Management of Open Wounds and Penetrating Injuries of the Knee Joint
Key Takeaway
Open wounds of the knee joint, particularly from civilian gunshot injuries, require immediate and systematic evaluation. Management hinges on ruling out neurovascular compromise, confirming intra-articular penetration via saline load testing or aspiration, and executing meticulous surgical debridement. Arthroscopic irrigation is increasingly preferred over open arthrotomy for low-velocity injuries without complex fractures, offering superior visualization of occult osteochondral fragments and foreign debris while minimizing postoperative morbidity.
INTRODUCTION TO OPEN KNEE JOINT INJURIES
Although the management of war-related open joint injuries has been reviewed extensively in trauma literature, the treatment of open joint wounds in the civilian population requires distinct, evidence-based protocols. As the incidence of civilian gunshot injuries has increased globally, gunshot wounds (GSWs) to the knee have become markedly more common. Of all open joint injuries, those involving the knee are by far the most prevalent, accounting for 53% to 91% of all cases.
The knee’s superficial anatomical location, combined with its expansive synovial capsule (which extends proximally into the suprapatellar pouch and posteriorly into the popliteal region), makes it highly susceptible to penetrating trauma. The primary goals of managing open knee wounds are the prevention of septic arthritis, the restoration of articular congruity, the stabilization of associated fractures, and the early return of functional range of motion (ROM).
INITIAL EVALUATION AND RESUSCITATION
The initial management of a patient with an open wound to the knee must follow standard Advanced Trauma Life Support (ATLS) protocols. Life-threatening injuries must be addressed before focusing on the extremity.
Neurovascular Assessment
Based on their extensive experience with 64 patients sustaining gunshot wounds to the knee, Perry et al. emphasized that the evaluation of a patient’s neurovascular status is of paramount importance. The popliteal artery and vein, along with the common peroneal and tibial nerves, are intimately associated with the posterior aspect of the knee joint.
Clinical Pearl: A penetrating injury traversing the popliteal fossa or presenting with an expanding hematoma, absent distal pulses, or an ankle-brachial index (ABI) less than 0.9 mandates immediate vascular evaluation. If hard signs of ischemia are present, immediate surgical exploration is required. If vascular repair is performed, a prophylactic surgical fasciotomy of the leg compartments should be strongly considered to prevent compartment syndrome.
Joint Penetration Assessment
If intra-articular fractures are not immediately evident on radiographs, determining whether the joint capsule has been violated is the next critical step.
* Knee Joint Aspiration: Aspiration of the knee joint can help determine if the joint has been penetrated. A grossly bloody aspirate (hemarthrosis) with fat globules (lipohemarthrosis) strongly indicates capsular penetration and occult fracture, dictating the need for formal joint irrigation.
* Saline Load Test: If aspiration is equivocal, a saline load test should be performed. This involves injecting 120 to 155 mL of sterile normal saline (often mixed with methylene blue) into the joint via a suprapatellar approach. Extravasation of fluid from the traumatic wound confirms joint violation.
DIAGNOSTIC IMAGING
Once neurovascular injuries have been identified and treated, skeletal injuries must be meticulously evaluated.
- Radiographs: High-quality anteroposterior (AP), lateral, and oblique radiographs are carefully scrutinized for fracture lines, intra-articular air (pneumarthrosis), bullet fragments, and osteochondral fragments.
- Computed Tomography (CT): CT scanning provides invaluable, high-resolution information regarding the extent and complexity of the fracture pattern, the exact trajectory of the missile, and the presence of occult intra-articular debris. CT is highly recommended for any periarticular gunshot wound to map out surgical approaches and fixation strategies.
ANTIBIOTIC PROPHYLAXIS AND TETANUS
The cornerstone of preventing septic arthritis in open knee injuries is the prompt administration of systemic antibiotics and tetanus prophylaxis.
Patzakis et al. reviewed 140 patients with penetrating joint injuries treated over a 4-year period, dividing them into three categories: open joint injuries with fractures, open joint injuries without fractures, and gunshot wounds. Their protocol of early antibiotics, surgical debridement, and irrigation yielded remarkably good results, with an overall infection rate of only 2.1% (3 out of 140 patients).
