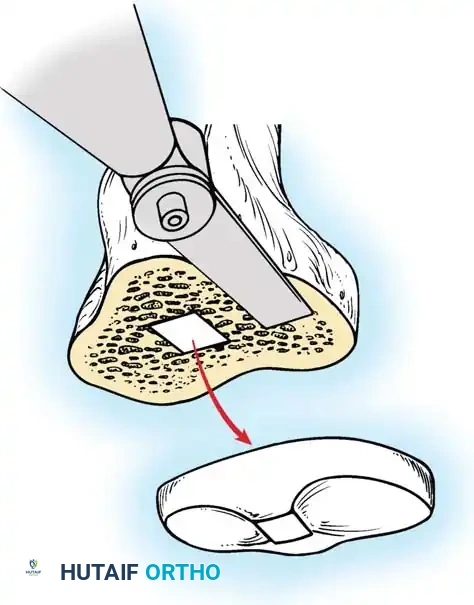
Fig. 6-80B Accessing the bone-cement interface of a metal-backed component.
If the stem is long, fully cemented, or features a porous ingrowth surface, a long tibial tubercle osteotomy may be required to safely disimpact the keel without fracturing the proximal tibia.
Fig. 6-81 Use of thin, flexible osteotomes to disrupt the bone-implant interface.
Removing the Femoral Component
The femoral component is addressed by systematically disrupting the cement mantle or ingrowth surface at the anterior flange, distal condyles, and posterior chamfers using thin, flexible osteotomes.

Fig. 6-82 Systematic disruption of the femoral bone-cement interface.
Once the interfaces are free, a slap hammer or extraction device is applied to the intercondylar notch or modular lugs to gently back the implant off the bone in the axis of its original insertion.

Fig. 6-83 Application of a slap hammer for controlled axial extraction of the femoral component.
Implant Selection, Constraint, and Bone Loss Management
Implant selection in revision TKA is dictated by the degree of ligamentous incompetence and the magnitude of bone loss. The surgeon must adhere to the principle of using the lowest level of constraint necessary to achieve stability, as increased constraint transfers higher stresses to the implant-bone interface, increasing the risk of premature aseptic loosening.

Fig. 6-84 Modular revision TKA systems offering variable constraint, stems, and augments.
Managing Instability Biomechanics
- Anteroposterior (Flexion Space) Instability: Treated by conversion to a Posterior-Stabilized (PS) implant. Cruciate-retaining (CR) inserts are rarely appropriate in the revision setting unless the PCL is pristine and the flexion gap is perfectly balanced.
- Varus-Valgus (Extension Space) Instability: If soft-tissue balancing is achievable, a Constrained Condylar Knee (CCK) design is utilized. CCK implants feature a tall, wide central post that engages the femoral cam closely, resisting coronal plane moments.
- Global or Multiplanar Instability: If the collateral ligaments are entirely deficient or cannot be reconstructed, a linked (rotating hinge) implant is mandatory.
Managing Metaphyseal and Diaphyseal Bone Loss
Bone loss is classified using systems such as the Anderson Orthopaedic Research Institute (AORI) classification.
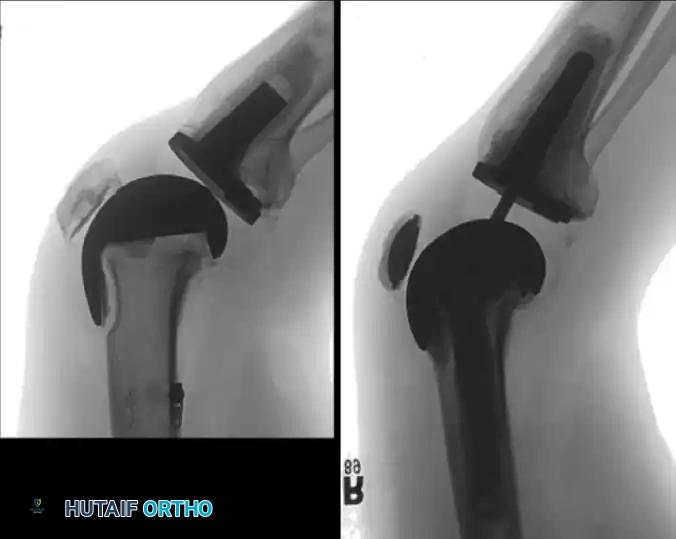
Fig. 6-85 Assessment of uncontained metaphyseal bone defects.
- Type I (Intact Metaphysis): Managed with standard revision components and particulate bone graft.
- Type II (Damaged Metaphysis): Requires modular metallic augments (blocks or wedges) to restore the joint line.

Fig. 6-86 Application of modular metallic augments to address Type II bone defects.
- Type III (Deficient Metaphysis): Severe cavitary or uncontained defects require highly porous metaphyseal cones, sleeves, or structural allografts to achieve zonal fixation.

Fig. 6-87 Use of highly porous metaphyseal cones and diaphyseal stems for Type III defects.
Diaphyseal engaging stems (cemented or press-fit) are critical in revision TKA to bypass deficient metaphyseal bone and transfer loads directly to the cortical diaphysis, adhering to the principles of joint line restoration and rigid mechanical alignment.
Postoperative Protocol
Rehabilitation following revision TKA is highly individualized. If a standard arthrotomy or rectus snip was utilized, immediate weight-bearing as tolerated and early active range of motion are encouraged. However, if a tibial tubercle osteotomy or V-Y quadriceps turndown was performed, the extensor mechanism must be protected. These patients are typically restricted to a hinged knee brace locked in extension during ambulation for 6 weeks, with strictly controlled passive flexion parameters to prevent catastrophic extensor mechanism failure.
