Chondrosarcoma Diagnosis: A Detailed Clinical & Imaging Case Study

Key Takeaway
Diagnosing distal femur chondrosarcoma starts with X-rays revealing lytic lesions and 'rings and arcs' calcification. MRI details soft tissue extension; CT maps cortical destruction; PET-CT aids systemic staging. Definitive diagnosis relies on image-guided biopsy, confirming atypical chondrocytes and tumor grade, as exemplified by this Grade II case.
Patient Presentation and History
A 58-year-old male presents to the orthopedic oncology clinic with a chief complaint of insidious onset, progressively worsening left distal thigh pain over the past eight months. Initially, the pain was characterized as dull and intermittent, primarily exacerbated by weight-bearing and moderate physical activity. Over the preceding two months, the clinical picture has evolved significantly; the pain has transitioned to a constant, deep ache that persists at rest and frequently disrupts his sleep architecture. This transition from mechanical-type pain to biological, rest-associated pain is a critical historical hallmark suggestive of an aggressive osseous process.
The patient denies any acute traumatic events, previous fractures, or sports-related injuries to the affected extremity. A comprehensive review of systems is negative for constitutional "B-symptoms," including unexplained weight loss, fever, chills, or night sweats. He reports no preceding systemic infections or illnesses. Pharmacological management prior to presentation consisted of over-the-counter non-steroidal anti-inflammatory drugs and acetaminophen, which provided only minimal and transient symptomatic relief.
His past medical history is notable for essential hypertension and dyslipidemia, both of which are well-controlled with a daily regimen of an ACE inhibitor and a statin. He is a former smoker with a 20 pack-year history, having achieved smoking cessation ten years prior to presentation. There is no known personal history of prior malignancies or radiation exposure. Family history is negative for bone tumors, soft tissue sarcomas, or known genetic cancer predisposition syndromes such as Li-Fraumeni syndrome or hereditary multiple exostoses. Occupationally, he is a retired machinist, a role that involved moderate physical exertion but no specific occupational hazards directly linked to primary bone sarcomas.
Clinical Examination Findings
On general inspection, the patient appears well-nourished and comfortable while seated at rest. Gait analysis reveals an antalgic gait favoring the left lower extremity, with a shortened stance phase on the affected side. Inspection of the left lower extremity demonstrates a subtle but distinct fullness over the lateral aspect of the distal thigh, immediately superior to the knee joint line. There is no obvious skin discoloration, venous engorgement, localized warmth, or overlying erythema to suggest an acute infectious process or superficial vascular malformation. Noticeable muscle atrophy is present within the left quadriceps muscle belly compared to the contralateral limb, indicative of chronic disuse secondary to pain.
Palpation of the left distal femur reveals a firm, fixed, and non-mobile mass located deep within the vastus lateralis musculature, approximately 10 centimeters proximal to the lateral femoral condyle. The mass measures approximately 6 by 4 centimeters in its palpable dimensions. It appears to be contiguous with the underlying osseous structures, suggesting a bone-derived pathology rather than an isolated soft tissue sarcoma. Palpation of the mass elicits mild discomfort but no exquisite tenderness. There is no palpable crepitus, fluctuance, or localized hyperthermia.
Range of motion testing of the left knee demonstrates a painful arc of motion. Active flexion is limited to 90 degrees, with significant pain experienced at the terminal ends of both flexion and extension. Passive range of motion is similarly restricted by pain and mechanical guarding, suggesting that the mass may be tethering the extensor mechanism or causing significant periosteal irritation. Hip and ankle range of motion are preserved and painless.
Neurological assessment of the left lower extremity reveals intact light touch and pinprick sensation across the L2 through S1 dermatomal distributions. Motor strength testing demonstrates 4/5 strength for knee extension, limited primarily by pain inhibition, while ankle dorsiflexion, plantarflexion, hip flexion, and hip extension remain 5/5 and symmetric to the contralateral side. Deep tendon reflexes, including the patellar and Achilles reflexes, are graded as 2+ and symmetric bilaterally. Vascular examination confirms palpable and symmetric femoral, popliteal, dorsalis pedis, and posterior tibial pulses. There is no evidence of distal ischemia, edema, or compartment syndrome. Palpation of the inguinal region reveals no regional lymphadenopathy.
