Comprehensive Management of Humeral Shaft Fractures: Operative and Nonoperative Strategies
Key Takeaway
Humeral shaft fractures account for approximately 3% of all fractures. While functional bracing remains the gold standard for nonoperative management, operative intervention is indicated for polytrauma, open fractures, and vascular injuries. Plate osteosynthesis is the preferred surgical method, offering high union rates and lower complication profiles compared to intramedullary nailing. This guide details the biomechanics, surgical approaches, and fixation techniques for optimal patient outcomes.
Introduction and Epidemiology
Fractures of the humeral shaft represent a significant portion of orthopedic trauma, accounting for approximately 3% of all fractures. The unique anatomical characteristics of the humerus, combined with the extensive compensatory range of motion provided by the adjacent shoulder and elbow joints, make it highly amenable to nonoperative management. As Sir John Charnley famously stated, “It is perhaps the easiest of the major long bones to treat by conservative methods.”
Because the upper extremity is not subjected to the weight-bearing demands of the lower extremity, the humerus exhibits a remarkable tolerance for radiographic imperfections. Small amounts of shortening, angulation, and rotation typically result in minimal functional deficit and are exceedingly well tolerated by the patient. However, the paradigm of treatment shifts dramatically in the presence of polytrauma, open injuries, or specific fracture patterns, necessitating a thorough understanding of both conservative and operative principles.
Nonoperative Management: The "Gold Standard"
Historically, conservative treatment modalities included skeletal traction, abduction casting, Velpeau dressings, and hanging arm casts. While each method has historical significance, functional bracing has essentially rendered them obsolete, emerging as the undisputed "gold standard" for nonoperative treatment.
Biomechanics of Functional Bracing
Initially popularized by Sarmiento in 1977, functional bracing relies on three core biomechanical principles:
1. The Hydraulic Effect: The rigid brace compresses the soft tissues (muscle and fascia) surrounding the fracture, creating a stabilizing hydrostatic column.
2. Active Muscle Contraction: Isometric and isotonic contractions of the biceps, triceps, and brachialis align the fracture fragments.
3. Gravity: The dependent position of the arm provides a continuous, mild traction force that restores length and corrects angulation.
Clinical Pearl: The use of a traditional sling is strongly discouraged during functional bracing, as it negates the beneficial effects of gravity and frequently leads to varus and internal rotation deformities.
Treatment Protocol and Acceptable Reduction
The standard protocol involves the initial application of a coaptation splint or hanging arm cast for the first 7 to 10 days. This allows acute swelling and pain to subside. Once the acute phase resolves, the patient is transitioned to a prefabricated functional brace.
Pendulum exercises are initiated early, and functional use of the extremity is encouraged as tolerated, though active shoulder abduction should be avoided until clinical stability is achieved. The brace is maintained until the patient is pain-free and radiographic union is evident. Union rates of 96% to 100% have been consistently reported, even in distal-third fractures.
Guidelines for Acceptable Radiographic Reduction:
* Shortening: Less than 3 cm
* Angulation: Less than 20 degrees (varus/valgus or apex anterior/posterior)
* Rotation: Less than 30 degrees
Skin maceration is a primary concern with functional bracing; therefore, meticulous daily hygiene must be stressed to the patient. While morbid obesity may increase the risk of varus deformities due to the fulcrum effect of the chest wall, these deformities are primarily cosmetic and rarely impair function.
Indications for Operative Treatment
The decision to proceed with operative intervention is multifactorial. McKee systematically categorized the indications for surgery into three distinct domains: Fracture Indications, Associated Injuries, and Patient Indications.
1. Fracture Indications
- Failure to obtain or maintain adequate closed reduction (exceeding acceptable parameters).
- Segmental fractures (high risk of nonunion due to disrupted endosteal blood supply).
- Pathological fractures (requiring stabilization and potential tumor management).
- Displaced intraarticular extension into the shoulder or elbow joints.
2. Associated Injuries
- Open wounds (requiring debridement and stabilization).
- Vascular injuries (requiring rigid skeletal fixation prior to or immediately following vascular repair).
- Brachial plexus injuries.
- "Floating elbow" (ipsilateral forearm fracture).
- Ipsilateral shoulder or elbow fractures.
- Bilateral humeral fractures (to allow for personal hygiene and independence).
- Lower extremity fractures requiring upper extremity weight-bearing (e.g., crutch use).
- High-velocity gunshot injuries or severe burns.
3. Patient Indications
- Polytrauma or multiple injuries (our most common indication for early mobilization).
- Severe head injury (Glasgow Coma Scale score ≤ 8) or chest trauma.
- Poor patient tolerance or compliance with bracing.
- Unfavorable body habitus (morbid obesity or large breasts precluding adequate brace fit).
Surgical Warning: While obesity and minimally displaced segmental fractures are relative indications, vascular injury, open fractures, and floating elbows are absolute indications for immediate surgical intervention.
Operative Treatment Modalities
The primary goal of operative treatment is to reestablish length, alignment, and rotation with stable fixation that permits early motion and, ideally, early weight-bearing on the fractured extremity. The three primary options are plate osteosynthesis, intramedullary (IM) nailing, and external fixation.
Plate Osteosynthesis: The Operative Gold Standard
Plate osteosynthesis remains the gold standard for the operative fixation of humeral shaft fractures. It provides superior biomechanical stability, allows for direct visualization and protection of the radial nerve, and produces minimal shoulder or elbow morbidity.
Extensive literature supports the efficacy of plating. Five large series (Foster, McKee, Vander Griend, Bell, and Tingstad) encompassing 361 fractures demonstrated an average union rate of 96.7%. Plating provides sufficient rigidity to allow early upper extremity weight-bearing, a critical factor for polytrauma patients.
Implant Choice and Construct Design
The workhorse implant for the humeral shaft is the broad, 4.5-mm limited-contact dynamic compression plate (LC-DCP). For patients with smaller osseous anatomy, a narrow 4.5-mm LC-DCP may be utilized.