📚 Medical References
- Revision total knee arthroplasty for failed unicompartmental replacement, J Bone Joint Surg 73A:186, 1991.
- Pagnano MW, Cushner FD, Scott N: Role of the posterior cruciate ligament in total knee arthroplasty, J Am Acad Orthop Surg 6:176, 1998.
- Pagnano MW, Levy BA, Berry DJ: Cemented all polyethylene tibial components in patients age 75 years and older, Clin Orthop Relat Res 367:73, 1999.
- Pagnano MW, Trousdale RT, Stuart MJ, et al: Rotating platform knees did not improve patellar tracking: a prospective, randomized study of 240 primary total knee arthroplasties, Clin Orthop Relat Res 428:221, 2004.
- Pereira DS, Jaffe FF, Ortiguera C: Posterior cruciate ligamentsparing versus posterior cruciate ligament-sacrifi cing arthroplasty: functional results using the same prosthesis, J Arthroplasty 13:138, 1998.
- Pettine KA, Wedel DJ, Cabanela ME, Weeks JL: The use of epidural bupivicaine following total knee arthroplasty, Orthop Rev 18:894, 1989.
- Pomeroy DL, Schaper LA, Badenhausen WE, et al: Results of all-polyethylene tibial components as a cost-saving technique, Clin Orthop Relat Res 380:140, 2000.
- Puloski SK, McCalden RW, MacDonald SJ, et al: Tibial post wear in posterior stabilized total knee arthroplasty: an unrecognized source of polyethylene debris, J Bone Joint Surg 83A:390, 2001.
- Ranawat AS, Rossi R, Loreti I, et al: Comparison of the PFC Sigma fi xed-bearing and rotating-platform total knee arthroplasty in the same patient: short-term results, J Arthroplasty 19:35, 2004.
- Ranawat CS: The patellofemoral joint in total condylar knee arthroplasty: pros and cons based on 5to 10-year follow-up observations, Clin Orthop Relat Res 205:93, 1986.
- Ranawat CS, Johanson NA, Rimnac CM, et al: Retrieval analysis of porous-coated components for total knee arthroplasty, Clin Orthop Relat Res 209:244, 1986.
- Rand JA: Patellar resurfacing in total knee arthroplasty, Clin Orthop Relat Res 260:110, 1990.
- Rand JA: Comparison of metal-backed and all-polyethylene tibial components in cruciate condylar total knee arthroplasty, J Arthroplasty 8:307, 1993.
- Rand JA, Chao EY, Stauffer RN: Kinematic rotating-hinge total knee arthroplasty, J Bone Joint Surg 69A:489, 1987.
- Rand JA, Ilstrup DM: Survival analysis of total knee arthroplasty, J Bone Joint Surg 73A:397, 1991.
- Reilly D, Walker PS, Ben-Dov M, et al: Effects of tibial components on load transfer in the upper tibia, Clin Orthop Relat Res 165:2373, 1982.
- Reis MD, Salehi A, Laskin RS, et al: Can rotational congruity be achieved in both fl exion and extension when the femoral component is externally rotated in total knee arthroplasty? Knee 5:37, 1998.
- Rose RM, Crugnola A, Ries M, et al: On origins of high in vivo wear rates in polyethylene components of total joint prostheses, Clin Orthop Relat Res 145:277, 1979.
- Rosenberg AG, Verner JJ, Galante JO: Clinical results of total knee revision using the total condylar III prosthesis, Clin Orthop Relat Res 273:83, 1991.
- Sands KC, Silver JW: Fracture of the polyethylene tibial post in a posterior stabilized PFC total knee arthroplasty, Orthopedics 28:1203, 2005.
- Scott RD: Primary knee arthroplasty: long-term outcomes and expectations—cruciate-sparing total knee arthroplasty, Orthopedics 17:839, 1994.
- Scott RD, Cobb AG, McQueary FG, et al: Unicompartmental knee arthroplasty: 8to 12-year follow-up with survivorship analysis, Clin Orthop Relat Res 271:96, 1991.
- Scott RD, Thornhill TS: Posterior cruciate supplementing total knee replacement using conforming inserts and cruciate recession: effect on range of motion and radiolucent lines, Clin Orthop Relat Res 309:146, 1994.
- Scott RD, Volatile TB: Twelve years’ experience with posterior cruciate–retaining total knee arthroplasty, Clin Orthop Relat Res 205:100, 1986.
- Scuderi GR, Insall JN, Windsor RE, et al: Survivorship of cemented knee replacements, J Bone Joint Surg 71B:798, 1989.
- Scuderi GR, Komistek RD, Dennis DA, et al: The impact of femoral component rotational alignment on condylar lift-off, Clin Orthop Relat Res 410:148, 2003.
- Sharrock NE, Go G, Williams-Russo P, et al: Comparison of extradural and general anesthesia on the fi brinolytic response to total knee arthroplasty, Br J Anaesth 80:126, 1998.
- Shiers LGP: Hinge arthroplasty of the knee, J Bone Joint Surg 47B:586, 1965.
- Shoji H, Wolf A, Packard S, et al: Cruciate retained and excised total knee arthroplasty: a comparative study in patients with bilateral total knee arthroplasty, Clin Orthop Relat Res 305:218, 1994.