Imaging and Diagnostics
The diagnostic workup for suspected primary bone tumors necessitates a multimodal imaging approach to evaluate the local extent of the lesion, characterize the tumor matrix, and stage the patient for potential distant metastatic disease.
Radiographic Evaluation
Initial imaging included standard anteroposterior and lateral plain radiographs of the left femur and knee. The radiographs revealed a large, lytic lesion centered within the metadiaphyseal region of the distal femur. The lesion demonstrated an aggressive radiographic appearance characterized by ill-defined margins and a wide zone of transition. Significant endosteal scalloping was present, accompanied by frank cortical destruction, particularly localized to the lateral cortex.
Within the radiolucent matrix of the lesion, areas of faint, irregular calcification were clearly identified. These calcifications exhibited the classic "rings and arcs" and "flocculent" morphology, which is highly pathognomonic for a chondroid matrix. A patchy and discontinuous periosteal reaction was observed, indicative of a biological process that is expanding rapidly enough to outpace the periosteum's ability to lay down mature reactive bone. While severe cortical thinning and erosion were evident, no complete pathological fracture was identified.
Advanced Cross Sectional Imaging
To precisely define the local anatomical extent, marrow involvement, and soft tissue extension, a dedicated Magnetic Resonance Imaging scan of the left femur with and without intravenous gadolinium contrast was obtained.
The MRI revealed a large, lobulated intraosseous lesion centered in the distal femoral metadiaphysis, extending approximately 10 centimeters longitudinally within the medullary canal. The lesion demonstrated characteristic signal intensities for a cartilaginous tumor: markedly hypointense on T1-weighted sequences and hyperintense on T2-weighted fluid-sensitive sequences. The high T2 signal correlates with the high water content typical of hyaline cartilage.
Internal septations and nodularity were prominent features. Following the administration of gadolinium contrast, significant peripheral and septal enhancement was observed, creating a classic "lobular" enhancement pattern. Crucially, the MRI confirmed the plain radiographic findings of cortical destruction, demonstrating frank extraosseous soft tissue extension into the vastus lateralis muscle belly. This extracompartmental extension confirms the aggressive, high-grade nature of the lesion and is a critical factor in surgical planning. The neurovascular bundle, including the superficial femoral artery and vein within the adductor canal, remained free of tumor involvement, with a clear fat plane preserved medially.

A computed tomography scan of the left femur was also obtained to provide superior resolution of the cortical bone architecture, confirming the exact dimensions of the cortical breach and assisting in the precise templating of the planned osteotomy level. For systemic staging, a high-resolution CT scan of the chest, abdomen, and pelvis was performed, which demonstrated no evidence of pulmonary nodules or visceral metastatic disease. A whole-body technetium-99m methylene diphosphonate bone scan showed intense, isolated focal uptake corresponding to the distal femoral lesion, with no other sites of skeletal metastasis.
Histopathological Analysis
Following the imaging workup, an image-guided core needle biopsy was performed. The biopsy tract was meticulously planned in consultation with the orthopedic oncology team to ensure that the entire tract could be excised en bloc during the definitive surgical resection. The biopsy was performed via a lateral approach, directly through the vastus lateralis, avoiding contamination of the anterior extensor mechanism or the medial neurovascular structures.
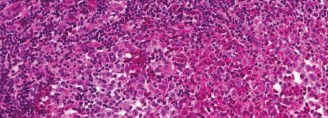
Histopathological examination of the core biopsy specimens revealed a hypercellular cartilaginous neoplasm. The chondrocytes exhibited moderate to severe nuclear atypia, pleomorphism, and frequent binucleation. The surrounding stroma showed areas of myxoid degeneration, a feature often associated with higher-grade chondrosarcomas. Mitotic figures were present but not abundant. Importantly, there was no evidence of malignant osteoid production by the tumor cells, effectively ruling out a chondroblastic osteosarcoma. Based on the cellularity, nuclear atypia, and myxoid changes, the lesion was classified as a Grade 2 (intermediate-grade) conventional chondrosarcoma.