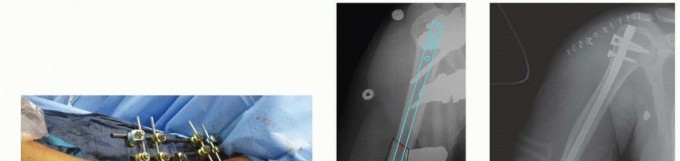
Fig. 54-28 Anterior plating of humeral shaft fracture with limited-contact dynamic compression plate.
For fractures located at the distal metaphyseal-diaphyseal transition zone, standard straight plates may not provide adequate distal purchase. In these scenarios, dual 3.5-mm LC-DCPs or anatomically pre-contoured extra-articular distal humerus plates are required.

Fig. 54-29 Dual plating of distal metaphyseal-diaphyseal humeral shaft fracture.
Construct Biomechanics based on Fracture Pattern:
* Spiral or Oblique Fractures: The ideal construct is absolute stability achieved via an interfragmentary lag screw protected by a neutralization plate. The Eglseder technique—attaining provisional reduction with a lag screw, Kirschner wire, or minifragment plate—allows direct observation of the reduction and simplifies the application of the definitive neutralization plate.


Fig. 54-30 A, Oblique humeral shaft fracture. B, After provisional reduction with lag screw and fixation with plate and screws.
- Transverse Fractures: These are ideally suited for dynamic compression plating to achieve primary bone healing.
- Comminuted Fractures: A bridge plating technique is employed to achieve relative stability. Anatomical reduction of every butterfly fragment is unnecessary and often detrimental. The goal is to restore length, alignment, and rotation while preserving the soft-tissue envelope and periosteal blood supply.