- Smith-Peterson MN: Arthroplasty of the hip: a new method, J Bone Joint Surg 31:269, 1939.
- Stiehl JB, Komistek RD, Dennis DA, et al: Fluoroscopic analysis of kinematics after posterior-cruciate-retaining knee arthroplasty, J Bone Joint Surg 77B:884, 1995.
- Sumner DR, Turner TM, Dawson D, et al: Effect of pegs and screws on bone ingrowth in cementless total knee arthroplasty, Clin Orthop Relat Res 309:150, 1994.
- Surace MF, Berzins A, Urban RM, et al: Coventry Award paper. Backsurface wear and deformation in polyethylene tibial inserts retrieved postmortem, Clin Orthop Relat Res 404:14, 2002.
- Swanson SA, Freeman MA: A new prosthesis for the total replacement of the knee, Acta Orthop 38(S1):55, 1972.
- Tew M, Waugh W: Tibiofemoral alignment and the results of knee replacement, J Bone Joint Surg 67B:551, 1985.
- Thompson NW, Wilson DS, Cran GW, et al: Dislocation of the rotating platform after low contact stress total knee arthroplasty, Clin Orthop Relat Res 425:207, 2004.
- Tsao S, Mintz L, McRae CR, et al: Failure of the porous-coated anatomic prosthesis in total knee arthroplasty due to severe polyethylene wear, J Bone Joint Surg 75A:19, 1993.
- Verneil A: Resultats obtain for France par l’operation d’esmarch: examen des causes d’insuccess et moyen d’y remedier, Gas Hebd Med Chir 10:97, 1863.
- Victor J, Banks S, Bellemans J: Kinematics of posterior cruciate ligament-retaining and -substituting total knee arthroplasty: a prospective randomised outcome study, J Bone Joint Surg 87B:646, 2005.
- Vince KG: Principles of condylar knee arthroplasty: issues evolving, Instr Course Lect 42:315, 1993.
- Vince KG, McPherson EJ: The patella in total knee arthroplasty, Orthop Clin North Am 23:675, 1992.
- Walker PS, Greene D, Reilly D, et al: Fixation of tibial components of knee prosthesis, J Bone Joint Surg 63A:258, 1981.
- Walldius B: Arthroplasty of the knee joint using endoprosthesis, Acta Orthop Scand 24(suppl):19, 1957.
- Wasielewski RC: The causes of insert backside wear in total knee arthroplasty, Clin Orthop Relat Res 404:232, 2002.
- Wasielewski RC, Galante JO, Leighty RM, et al: Wear patterns on retrieved polyethylene tibial inserts and their relationship to technical considerations during total knee arthroplasty, Clin Orthop Relat Res 299:31, 1994.
- Waters TS, Bentley G: Patellar resurfacing in total knee arthroplasty: a prospective, randomized study, J Bone Joint Surg 85A:212, 2003.
- Weir DJ, Moran CG, Pinder IM: Kinematic condylar total knee arthroplasty: 14-year survivorship analysis of 208 consecutive cases. J Bone Joint Surg 78B:907, 1996.
- Westrich GH, Haas SB, Insall JN, et al: Resection specimen analysis of proximal tibial anatomy based on 100 total knee arthroplasty specimens, J Arthroplasty 10:47, 1995.
- Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty, Clin Orthop Relat Res 321:168, 1995.
- Whiteside LA, Nakamura T: Effect of femoral component design on unresurfaced patellas in knee arthroplasty, Clin Orthop Relat Res 410:189, 2003.
- Wilson SA, McCann PD, Gotlin RS, et al: Comprehensive gait analysis in posterior-stabilized knee arthroplasty, J Arthroplasty 11:359, 1996.
- Windsor RE, Scuderi GR, Moran MC, et al: Mechanisms of failure of the femoral and tibial components in total knee arthroplasty, Clin Orthop Relat Res 248:15, 1989.
- Wood DJ, Smith AJ, Collopy D, et al: Patellar resurfacing in total knee arthroplasty: a prospective, randomized trial, J Bone Joint Surg 84A:187, 2002.
- Wright TM, Rimnac CM, Stulberg SD, et al: Wear of polyethylene in total joint replacements: observations from retrieved PCA knee implants, Clin Orthop Relat Res 276:126, 1992.
- Indications and Contraindications Abraham W, Buchanan JR, Daubert H, et al: Should the patella be resurfaced in total knee arthroplasty? Effi cacy of patellar resurfacing, Clin Orthop Relat Res 236:128, 1988.
- Adam RF, Noble J: Primary total knee arthroplasty in the elderly, J Arthroplasty 9:495, 1994.
- Barrack RL, Wolfe MW, Waldman DA, et al: Resurfacing of the patella in total knee arthroplasty, J Bone Joint Surg 79A:1121, 1997.
- Barrett WP, Scott RD: Revision of failed unicondylar unicompartmental knee arthroplasty, J Bone Joint Surg 69A:1328, 1987.
- Bould M, Freeman BJ, Pullyblank A, et al: Blood loss in sequential bilateral total knee arthroplasty, J Arthroplasty 13:77, 1998.
- Boyd AD, Ewald FC, Thomas WH, et al: Long-term complications after total knee arthroplasty with or without resurfacing of the patella, J Bone Joint Surg 75A:674, 1993.
- Cartier P, Sanouiller J-L, Grelsamer RP: Unicompartmental knee arthroplasty surgery: 10-year minimum follow-up period, J Arthroplasty 11:782, 1996.