Differential Diagnosis
The presentation of a destructive, matrix-producing bone lesion in an adult necessitates a structured differential diagnosis. The primary considerations include various benign and malignant cartilaginous tumors, as well as other primary bone sarcomas and metastatic disease.
| Pathology | Typical Demographics | Radiographic Characteristics | Clinical and Histological Features |
|---|---|---|---|
| Conventional Chondrosarcoma | Adults > 40 years old. | Lytic lesion, ill-defined margins, endosteal scalloping > 2/3 cortical thickness, cortical destruction, "rings and arcs" calcification. | Pain at rest/night. Histology shows atypical chondrocytes, hypercellularity, binucleation, and host bone entrapment. |
| Enchondroma | 20 - 50 years old. | Well-circumscribed, medullary lesion, intact cortex, stippled calcification. No significant endosteal scalloping. | Usually asymptomatic, discovered incidentally. Histology shows mature, hypocellular hyaline cartilage without atypia. |
| Osteosarcoma (Chondroblastic) | Bimodal: Teens/young adults, and > 65 years (secondary). | Aggressive, mixed lytic/sclerotic lesion, destructive, prominent periosteal reaction (Codman's triangle, sunburst). | Rapidly progressive pain, swelling. Histology MUST show malignant cells producing osteoid matrix, even if cartilage dominates. |
| Metastatic Carcinoma | Adults > 50 years old. | Typically purely lytic (e.g., renal, thyroid, lung) or blastic (prostate, breast). Usually lacks chondroid matrix. | History of primary carcinoma. Multiple lesions common. Histology matches the primary epithelial malignancy. |
Diagnostic Distinctions
Differentiating between a benign enchondroma and a low-to-intermediate grade chondrosarcoma is one of the most challenging tasks in musculoskeletal oncology. In this case, several factors point definitively toward a malignant process. Clinically, the presence of progressive, non-mechanical pain, particularly at night, is a red flag. Radiographically, the size of the lesion (greater than 5 cm), the presence of deep endosteal scalloping (eroding more than two-thirds of the cortical thickness), frank cortical breakthrough, and the development of an associated soft tissue mass are all definitive indicators of malignancy.
Chondroblastic osteosarcoma was considered due to the aggressive nature of the lesion; however, the patient's age makes primary osteosarcoma less likely, and the definitive lack of malignant osteoid on the biopsy specimen rules out this diagnosis. Metastatic disease was considered given the patient's age and smoking history, but the distinct chondroid matrix on imaging and the primary cartilaginous histology confirm a primary bone sarcoma.
Surgical Decision Making and Classification
The management of conventional chondrosarcoma is fundamentally surgical. Unlike osteosarcoma and Ewing sarcoma, conventional chondrosarcomas are notoriously resistant to both systemic chemotherapy and radiation therapy. This inherent chemoresistance is attributed to the tumor's poor vascularity, low fraction of dividing cells, and the dense extracellular cartilaginous matrix that impedes drug delivery. Consequently, the primary prognostic factor for overall survival and local recurrence is the achievement of wide surgical margins.
Oncologic Staging and Tumor Characteristics
Using the Enneking Surgical Staging System for benign and malignant bone tumors, this lesion is classified as a Stage IIB tumor. Stage II denotes a high-grade malignancy (Grade 2 histology is considered intermediate-to-high grade in this context due to its biological behavior), and "B" denotes an extracompartmental location, evidenced by the cortical breakthrough and extension into the vastus lateralis muscle.
According to the American Joint Committee on Cancer staging system, this would be classified as a Stage IIA (T1, N0, M0, Grade 2) or potentially Stage III depending on the exact longitudinal dimension exceeding 8 cm. Regardless of the specific staging nomenclature, the biological aggressiveness of a Grade 2 chondrosarcoma with soft tissue extension mandates an en bloc wide resection. Intralesional procedures, such as curettage and cryotherapy, are contraindicated for Grade 2 and Grade 3 lesions due to unacceptably high local recurrence rates.
Reconstructive Options and Implant Selection
The necessity for a wide resection of the distal femur presents a significant reconstructive challenge. The goals of reconstruction are to provide immediate structural stability, restore limb length and alignment, preserve joint kinematics, and allow for early mobilization.
Options for distal femoral reconstruction include osteoarticular allografts, allograft-prosthetic composites, and modular endoprosthetic reconstruction (megaprosthesis). In a 58-year-old patient, modular endoprosthetic reconstruction is the gold standard. It allows for immediate weight-bearing, avoids the risks of disease transmission and non-union associated with massive allografts, and provides a highly customizable reconstruction based on the exact length of the intraoperative resection.
