Correction of Proximal Third Humeral Malunion: Advanced Surgical Techniques and Outcomes
Key Takeaway
Proximal third humeral malunions often result in severe functional impairment, restricted range of motion, and subacromial impingement. Surgical correction requires meticulous preoperative planning, precise corrective osteotomy, and rigid internal fixation, typically utilizing a proximal humeral locking plate. This comprehensive guide details the anterolateral approach, wedge osteotomy execution, and evidence-based postoperative rehabilitation protocols essential for restoring shoulder biomechanics and optimizing patient outcomes in complex humeral deformities.
INTRODUCTION TO PROXIMAL HUMERAL MALUNION
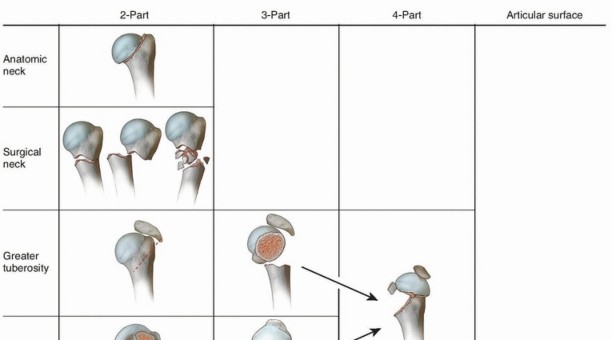
Malunion of the proximal third of the humerus is a complex and functionally debilitating condition that typically arises following the nonoperative management of displaced proximal humerus fractures, or secondary to the failure of primary internal fixation. The proximal humerus possesses a wide range of motion, and while it can tolerate mild degrees of angulation and displacement, severe malunions—particularly those involving varus collapse, severe retroversion, or greater tuberosity displacement—profoundly alter the biomechanics of the glenohumeral joint.
The resulting pathoanatomy frequently leads to subacromial impingement, secondary rotator cuff dysfunction, early-onset glenohumeral arthrosis, and intractable pain. For the practicing orthopaedic surgeon, the correction of a proximal third humeral malunion demands a rigorous understanding of shoulder biomechanics, meticulous preoperative templating, and precise execution of corrective osteotomies.
CLINICAL EVALUATION AND INDICATIONS FOR SURGERY
Patient Presentation
Patients typically present with a history of a proximal humerus fracture managed conservatively or with failed fixation. Chief complaints include chronic shoulder pain, significant limitation in active elevation and external rotation, and profound weakness. A hallmark of varus malunion is the mechanical block to abduction caused by the impingement of the malpositioned greater tuberosity against the acromion.
Radiographic Assessment
Standard trauma series radiographs (true anteroposterior, scapular Y, and axillary lateral views) are mandatory. However, plain films are often insufficient for complex three-dimensional deformities.
* Computed Tomography (CT): A CT scan with 3D reconstruction is the gold standard. It allows for the precise quantification of the angular deformity (varus/valgus), rotational malalignment (version), and the status of the articular surface.
* Magnetic Resonance Imaging (MRI): Indicated if concomitant rotator cuff tearing or severe tendinopathy is suspected, as the integrity of the rotator cuff dictates the ultimate functional outcome and may shift the surgical algorithm toward arthroplasty in older patients.
Indications for Corrective Osteotomy
- Symptomatic malunion with severe pain refractory to conservative management.
- Unacceptable loss of range of motion (e.g., active forward elevation < 90 degrees) directly attributable to the bony deformity.
- Varus angulation exceeding 20 to 30 degrees, leading to persistent subacromial impingement.
- Young, active patients with high functional demands where arthroplasty is contraindicated.
💡 Clinical Pearl: Arthroplasty vs. Osteotomy
In elderly patients with severe osteopenia, advanced glenohumeral osteoarthritis, or massive irreparable rotator cuff tears associated with the malunion, corrective osteotomy carries a high risk of failure. In such cases, reverse total shoulder arthroplasty (RTSA) is the preferred reconstructive option. Osteotomy is reserved for patients with preserved articular cartilage and functional rotator cuffs.
PREOPERATIVE PLANNING AND TEMPLATING
The success of a corrective osteotomy hinges on precise preoperative planning. The surgeon must calculate the exact dimensions of the bony wedge to be resected to restore the normal neck-shaft angle (typically 130 to 140 degrees) and correct any rotational deformity.