- Cohen RG, Forrest CJ, Benjamin JB: Safety and effi cacy of bilateral total knee arthroplasty, J Arthroplasty 12:497, 1997.
- Dorr LD, Merkel C, Mellman MF, et al: Fat emboli in bilateral total knee arthroplasty: predictive factors for neurologic manifestations, Clin Orthop Relat Res 248:112, 1989.
- Duffy GP, Trousdale RT, Stuart MJ: Total knee arthroplasty in patients 55 years old or younger, 10to 17-year results, Clin Orthop Relat Res 356:22, 1998.
- Easley ME, Insall JN, Scuderi GR, et al: Primary constrained condylar knee arthroplasty for the arthritic valgus knee, Clin Orthop Relat Res 380:58, 2000.
- Enis JE, Gardner R, Robledo MA, et al: Comparison of patellar resurfacing versus nonresurfacing in bilateral knee arthroplasty, Clin Orthop Relat Res 260:38, 1990.
- Gill T, Schemitsch EH, Brick GW, Thornhill TS: Revision total knee arthroplasty after failed unicompartmental knee arthroplasty or high tibial osteotomy, Clin Orthop Relat Res 321:10, 1995.
- Healy WL, Finn D: The hospital cost and the cost of the implant for total knee arthroplasty: a comparison between 1983 and 1991 for one hospital, J Bone Joint Surg 76A:801, 1994.
- Hosick WB, Lotke PA, Baldwin A: Total knee arthroplasty in patients 80 years of age and older, Clin Orthop Relat Res 299:77, 1994.
- Jankiewicz JJ, Sculco TP, Ranawat CS, et al: One-stage versus two-stage bilateral total knee arthroplasty, Clin Orthop Relat Res 309:94, 1994.
- Keblish PA, Varma AK, Greenwald AS: Patellar resurfacing or retention in total knee arthroplasty, J Bone Joint Surg 76B:930, 1994.
- Kolettis GT, Wixson RL, Peruzzi WT, et al: Safety of one-stage bilateral total knee arthroplasty, Clin Orthop Relat Res 309:102, 1994.
- Kozinn SC, Scott RD: Unicondylar knee arthroplasty, J Bone Joint Surg 71A:145, 1989.
- Kulkarni S, Sawant M, Ireland J: Allograft reconstruction of the extensor mechanism for progressive extensor lag after total knee arthroplasty and previous patellectomy: a 3-year followup, J Arthroplasty 14:892, 1999.
- Lane GJ, Hozack WJ, Shah S, et al: Simultaneous bilateral versus unilateral total knee arthroplasty, Clin Orthop Relat Res 345:106, 1997.
- Levine WN, Ozuna RM, Scott RD, Thornhill TS: Conversion of failed modern unicompartmental arthroplasty to total knee arthroplasty, J Arthroplasty 11:797, 1996.
- Levitsky KA, Harris WJ, McManus J, et al: Total knee arthroplasty without patellar resurfacing: clinical outcomes and longterm follow-up evaluation, Clin Orthop Relat Res 286:116, 1993.
- Lynch NM, Trousdale RT, Ilstrup DM: Complications after concomitant bilateral total knee arthroplasty in elderly patients, Mayo Clin Proc 72:799, 1997.
- McLaughlin TP, Fisher RL: Bilateral total knee arthroplasties: comparison of simultaneous (two-team), sequential and staged knee replacements, Clin Orthop Relat Res 199:220, 1985.
- Padgett DE, Stern SH, Insall JN: Revision total knee arthroplasty for failed unicompartmental replacement, J Bone Joint Surg 73A:186, 1991.
- Ranawat CS: The patellofemoral joint in total condylar knee arthroplasty: pros and cons based on fi veto ten-year followup observations, Clin Orthop Relat Res 205:93, 1986.
- Rand JA: The patellofemoral joint in total knee arthroplasty, J Bone Joint Surg 76A:612, 1994.
- Scott RD, Reilly DT: Pros and cons of patella resurfacing in total knee replacement, Orthop Trans 4:328, 1980.
- Scuderi GR, Insall JN, Windsor RE, et al: Survivorship of cemented knee replacement, J Bone Joint Surg 71B:798, 1989.
- Smith BE, Askew MJ, Gradisar IA, et al: The effect of patient weight on the functional outcome of total knee arthroplasty, Clin Orthop Relat Res 276:237, 1992.
- Soudry M, Binazzi R, Insall JN, et al: Successive bilateral total knee replacement, J Bone Joint Surg 67A:573, 1985.
- Stern SH, Becker MW, Insall JN: Unicondylar knee arthroplasty: an evaluation of selection criteria, Clin Orthop Relat Res 286:143, 1993.
- Stern SH, Sharrock N, Kahn R, et al: Hematologic and circulatory changes associated with total knee arthroplasty instrumentation, Clin Orthop Relat Res 299:179, 1994.
- Thornhill TS, Scott RD: Unicompartmental total knee arthroplasty, Orthop Clin North Am 20:245, 1989.
- Wapner JL: Rationale for staged versus simultaneous bilateral total knee replacements, Orthop Trans 8:398, 1984.
- Zicat B, Rorabeck CH, Bourne RB, et al: Total knee arthroplasty in the octogenarian, J Arthroplasty 8:395, 1993.
- Results of Total Knee Arthroplasty Adili A, Bhandari M, Petruccelli D, et al: Sequential bilateral total knee arthroplasty under 1 anesthetic in patients > or = 75 years old: complications and functional outcomes, J Arthroplasty 16:271, 2001.