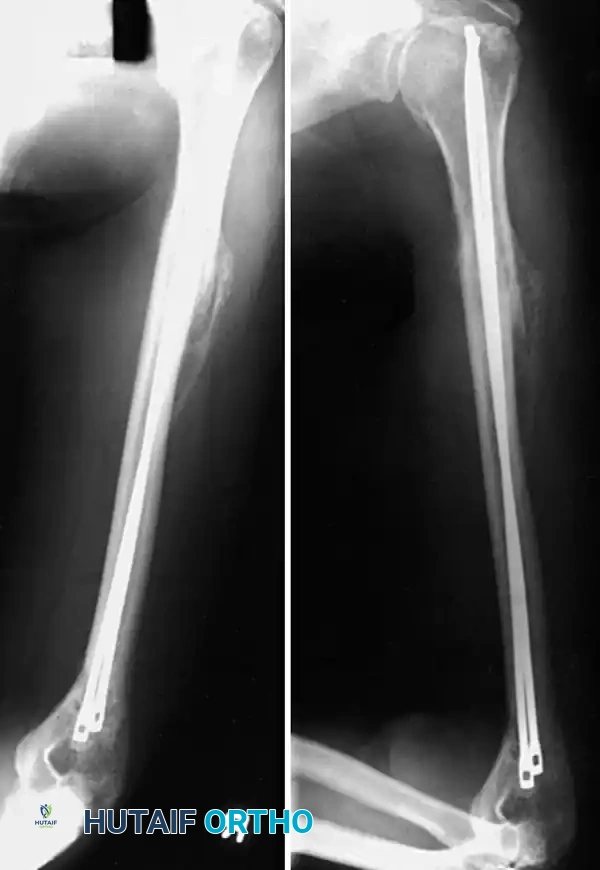
Fig. 54-31 A, Segmental shaft fracture with extension into proximal humerus. B and C, Long plate used to obtain secure fixation.
Biomechanical Principle: Generally, a minimum of eight cortices (four bicortical screws) above and below the fracture are necessary to prevent screw pullout. In osteoporotic bone, longer plates spanning a greater working length, locking screws, or methylmethacrylate augmentation may be required.
Minimally Invasive Plate Osteosynthesis (MIPO)
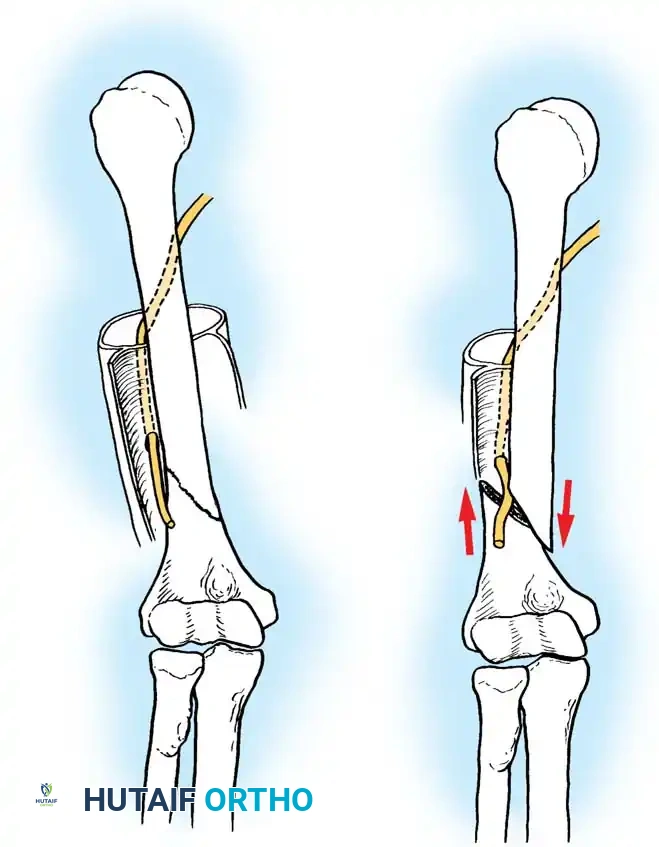
While MIPO has gained traction in lower extremity trauma, its application in the humerus is tempered by the risk of iatrogenic radial nerve injury. Cadaveric studies by Apivatthakakul et al. demonstrated that the plate sits an average of 3.2 mm from the radial nerve. Pronation of the forearm moves the nerve even closer (by 3 mm). Due to these risks, MIPO should be reserved for highly experienced surgeons.

Intramedullary Nailing vs. Plating
While intramedullary (IM) nailing is the standard of care for femoral and tibial shaft fractures, its role in the humerus is more controversial.
A prospective, randomized trial by McCormack et al. comparing plate fixation (23 patients) to IM nailing (21 patients) found no significant differences in overall elbow/shoulder function. However, shoulder impingement occurred in six nailing patients versus only one plating patient, and seven nailing patients required a secondary operation compared to one in the plating group.
Similarly, Flinkkilä et al. and a meta-analysis by Bhandari et al. confirmed that reoperation rates and shoulder impingement are significantly higher following antegrade IM nailing. Consequently, IM nailing is generally reserved for specific indications:
* Pathological fractures (prophylactic or therapeutic).
* Segmental fractures where extensive soft-tissue stripping for a plate is undesirable.
* Severe osteopenia where screw purchase is compromised.


External Fixation
External fixation is rarely used as definitive management. It is strictly reserved for damage-control orthopedics, high-energy gunshot wounds, massive soft-tissue defects, or gross contamination where internal hardware would pose an unacceptable risk of deep infection.