Based on current evidence and the recommendations of Perry et al., the following antibiotic protocols are standard:
* Non-Operative Wounds (Superficial/No Joint Violation): Ceftriaxone (one 1-g dose) or a first-generation cephalosporin.
* Severe Injuries / Joint Violation: Cefazolin (1 to 2 g) and Gentamicin (80 mg) administered every 8 hours until surgery. This regimen is continued postoperatively for up to 48 hours.
* Post-Culture Adjustment: Once intraoperative culture reports and sensitivities are obtained, antibiotic dosages and agents are adjusted accordingly.
TREATMENT ALGORITHM FOR GUNSHOT WOUNDS TO THE KNEE
Perry et al. designed a comprehensive treatment protocol for the management of neurovascular injuries, soft-tissue wounds, and fractures occurring with gunshot wounds to the knee. The algorithm dictates a logical progression from life- and limb-saving vascular assessment to joint debridement and definitive fracture care.
SURGICAL MANAGEMENT: ARTHROSCOPIC VS. OPEN DEBRIDEMENT
If the joint is violated, surgical debridement and irrigation are mandatory. The choice between arthroscopic and open arthrotomy depends on the severity of the soft-tissue injury, the presence of complex fractures requiring open reduction, and the degree of contamination.
Arthroscopic Debridement and Irrigation
For low-velocity gunshot wounds and penetrating injuries without complex, unstable fractures, arthroscopic debridement has become the gold standard.
Advantages of Arthroscopy:
Raskind and Marder compared the results of arthroscopic examination and debridement (14 patients) with those of open debridement (16 patients) in penetrating knee joint injuries. While neither group developed infections, the arthroscopic group demonstrated:
* Shorter postoperative hospital stays.
* Significantly less postoperative pain.
* Superior cosmetic results.
* Enhanced identification of occult intra-articular injuries.
Furthermore, Berg and Ciullo noted that the degree of joint contamination detected during arthroscopic debridement greatly exceeded that indicated by clinical and radiographic examinations. They successfully debrided denim, hair, skin, and osteochondral fragments from the knee joints of patients. They concluded that arthroscopy is a highly effective component of surgical debridement, especially when a bullet has passed through clothing before entering the joint. Parisien and Esformes also reported excellent functional outcomes following arthroscopic treatment of low-velocity GSWs.
Arthroscopic Technique:
1. Positioning: The patient is placed supine. A tourniquet is applied to the proximal thigh but is generally not inflated unless visualization is severely compromised by bleeding, as maintaining perfusion assessment is critical.
2. Portals: Standard anterolateral and anteromedial portals are established. If the traumatic wound is appropriately located, it may be incorporated into a portal or excised during closure.
3. Diagnostic Sweep: A systematic 6-point diagnostic sweep is performed (suprapatellar pouch, medial gutter, medial compartment, intercondylar notch, lateral compartment, lateral gutter).
4. Debridement: All foreign material (clothing, bullet fragments, hair) and devitalized tissue are removed using motorized shavers and graspers.
5. Irrigation: Copious irrigation with a minimum of 6 to 9 liters of sterile normal saline is utilized to mechanically wash out microscopic debris and bacteria.
6. Fragment Management: Small, unfixable osteochondral fragments are excised. Large, viable osteochondral fragments can be reattached and fixed using arthroscopic techniques (e.g., headless compression screws or bioabsorbable pins).
Open Arthrotomy and Debridement
In cases of high-velocity injuries, shotgun blasts, severe gross contamination, or when complex intra-articular fractures require open reduction and internal fixation (ORIF), an open arthrotomy is indicated. Ashby’s review of low-velocity GSWs also supported open surgical debridement when occult osteochondral fragments could not be managed minimally invasively.
Surgical Technique & Pitfalls:
1. Approach: A standard medial or lateral parapatellar arthrotomy is typically utilized, allowing extensile exposure of the articular surfaces.