A rotating hinge knee mechanism is required for the distal femoral replacement. Because the resection necessitates the removal of the collateral ligaments and the cruciate ligaments along with the distal femur, a standard constrained condylar knee is insufficient. A rotating hinge prosthesis provides the necessary coronal and sagittal plane stability while allowing for a degree of axial rotation, which significantly reduces the torsional stresses transmitted to the stem-cement-bone interface, thereby mitigating the risk of aseptic loosening.
Surgical Technique and Intervention
The patient was medically optimized and cleared for surgery. The procedure planned was a wide en bloc resection of the left distal femur, including the biopsy tract, with modular distal femoral endoprosthetic reconstruction.
Patient Positioning and Operating Room Setup
The patient was placed supine on a radiolucent operating table to facilitate intraoperative fluoroscopy. A bump was placed under the ipsilateral hip to prevent external rotation of the lower extremity. A sterile tourniquet was applied to the proximal thigh but not inflated, as exsanguination of a limb harboring a malignancy is generally avoided to prevent potential systemic embolization of tumor cells. The entire left lower extremity, from the iliac crest to the toes, was prepped and draped in a standard sterile fashion. Prophylactic intravenous antibiotics (Cefazolin) were administered prior to incision.
Surgical Approach and Tumor Resection
An extensile anterolateral approach to the distal femur was utilized. The skin incision incorporated the previous core needle biopsy tract in an elliptical fashion to ensure it was excised en bloc with the tumor specimen. The incision was carried distally over the lateral border of the patella and extended to the tibial tubercle.
Subcutaneous tissues were divided, and the fascia lata was incised. The vastus lateralis was identified. Because the MRI demonstrated tumor extension into the vastus lateralis, a cuff of normal muscle tissue surrounding the tumor extension was left attached to the femur. The vastus intermedius was elevated off the anterior femur well proximal to the tumor extent.
Medially, the superficial femoral artery and vein were carefully identified as they exited the adductor canal at the adductor hiatus. The vessels were meticulously dissected free from the posterior aspect of the distal femur and retracted gently using vessel loops. The sciatic nerve was identified posteriorly and protected throughout the procedure.
Based on preoperative MRI measurements, the planned femoral osteotomy site was marked 3 centimeters proximal to the most proximal extent of the marrow abnormality. Intraoperative fluoroscopy confirmed the level. A transverse osteotomy was performed using an oscillating saw. A sample of the proximal medullary canal marrow was immediately sent for frozen section analysis, which confirmed negative margins for malignant cells.
Distally, the knee joint was accessed via a lateral parapatellar arthrotomy. The anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, and lateral collateral ligament were sequentially released from their femoral attachments. The posterior capsule was sharply divided, taking extreme care to protect the popliteal vessels lying immediately posterior to the capsule. The entire distal femur, encompassing the tumor, the biopsy tract, and a cuff of normal surrounding soft tissue, was then delivered en bloc from the surgical field and sent to pathology for definitive margin assessment.
Endoprosthetic Reconstruction
Attention was then turned to the reconstruction. The proximal tibia was prepared for the tibial component of the rotating hinge knee. The tibial plateau was resected perpendicular to the mechanical axis using standard intramedullary alignment guides. The tibial canal was broached, and a cemented tibial baseplate and stem were implanted using polymethylmethacrylate bone cement.
The remaining proximal femur was then prepared. The medullary canal was reamed sequentially to accommodate the femoral stem of the megaprosthesis. The exact length of the resected specimen was measured on the back table to assemble the modular distal femoral components accurately, ensuring restoration of the patient's native leg length.
A cemented, porous-coated titanium femoral stem was selected. A cement restrictor was placed in the femoral canal, the canal was pulsatile lavaged and dried, and PMMA cement was injected in a retrograde fashion. The assembled modular distal femoral prosthesis was inserted, and excess cement was cleared.
Once the cement had cured, the rotating hinge mechanism was linked by inserting the axle through the femoral component and the tibial polyethylene bearing. The knee was taken through a full range of motion, demonstrating excellent stability, full extension, and flexion to 120 degrees. Patellar tracking was assessed; a lateral retinacular release was not required as the patella tracked centrally within the prosthetic trochlear groove.