- Determine the Apex of Deformity: Identify the center of rotation of angulation (CORA). In proximal third malunions, this is frequently located at the surgical neck.
- Calculate the Wedge Angle: Using digital templating software, superimpose the contralateral (normal) proximal humerus over the deformed side to determine the exact angle of the closing wedge required.
- Implant Selection: While historical techniques utilized standard plates, modern osteopenic bone demands fixed-angle constructs. Pre-select the appropriate length of a proximal humeral locking plate.
SURGICAL ANATOMY AND PATIENT POSITIONING
Positioning
The patient is placed in the beach chair position with the head and neck securely stabilized. The operative arm must be completely free and draped into the sterile field to allow for full intraoperative range of motion and manipulation. A sterile Mayo stand or arm board can be used to support the arm during the osteotomy.
Fluoroscopy Setup
The C-arm should be positioned at the head of the bed or coming in from the contralateral side, ensuring unobstructed orthogonal views (AP and axillary) of the proximal humerus can be obtained without compromising the sterile field.
SURGICAL TECHNIQUE: STEP-BY-STEP CORRECTION
1. The Anterolateral Approach
Expose the fracture through an anterolateral incision 7.5 cm long, centered precisely over the apex of the angulation.
* The anterolateral approach utilizes the internervous plane between the anterior and middle thirds of the deltoid.
* Axillary Nerve Protection: The axillary nerve crosses the operative field approximately 5 to 7 cm distal to the lateral edge of the acromion. It must be meticulously identified, mobilized, and protected with a vessel loop. The dissection must remain proximal and distal to the nerve, creating a "window" for plate insertion if a longer construct is required.
2. Soft Tissue Handling
Extensive stripping of the periosteum is unnecessary and strictly contraindicated. The proximal humerus relies heavily on its periosteal and muscular blood supply (via the anterior and posterior circumflex humeral arteries). Overzealous stripping increases the risk of avascular necrosis (AVN) of the humeral head and nonunion at the osteotomy site. Elevate only enough periosteum to accommodate the osteotomy cuts and the footprint of the plate.
3. The Corrective Osteotomy (Technique 58-22)
Once the apex of the deformity is exposed, the planned osteotomy is executed.
* Wedge Resection: Divide the bone using a sharp, broad osteotome. While an oscillating saw can be used, an osteotome minimizes thermal necrosis and bone loss.
* Remove a wedge of the previously calculated size. For the classic varus malunion, this is a laterally based closing wedge.
* Apex Positioning: The apex of the wedge must be directed at the medial surgical neck. Care must be taken not to breach the medial cortex completely during the initial cut, as an intact medial periosteal hinge greatly enhances stability and aids in reduction.
⚠️ Surgical Warning: The Medial Hinge
If the medial cortex is inadvertently transected or highly comminuted during the osteotomy, the construct loses inherent stability. In such cases, the surgeon must rely entirely on the rigid fixation of the locking plate to prevent varus collapse.
4. Reduction and Provisional Fixation
- Use a bone skid or a broad periosteal elevator to gently lever the fragments into their normal anatomical position, closing the lateral wedge.
- Correct any associated rotational deformity (retroversion/anteversion) at this stage.
- Provisionally hold the reduction with heavy Kirschner wires (K-wires) driven from the lateral cortex into the humeral head.
- Verify the reduction, neck-shaft angle, and hardware placement using orthogonal fluoroscopy.
5. Definitive Internal Fixation
Historically, stabilization of the osteotomy was achieved with a T-shaped plate and 4.5-mm cortical screws. However, modern biomechanical evidence has shifted the paradigm.
* Modern Standard: As recommended by Benegas et al., a locking compression plate system is vastly superior. A proximal humeral locking plate (e.g., PHILOS) provides optimal, fixed-angle fixation. This is particularly critical in the proximal humerus, where cancellous bone quality is often poor, and the deforming forces of the rotator cuff are immense.
* Apply the plate laterally, sliding it under the axillary nerve if necessary. Secure the proximal fragment with multiple multi-planar locking screws into the humeral head, ensuring they do not penetrate the articular surface.
* Secure the distal shaft with a combination of non-locking (to pull the bone to the plate) and locking screws.
6. Adjunctive Procedures: Acromioplasty
Assess the subacromial space after the osteotomy is secured. If the greater tuberosity was severely malunited and residual subacromial impingement persists despite the correction of the shaft, perform an acromioplasty.