Surgical Approaches to the Humeral Shaft
The choice of surgical approach is dictated by the fracture location and the planned construct.
Anterolateral Approach (Brachialis-Splitting)
Ideal for fractures of the proximal and middle thirds of the humeral shaft. The internervous plane lies proximally between the deltoid (axillary nerve) and pectoralis major (medial/lateral pectoral nerves), and distally it splits the brachialis muscle. The lateral half of the brachialis is innervated by the radial nerve, and the medial half by the musculocutaneous nerve, making this a safe, denervation-free split.
Posterior Approaches
Ideal for midshaft fractures and those extending into the distal third.
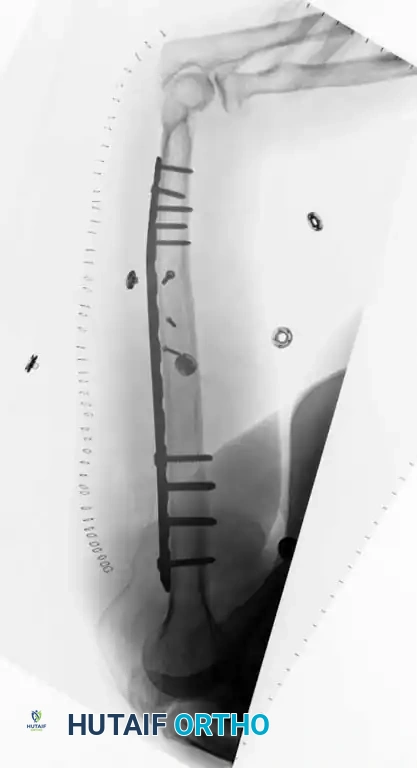

Fig. 54-32 A, Fracture of distal third of humeral shaft. B, After plate fixation through posterior triceps-splitting approach.
The traditional triceps-splitting approach provides excellent access but can limit distal visualization. To overcome this, Gerwin, Hotchkiss, and Weiland described a modified posterior approach (triceps-reflecting). By reflecting the triceps medially off the lateral intermuscular septum, this approach exposes an average of 10 cm more of the humeral shaft than the standard split, providing unparalleled access to the radial nerve and the posterior humerus.