- Andriacchi TP, Galante JO, Fermier RW: The infl uence of total knee replacement design on walking and stair climbing, J Bone Joint Surg 64A:1328, 1982.
- Armstrong RA, Whiteside LA: Results of cementless total knee arthroplasty in an older rheumatoid arthritis population, J Arthroplasty 6:357, 1991.
- Barrack RL, Nakamura SJ, Hopkins SG, et al: Winner of the 2003 James A. Rand Young Investigator’s Award. Early failure of cementless mobile-bearing total knee arthroplasty, J Arthroplasty 19(7 suppl 2):101, 2004.
- Benson ER, Resine ST, Lewis CG: Functional outcome of arthrodesis for failed total knee arthroplasty, Orthopedics 21:875, 1998.
- Berend KR, Lombardi AV Jr, Mallory TH, et al: Early failure of minimally invasive unicompartmental knee arthroplasty is associated with obesity, Clin Orthop Relat Res 440:60, 2005.
- Berger RA, Lyon JH, Jacobs JJ, et al: Problems with cementless total knee arthroplasty at 11 years followup, Clin Orthop Relat Res 392:196, 2001.
- Buechel FF: Long-term outcomes and expectations: cementless meniscal bearing knee arthroplasty: 7to 12-year outcome analysis, Orthopedics 17:833, 1994.
- Buechel FF Sr: Long-term followup after mobile-bearing total knee replacement, Clin Orthop Relat Res 404:40, 2002.
- Bullock DP, Sporer SM, Shirreffs TG Jr: Comparison of simultaneous bilateral with unilateral total knee arthroplasty in terms of perioperative complications, J Bone Joint Surg 85A:1981, 2003.
- Callahan CM, Drake BG, Heck DA, et al: Patient outcomes following unicompartmental or bicompartmental knee arthroplasty: a meta-analysis, J Arthroplasty 10:141, 1995.
- Crowder AR, Duffy GP, Trousdale RT: Long-term results of total knee arthroplasty in young patients with rheumatoid arthritis, J Arthroplasty 20(7 suppl 3):12, 2005.
- Dennis DA, Clayton ML, O’Donnell S, et al: Posterior cruciate condylar total knee arthroplasty: average 11-year follow-up examination, Clin Orthop Relat Res 281:168, 1992.
- Dennis DA, Komistek RD, Stiehl JB, et al: Range of motion after total knee arthroplasty: the effect of implant design and weight-bearing conditions, J Arthroplasty 13:748, 1998.
- Dixon MC, Brown RR, Parsch D, et al: Modular fi xed-bearing total knee arthroplasty with retention of the posterior cruciate ligament: a study of patients followed for a minimum of fi fteen years, J Bone Joint Surg 87A:598, 2005.
- Duffy GP, Berry DJ, Rand JA: Cement versus cementless fi xation in total knee arthroplasty, Clin Orthop Relat Res 356:66, 1998.
- Ecker ML, Lotke PA, Windsor RE, et al: Long-term results after total condylar knee arthroplasty: signifi cance of radiolucent lines, Clin Orthop Relat Res 216:151, 1987.
- Elkus M, Ranawat CS, Rasquinha VJ, et al: Total knee arthroplasty for severe valgus deformity: fi ve to fourteen-year followup, J Bone Joint Surg 86A:2671, 2004.
- Ewald FC: The Knee Society total knee arthroplasty roentgenographic evaluation and scoring system, Clin Orthop Relat Res 248:9, 1989.
- Ewald FC, Wright J, Poss R, et al: Kinematic total knee arthroplasty: a 10to 14-year prospective follow-up review, J Arthroplasty 14:473, 1999.
- Fetzer GB, Callaghan JJ, Templeton JE, et al: Posterior cruciate–retaining modular total knee arthroplasty: a 9to 12-year follow-up investigation, J Arthroplasty 17:961, 2002.
- Gill GS, Joshi AB: Long-term results of cemented, posterior cruciate ligament-retaining total knee arthroplasty in osteoarthritis, Am J Knee Surg 14:209, 2001.
- Gill GS, Joshi AB, Mills DM: Total condylar knee arthroplasty, Clin Orthop Relat Res 367:210, 1999.
- Hartford JM, Goodman SB, Schurman DJ, et al: Complex primary and revision total knee arthroplasty using the condylar constrained prosthesis: an average 5-year follow-up, J Arthroplasty 13:380, 1998.
- Hofmann AA, Heithoff SM, Camargo M: Cementless total knee arthroplasty in patients 50 years or younger, Clin Orthop Relat Res 404:102, 2002.
- Hohl WM, Crawfurd E, Zelicof SB, et al: The total condylar III prosthesis in complex knee reconstruction, Clin Orthop Relat Res 273:91, 1991.
- Hungerford DJ, Krackow KA, Kenna RV: Twoand fi ve-year experience with a cementless porous coated total knee prosthesis. In Rand JA, Dorr LD, eds: Total arthroplasty of the knee, Rockville, Md, 1987, Aspen. Insall JN, Dorr LD, Scott RD, et al: Rationale of the Knee Society clinical rating system, Clin Orthop Relat Res 248:13, 1989.
- Kelly MA, Clarke HD: Long-term results of posterior cruciate– substituting total knee arthroplasty, Clin Orthop Relat Res 404:51, 2002.