2. Debridement: Meticulous excision of all necrotic skin, subcutaneous tissue, fascia, and muscle is performed. The "rule of 4 Cs" (Color, Consistency, Contractility, Circulation) must be applied to muscle viability.
3. Irrigation: High-volume, low-pressure pulsatile lavage is employed.
Surgical Warning - The Danger of Closed Suction Drains:
In their landmark review, Patzakis et al. initially utilized polyethylene tubes for closed irrigation and suction. While their overall infection rate was low, they noted that several patients developed positive cultures from the drainage tubes postoperatively, despite having negative cultures at the time of initial surgery. They concluded that the closed irrigation and suction system itself acted as a conduit for retrograde contamination. Therefore, closed irrigation and suction should NOT be used routinely for open joint injuries. It is reserved strictly for cases with initial severe, massive contamination or extensive soft-tissue stripping where dead-space management is critical.
FRACTURE AND SOFT-TISSUE MANAGEMENT
Fracture management is dictated by the stability of the fracture pattern, the degree of comminution, and the condition of the soft-tissue envelope.
- Stable Fracture Patterns (or Unicortical Defects): May be managed non-operatively with prophylactic hinged knee bracing and early ROM.
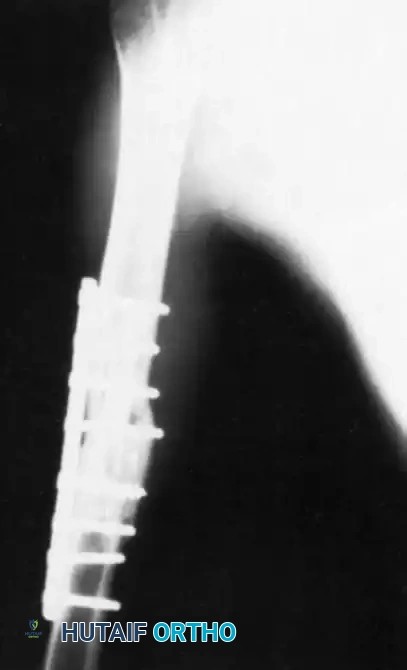
- Unstable Intra-articular Fractures: Require anatomical reduction and stable fixation. Depending on soft-tissue viability, this may involve immediate ORIF with locking plates and screws, or temporary spanning external fixation if the soft tissues are too compromised to tolerate immediate internal hardware.
- Massive Soft-Tissue Defects: Large soft-tissue avulsions or necrosis from high-velocity blasts may require delayed primary closure, negative pressure wound therapy (NPWT), or coverage via local rotational flaps (e.g., gastrocnemius flap) or free tissue transfer.
- Ligamentous/Tendinous Injury: Damaged musculotendinous units (e.g., patellar tendon, quadriceps tendon) or collateral ligaments should be repaired or reconstructed as soon as the wound is deemed clean and stable to restore joint kinematics and function.
POSTOPERATIVE PROTOCOL AND REHABILITATION
The postoperative rehabilitation protocol must be individualized based on the stability of the fracture fixation and the integrity of the extensor mechanism.
- Early Range of Motion (ROM): If no fracture is present, or if the fracture is rigidly fixed, early continuous passive motion (CPM) and active-assisted ROM are initiated within 24 to 48 hours to prevent arthrofibrosis and promote cartilage nutrition.
- Weight-Bearing Status:
- No fracture / Stable unicortical defect: Weight-bearing as tolerated (WBAT) in a hinged brace.
- Operatively fixed intra-articular fractures: Strictly non-weight-bearing (NWB) or touch-down weight-bearing (TDWB) for 8 to 12 weeks, depending on radiographic evidence of callus formation.
- Monitoring: Patients must be closely monitored for signs of septic arthritis (increasing effusion, erythema, disproportionate pain, fever) or compartment syndrome in the immediate postoperative period. Serial inflammatory markers (CRP, ESR) may be tracked if clinical suspicion of infection arises.
You Might Also Like