Step-by-Step Surgical Technique: Modified Posterior Approach (Triceps-Reflecting) [TECHNIQUE 54-6]
This approach is highly favored for complex mid-to-distal third fractures requiring extensive plating.
1. Positioning and Preparation:
* Place the patient in the lateral decubitus position with the operative arm draped over a padded post.
* Ensure a wide proximal preparation and drape to allow for the application of a sterile tourniquet if necessary.
2. Incision:
* Make a longitudinal incision starting from the level of the tourniquet, extending distally to the tip of the olecranon, perfectly in line with the posterior axis of the humerus.
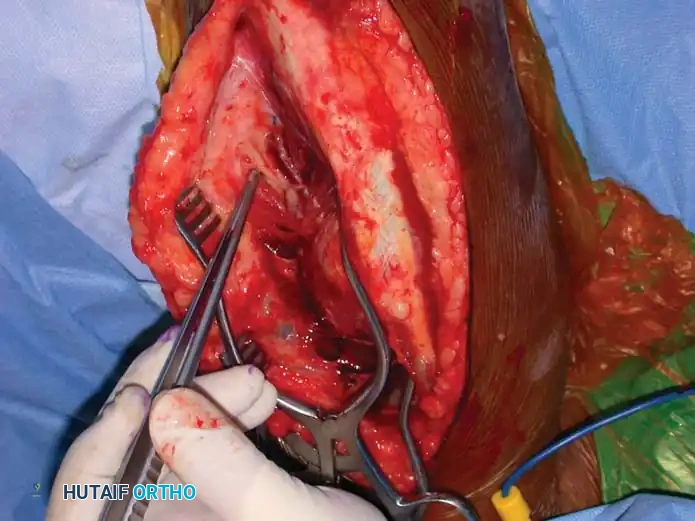
Fig. 54-33 A, Incision for the modified posterior approach.
3. Superficial Dissection:
* Carry the dissection sharply down through the subcutaneous tissue to identify the triceps fascia.
* Incise the fascia longitudinally. Carry the fascial dissection laterally to identify the lateral intermuscular septum.
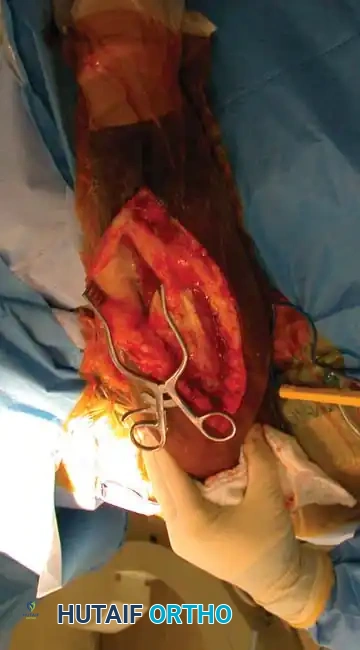
Fig. 54-33 B, Incision of fascia to expose the intramuscular septum.
4. Nerve Identification:
* Carefully identify and protect the lateral brachial cutaneous nerve, which serves as a reliable guide to the radial nerve.
Fig. 54-33 C, Identification of the lateral brachial cutaneous nerve.
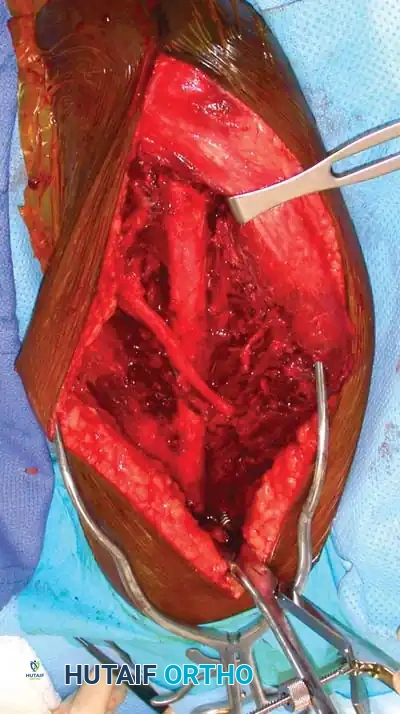
5. Deep Dissection and Radial Nerve Mobilization:
* Elevate the lateral head of the triceps off the lateral intermuscular septum.
* Identify the radial nerve and the profunda brachii artery as they pierce the lateral intermuscular septum to enter the anterior compartment.
* Carefully mobilize the radial nerve. Use vessel loops for gentle retraction. Never apply excessive traction to the nerve.
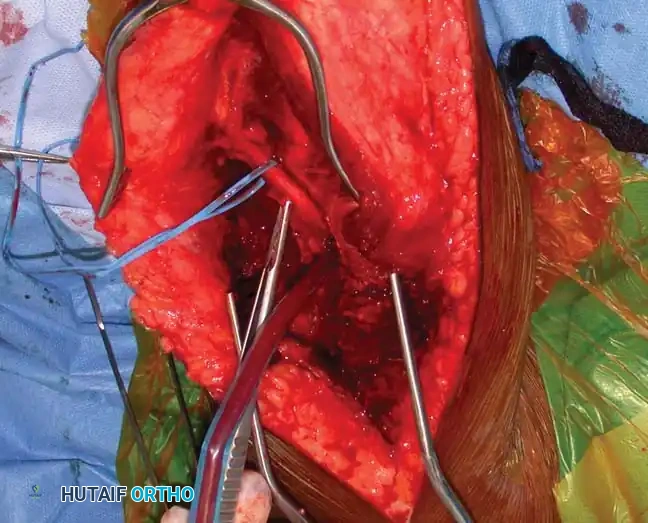
Fig. 54-33 D, Mobilization of the radial nerve.
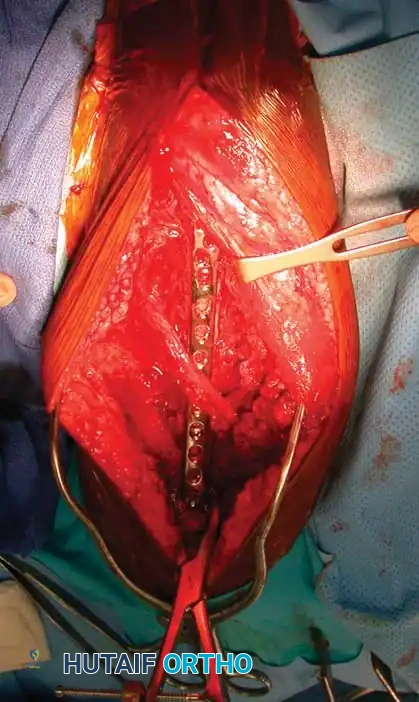
6. Fracture Reduction and Fixation:
* Reflect the entire triceps muscle mass medially to expose the posterior humeral shaft.
* Reduce the fracture and apply the pre-selected LC-DCP. Ensure the radial nerve is completely free and not tethered beneath the plate.


📚 Medical References
You Might Also Like