- Knutson K, Lewold S, Robertsson O, et al: The Swedish knee arthroplasty register: a nation-wide study of 30,003 knees, 1976-1992, Acta Orthop Scand 65:375, 1994.
- Kobs JK, Lachiewicz PF: Hybrid total knee arthroplasty: twoto fi ve-year results using the Miller-Galante prosthesis, Clin Orthop Relat Res 286:78, 1993.
- Lachiewicz PF, Falatyn SP: Clinical and radiographic results of the total condylar III and constrained condylar total knee arthroplasty, J Arthroplasty 11:916, 1996.
- Laskin RS: Total knee arthroplasty using an uncemented, polyethylene tibial implant: a seven-year follow-up study, Clin Orthop Relat Res 288:270, 1993.
- Laskin RS: The Genesis total knee prosthesis: a 10-year followup study, Clin Orthop Relat Res 388:95, 2001.
- Lawrence T, Moskal JT, Diduch DR: Analysis of routine histological evaluation of tissues removed during primary hip and knee arthroplasty, J Bone Joint Surg 81A:926, 1999.
- Li PLS, Zamora J, Bentley G: The results at ten years of the Insall-Burstein II total knee replacement: clinical, radiological, and survivorship studies, J Bone Joint Surg 81B:647, 1999.
- Lizaur A, Marco L, Cebrian R: Preoperative factors infl uencing the range of movement after total knee arthroplasty for severe osteoarthritis, J Bone Joint Surg 79B:626, 1997.
- Maloney WJ, Schurman DJ: The effects of implant design on range of motion after total knee arthroplasty: total condylar versus posterior stabilized total condylar designs, Clin Orthop Relat Res 278:147, 1992.
- McCaskie AW, Deehan DJ, Green TP, et al: Randomised, prospective study comparing cemented and cementless total knee replacement, J Bone Joint Surg 80B:971, 1998.
- Mont MA, Yoon T-R, Krackow KA, et al: Eliminating patellofemoral complications in total knee arthroplasty: clinical and radiographic results of 121 consecutive cases using the Duracon system, J Arthroplasty 14:446, 1999.
- Nelissen RGHH, Brand R, Rozing PM: Survivorship analysis in total condylar knee arthroplasty, J Bone Joint Surg 74A:383, 1992.
- Parsley BS, Engh GA, Dwyer KA: Preoperative fl exion: does it infl uence postoperative fl exion after posterior-cruciate-retaining total knee arthroplasty? Clin Orthop Relat Res 275:204, 1992.
- Pavone V, Boettner F, Fickert S, et al: Total condylar knee arthroplasty: a long-term followup, Clin Orthop Relat Res 388:18, 2001.
- Rader CP, Löhr J, Wittmann R, et al: Results of total knee arthroplasty with a metal-backed patellar component: a 6-year follow-up study, J Arthroplasty 11:923, 1996.
- Ranawat CS, Boachie-Adjei O: Survivorship analysis and results of total condylar knee arthroplasty: eight to 11-year follow-up period, Clin Orthop Relat Res 226:6, 1998.
- Ranawat CS, Flynn WF, Deshmukh RG: Impact of modern technique on long-term results of total condylar knee arthroplasty, Clin Orthop Relat Res 309:131, 1994.
- Ranawat CS, Flynn WF, Saddler S, et al: Long-term results of the total condylar knee arthroplasty: a 15-year survivorship study, Clin Orthop Relat Res 286:94, 1993.
- Rand JA: Comparison of metal-backed and all-polyethylene tibial components in cruciate condylar total knee arthroplasty, J Arthroplasty 8:307, 1993.
- Rand JA, Ilstrup DM: Survivorship analysis of total knee arthroplasty, J Bone Joint Surg 73A:397, 1991.
- Ritter MA, Campbell E, Faris P, et al: Long-term survival analysis of the posterior cruciate condylar total knee arthroplasty: a 10-year evaluation, J Arthroplasty 4:293, 1989.
- Ritter MA, Harty LD, Davis KE, et al: Simultaneous bilateral, staged bilateral, and unilateral total knee arthroplasty: a survival analysis, J Bone Joint Surg 85A:1532, 2003.
- Ritter MA, Herbst SA, Keating EM, et al: Long-term survival analysis of a posterior cruciate–retaining total condylar total knee arthroplasty, Clin Orthop Relat Res 309:136, 1994.
- Robertsson O, Scott G, Freeman MA: Ten-year survival of the cemented Freeman-Samuelson primary knee arthroplasty: data from the Swedish Knee Arthroplasty Register and the Royal London Hospital, J Bone Joint Surg 82B:506, 2000.
- Rosenthal L, Lepanto L, Raymond F: Radiophosphate uptake in asymptomatic knee arthroplasty, J Nucl Med 28:1546, 1987.
- Schai PA, Thornhill TS, Scott RD: Total knee arthroplasty with the PFC system: results at a minimum of ten years and survivorship analysis, J Bone Joint Surg 80B:850, 1998.
- Scott RD, Joyce MJ, Ewald FC, et al: McKeever metallic hemiarthroplasty of the knee in unicompartmental degenerative arthritis: long-term clinical follow-up and current indications, J Bone Joint Surg 67A:203, 1985.
- Scott WN, Rubinstein M, Scuderi G: Results after knee replacement with a posterior cruciate–substituting prosthesis, J Bone Joint Surg 70A:1163, 1988.
- Scuderi GR, Insall JN: Total knee arthroplasty, Clin Orthop Relat Res 276:26, 1992.