The soft tissue envelope was meticulously reconstructed. The extensor mechanism is critical following distal femoral replacement. The remaining vastus medialis and rectus femoris were advanced and sutured to the lateral soft tissue sleeve. In cases where the soft tissue envelope is severely compromised, a medial gastrocnemius rotational flap may be required to cover the prosthesis and provide vascularized tissue for extensor mechanism reattachment; however, in this case, adequate local tissue remained for primary closure over a closed suction drain. The subcutaneous tissues and skin were closed in layers.
Post Operative Protocol and Rehabilitation
The postoperative management of a patient undergoing a distal femoral replacement requires a delicate balance between protecting the soft tissue reconstruction and initiating early mobilization to prevent complications.
Acute Inpatient Management
Postoperatively, the patient was admitted to the orthopedic oncology unit. Intravenous antibiotics were continued for 24 hours. Deep vein thrombosis prophylaxis was initiated on postoperative day one using low-molecular-weight heparin, given the high-risk nature of major orthopedic oncology surgery.
The closed suction drain was monitored and removed on postoperative day two when output decreased to less than 30 cc over a 24-hour period. Pain management utilized a multimodal approach, including scheduled acetaminophen, NSAIDs, gabapentin, and judicious use of opioid analgesics.
Physical therapy was consulted on postoperative day one. The patient was allowed immediate weight-bearing as tolerated on the left lower extremity with the assistance of a walker, relying on the immediate stability provided by the cemented diaphyseal fixation. A hinged knee brace locked in extension was utilized during ambulation for the first two weeks to protect the extensor mechanism repair from eccentric loading forces.
Long Term Rehabilitation Strategy
The rehabilitation protocol is phased to ensure progressive functional recovery:
- Phase 1 (Weeks 0-2): Focus on wound healing, edema control, and early mobilization. Weight-bearing as tolerated with assistive devices. Knee range of motion is limited to 0-60 degrees to minimize stress on the capsular closure and extensor mechanism.
- Phase 2 (Weeks 2-6): Progression of range of motion to 0-90 degrees. Initiation of active-assisted quadriceps strengthening and straight leg raises. The hinged knee brace is gradually unlocked during ambulation as quadriceps control improves.
- Phase 3 (Weeks 6-12): Focus on weaning off assistive devices, normalizing gait mechanics, and advanced strengthening, including closed kinetic chain exercises.
- Phase 4 (Months 3-12): Return to functional activities. High-impact activities and running are permanently restricted to prevent premature aseptic loosening or mechanical failure of the endoprosthesis.
Oncologic surveillance is a critical component of postoperative care. For an intermediate-grade chondrosarcoma, the protocol includes physical examination, plain radiographs of the reconstructed limb, and a non-contrast CT scan of the chest every 3 to 4 months for the first two years, every 6 months for years 3 through 5, and annually thereafter. Local recurrence is monitored closely, as it represents a significant risk for subsequent systemic metastasis.
Clinical Pearls and Pitfalls
- Biopsy Tract Placement: The most catastrophic error in orthopedic oncology is an improperly placed biopsy tract that contaminates major neurovascular structures or violates multiple compartments. The biopsy tract must always be placed longitudinally and strictly within the planned excision field.
- Differentiating Chondroid Lesions: Pain is a paramount clinical differentiator. A painful cartilaginous lesion in an adult, particularly pain at rest, must be considered malignant until proven otherwise. Radiographic signs of endosteal scalloping >2/3 of the cortex or soft tissue extension mandate aggressive workup.
- Margin Assessment: Conventional chondrosarcoma does not respond to adjuvant therapies. Therefore, the surgical margin is the sole determinant of local control. Intraoperative frozen sections of the marrow margin are essential before committing to the reconstruction.
- Implant Biomechanics: Utilizing a rotating hinge mechanism rather than a fixed hinge is critical in massive distal femoral replacements. The rotational freedom significantly dissipates torsional forces that would otherwise be transmitted to the cement mantle, delaying the onset of aseptic loosening.
- Extensor Mechanism Protection: Extensor lag is a common complication following distal femoral replacement due to the necessary soft tissue resection. Meticulous closure of the extensor mechanism and a period of protected weight-bearing in extension are crucial to optimize functional outcomes.
You Might Also Like