* Release the coracoacromial ligament.
* Use a motorized burr or osteotome to resect the anteroinferior aspect of the acromion, ensuring smooth, unhindered passage of the tuberosity during shoulder elevation.
COMPLEX HUMERAL MALUNIONS: DISTAL AND BIPOLAR CONSIDERATIONS
While this guide primarily addresses proximal third malunions, the orthopaedic surgeon must recognize that severe trauma can result in complex, multi-level, or distal humeral deformities that profoundly affect the entire upper extremity kinetic chain.
In cases where a humeral malunion extends distally or involves the elbow joint (e.g., severe cubitus varus or valgus), the surgical algorithm shifts significantly. Surgical treatment for these distal or complex deformities may consist of:
* Reconstruction of the lateral collateral ligament (LCL) combined with osteotomy.
* Ligament reconstruction alone.
* Osteotomy alone.
* Total elbow arthroplasty (TEA) in cases of advanced intra-articular destruction.
🔬 Evidence-Based Practice: Severe Distal Deformities
For a severe deformity (> 15 degrees) at the distal humerus coupled with high functional demands, O’Driscoll et al. strongly recommended corrective osteotomy combined with ligament reconstruction. This dual approach addresses both the bony architectural derangement and the secondary ligamentous insufficiency that inevitably develops on the convex side of the deformity.
POSTOPERATIVE CARE AND REHABILITATION
The postoperative protocol must balance the need for rigid immobilization to allow osteotomy consolidation with the imperative to initiate early motion to prevent adhesive capsulitis.
Immediate Postoperative Phase (Days 0 to 8)
- Immobilization: A shoulder abduction brace may be applied immediately postoperatively if needed to counteract severe muscle spasm and neutralize the deforming forces of the deltoid and rotator cuff.
- If intraoperative stability is deemed highly satisfactory (due to excellent bone quality and rigid locking plate fixation), a standard sling and swathe can be used instead.
- Early Motion: Codman (pendulum) range of motion exercises can be started between 2 and 8 days postoperatively, depending on patient comfort and wound healing.
Intermediate Phase (Weeks 2 to 6)
- Passive and active-assisted range of motion (AAROM) exercises are initiated under the guidance of a physiotherapist.
- Forward elevation in the scapular plane and gentle external rotation are prioritized.
- Protection with the abduction brace or a sling between exercise sessions is continued for 2 more weeks (up to 4-6 weeks total).
Late Phase (6 Weeks and Beyond)
- Active Range of Motion: Active range of motion (AROM) is allowed as clinical and radiographic fracture consolidation occurs, which is usually observed at 6 weeks postoperatively.
- Strengthening: Once the osteotomy is fully united (typically 8 to 12 weeks), progressive resistance exercises for the rotator cuff and periscapular stabilizers are initiated.
- Return to heavy manual labor or high-impact sports is generally restricted until 4 to 6 months postoperatively, contingent upon complete radiographic union and the restoration of near-normal shoulder strength.
COMPLICATIONS AND PITFALLS
- Nonunion or Delayed Union: The risk is elevated if excessive periosteal stripping occurs or if the osteotomy site lacks rigid compression. Treatment requires revision fixation, often supplemented with autologous bone grafting.
- Avascular Necrosis (AVN): Disruption of the ascending branch of the anterior circumflex humeral artery or extensive soft tissue dissection can lead to AVN of the humeral head. If symptomatic, this may eventually necessitate arthroplasty.
- Axillary Nerve Injury: Iatrogenic injury during the anterolateral approach or plate insertion can result in deltoid paralysis. Meticulous identification and protection of the nerve are non-negotiable.
- Hardware Penetration: Intra-articular penetration of proximal locking screws is a common complication. Thorough intraoperative fluoroscopic evaluation through a full range of motion is required to confirm that all screws are extra-articular.
CONCLUSION
The correction of a proximal third humeral malunion is a technically demanding procedure that requires a deep understanding of shoulder pathoanatomy. By adhering to strict preoperative templating, utilizing an anterolateral approach with minimal soft tissue disruption, executing a precise wedge osteotomy, and employing modern fixed-angle locking plate technology, the orthopaedic surgeon can reliably restore glenohumeral biomechanics. Coupled with a structured, evidence-based postoperative rehabilitation protocol, patients can achieve significant pain relief and a profound restoration of upper extremity function.
You Might Also Like