- Sledge CB, Ewald FC: Total knee arthroplasty experience at the Robert Breck Brigham Hospital, Clin Orthop Relat Res 145:78, 1979.
- Sliva CD, Callaghan JJ, Goetz DD, et al: Staggered bilateral total knee arthroplasty performed four to seven days apart during a single hospitalization, J Bone Joint Surg 87A:508, 2005.
- Smith S, Naima VSN, Freeman MAR: The natural history of tibial radiolucent lines in a proximally cemented stemmed total knee arthroplasty, J Arthroplasty 14:3, 1999.
- Weir DJ, Moran CG, Pinder IM: Kinematic condylar total knee arthroplasty: 14-year survivorship analysis of 208 consecutive cases, J Bone Joint Surg 78B:907, 1996.
- Whiteside LA: Cementless total knee replacement: 9to 11-year results and 10-year survivorship analysis, Clin Orthop Relat Res 309:185, 1994.
- Whiteside LA: Long-term followup of the bone-ingrowth Ortholoc knee system without a metal-backed patella, Clin Orthop Relat Res 388:77, 2001.
- Wright RJ, Sledge CB, Poss R, et al: Patient-reported outcome and survivorship after Kinemax total knee arthroplasty, J Bone Joint Surg 86A:2464, 2004.
- Wright TM, Bartel DL: The problem of surface damage in polyethylene total knee components, Clin Orthop Relat Res 205:67, 1986.
- Surgical Technique Akagi M, Mori S, Nishimura S, et al: Variability of extraarticular tibial rotation references for total knee arthroplasty, Clin Orthop Relat Res 436:172, 2005.
- Arima J, Whiteside LA, McCarthy DS, et al: Femoral rotational alignment, based on the anteroposterior axis in total knee arthroplasty in a valgus knee, J Bone Joint Surg 77A:1331, 1995.
- Berger RA, Rubash HE, Seel MJ, et al: Determining the rotational alignment of the femoral component in total knee arthroplasty using the epicondylar axis, Clin Orthop Relat Res 286:40, 1993.
- Brand MG, Daley FJ, Ewald FC, et al: Tibial tray augmentation with modular metal wedges for tibial bone stock defi ciency, Clin Orthop Relat Res 248:71, 1989.
- Brys DA, Lombardi AV, Mallory TH, et al: A comparison of intramedullary and extramedullary alignment systems for tibial component placement in total knee arthroplasty, Clin Orthop Relat Res 263:175, 1991.
- Burkart BC, Bourne RB, Rorabeck CH, et al: The effi cacy of tourniquet release in blood conservation after total knee arthroplasty, Clin Orthop Relat Res 299:147, 1994.
- Cooper RE, Trinidad G, Buck WR: Midvastus approach in total knee arthroplasty: a description and a cadaver study determining the distance of the popliteal artery from the patellar margin of the incision, J Arthroplasty 14:505, 1999.
- Dennis DA, Channer M, Susman MH, et al: Intramedullary versus extramedullary tibial alignment systems in total knee arthroplasty, J Arthroplasty 8:43, 1993.
- Dorr LD, Merkel C, Mellman MF, et al: Fat emboli in bilateral total knee arthroplasty: predictive factors for neurologic manifestations, Clin Orthop Relat Res 248:112, 1989.
- Emerson RH, Ayers C, Higgins LL: Surgical closing in total knee arthroplasty, Clin Orthop Relat Res 368:176, 1999.
- Engh GA, Holt BT, Parks NL: A midvastus muscle-splitting approach for total knee arthroplasty, J Arthroplasty 12:322, 1997.
- Engh GA, Parks NL: Surgical technique of the midvastus arthrotomy, Clin Orthop Relat Res 351:270, 1998.
- Fahmy NR, Chandler HP, Danylchuk K, et al: Blood-gas and circulatory changes during total knee replacement: role of the intramedullary alignment rod, J Bone Joint Surg 72A:19, 1990.
- Firestone TP, Krackow KA, Davis JD IV, et al: The management of fi xed fl exion contractures during total knee arthroplasty, Clin Orthop Relat Res 284:221, 1992.
- Fisher DA, Trimble SM, Breedlove K: The medial trivector approach in total knee arthroplasty, Orthopedics 21:53, 1998.
- Gore DR, Sellinger DS, Gassner KJ, et al: Subvastus approach for total knee arthroplasty, Orthopedics 26:33, 2003.
- Hofmann AA, Bloebaum RD, Rubman MH, et al: Microscopic analysis of autograft bone applied at the interface of porouscoated devices in human cancellous bone, Int Orthop 16:349, 1992.
- Hofmann AA, Plaster RL, Murdock LE: Subvastus (southern) approach for primary total knee arthroplasty, Clin Orthop Relat Res 269:70, 1991.
- Husted H, Toftgaard Jensen T: Infl uence of the pneumatic tourniquet on patella tracking in total knee arthroplasty: a prospective randomized study in 100 patients, J Arthroplasty 20:694, 2005.
- Insall J: A midline approach to the knee, J Bone Joint Surg 53A:1584, 1971.
- Insall JN: Technique of total knee replacement, Instr Course Lect 30:324, 1981.
- Insall JN: Surgical techniques and instrumentation in total knee arthroplasty. In Insall JN, ed: Surgery of the knee, New York, 1993, Churchill Livingstone. Jenny JY, Clemens U, Kohler S, et al: Consistency of implantation of a total knee arthroplasty with a non-image-based navigation system: a case-control study of 235 cases compared with 235 conventionally implanted prostheses, J Arthroplasty 20:832, 2005.
- Katz MA, Beck TD, Silber JS, et al: Determining femoral rotational alignment in total knee arthroplasty: reliability of techniques, J Arthroplasty 16:301, 2001.
- [Krackow KA: The technique of total knee arthroplasty, St Louis, 1990, Mosby.
Krackow KA, Mihalko WM: Flexion-extension joint gap changes after lateral structure release for valgus deformity correction in total knee arthroplasty, J Arthroplasty 14:994, 1999.](https://pubmed.ncbi.nlm.nih.gov/?term=Krackow%20KA%3A%20The%20technique%20of%20total%20knee%20arthroplasty%2C%20St%20Louis%2C%201990%2C%20Mosby.%0A%0AKrackow%20KA%2C%20Mihalko%20WM%3A%20Flexion-extension%20joint%20gap%20changes%20after%20lateral%20structure%20release%20for%20valgus%20deformity%20correction%20in%20total%20knee%20arthroplasty%2C%20J%20Arthroplasty%2014%3A994%2C%201999.)
- Lombardi AV Jr, Mallory TH, Fada RA, et al: An algorithm for the posterior cruciate ligament in total knee arthroplasty, Clin Orthop Relat Res 392:75, 2001.
- Mantas JP, Bloebaum RD, Skedros JG, et al: Implications of reference axes used for rotational alignment of the femoral component in primary and revision knee arthroplasty, J Arthroplasty 7:531, 1992.
- Marson BM, Tokish JT: The effect of a tourniquet on intraoperative patellofemoral tracking during total knee arthroplasty, J Arthroplasty 14:197, 1999.
- Mihalko WM, Krackow KA: Posterior cruciate ligament effects on the fl exion space in total knee arthroplasty, Clin Orthop Relat Res 360:243, 1999.
- Mihalko WM, Whiteside LA: Bone resection and ligament treatment for fl exion contracture in knee arthroplasty, Clin Orthop Relat Res 406:141, 2003.
- Miller MC, Berger RA, Petrella AJ, et al: Optimizing femoral component rotation in total knee arthroplasty, Clin Orthop Relat Res 392:38, 2001.
- Parker MJ, Roberts CP, Hay D: Closed suction drainage for hip and knee arthroplasty: a meta-analysis, J Bone Joint Surg 86A:1146, 2004.
- Perlick L, Bathis H, Tingart M, et al: Navigation in total-knee arthroplasty: CT-based implantation compared with the conventional technique, Acta Orthop Scand 75:567, 2004.
- Rand JA: Cemented total knee arthroplasty. In Morrey BF, ed: Reconstructive surgery of the joints, New York, 1996, Churchill Livingstone. Raut VV, Stone MH, Wroblewski BM: Reduction of postoperative blood loss after press-fi t condylar knee arthroplasty with use of a femoral intramedullary plug, J Bone Joint Surg 75A:1356, 1993.
- Ritter MA, Faris PM, Keating EM: Posterior cruciate ligament balancing during total knee arthroplasty, J Arthroplasty 3:323, 1988.
- Ritter MA, Harty LD: Medial screws and cement: a possible mechanical augmentation in total knee arthroplasty, J Arthroplasty 19:587, 2004.
- Ritter MA, Keating EM, Faris PM: Screw and cement fi xation of large defects in total knee arthroplasty, J Arthroplasty 8:63, 1993.
- Ritter MA, Pierce MJ, Zhou H, et al: Patellar complications (total knee arthroplasty): effect of lateral release and thickness, Clin Orthop Relat Res 367:149, 1999.
- Ritter MA, Stringer EA: Predictive range of motion after total knee replacement, Clin Orthop Relat Res 143:115, 1979.
- Schurman D, Parker J, Ornstein D: Total condylar knee replacements: a study of factors infl uencing range of motion as late as two years after arthroplasty, J Bone Joint Surg 67A:1006, 1985.
- Simmons ED, Sullivan JA, Rackemann S, et al: The accuracy of tibial intramedullary alignment devices in total knee arthroplasty, J Arthroplasty 6:45, 1991.
- Siston RA, Patel JJ, Goodman SB, et al: The variability of femoral rotational alignment in total knee arthroplasty, J Bone Joint Surg 87A:2276, 2005.
- Stern SH, Sharrock N, Kahn R, et al: Hematologic and circulatory changes associated with total knee arthroplasty surgical instrumentation, Clin Orthop Relat Res 299:179, 1994.
- Swany MR, Scott RD: Posterior polyethylene wear in posterior cruciate ligament-retaining total knee arthroplasty, J Arthroplasty 8:4839, 1993.
- Tanzer M, Miller J: The natural history of fl exion contracture in total knee arthroplasty, Clin Orthop Relat Res 248:129, 1989.
- Tew M, Forster IW: Effect of knee replacement on fl exion deformity, J Bone Joint Surg 69B:395, 1987.
- Victor J, Hoste D: Image-based computer-assisted total knee arthroplasty leads to lower variability in coronal alignment, Clin Orthop Relat Res 428:131, 2004.
- Whiteside LA: Selective ligament release in total knee arthroplasty of the knee in valgus, Clin Orthop Relat Res 367:130, 1999.
- Whiteside LA, Arima J: The anteroposterior axis for femoral rotational alignment in valgus total knee arthroplasty, Clin Orthop Relat Res 321:168, 1995.
- Windsor RE, Insall JN, Sculco TP:
You Might Also Like


