Operative Management of Hip Dislocations and Fracture-Dislocations
Key Takeaway
Hip dislocations and fracture-dislocations are high-energy orthopedic emergencies requiring prompt reduction to minimize the risk of avascular necrosis. This comprehensive guide details the biomechanics, Thompson and Epstein classification, closed reduction maneuvers—including the Allis and Stimson techniques—and indications for open reduction. Mastering these evidence-based protocols is essential for orthopedic surgeons to restore joint congruity, manage associated sciatic nerve injuries, and optimize long-term patient outcomes.
Introduction to Hip Joint Trauma
Injuries of the hip joint encompass a spectrum of severe trauma, including pure hip dislocations, dislocations with associated fractures of the femoral head, and dislocations complicated by fractures of the acetabulum. The precise position of the femoral head in relation to the acetabulum, combined with the vector of the force at the exact moment of impact, dictates the specific pattern of injury produced.
Because of the profound intrinsic stability of the hip joint—afforded by the massive bony columns of the pelvis, the robust acetabular labrum, and the thick iliofemoral ligaments—exceedingly high energy is usually required to produce these injuries. Consequently, hip joint injuries are rarely isolated; they are frequently complicated by concomitant injuries to other organ systems or the pelvic ring, which can precipitate catastrophic hemorrhage and hemodynamic shock.
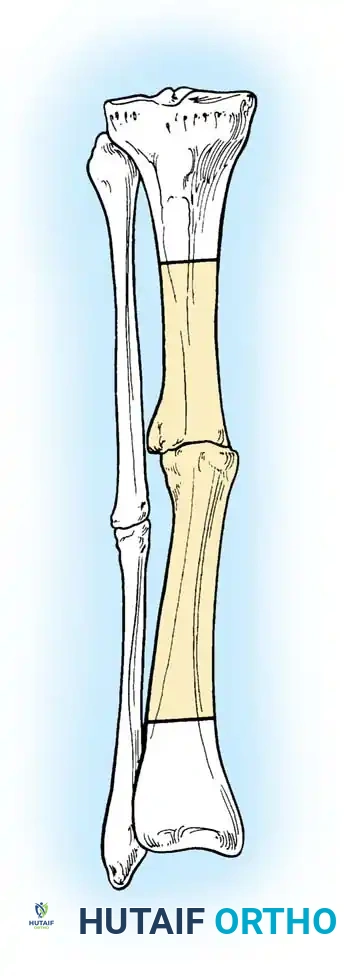
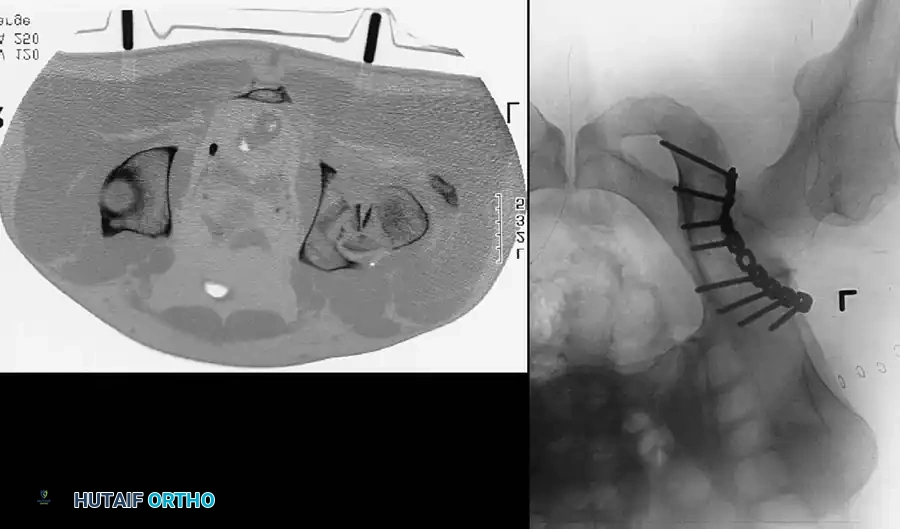
Fig. 52-44 A, Initially nondisplaced, unrecognized femoral fracture that displaced after closed intramedullary nailing of associated femoral shaft fracture. B, After closed reduction and fixation of femoral neck fracture with cannulated screws placed anterior to the femoral nail.
Displacement of the femoral head or the acetabular columns poses an immediate threat to the sciatic, femoral, or obturator nerves. Furthermore, associated injuries to the ipsilateral knee are highly prevalent. The classic "dashboard injury" frequently results in patellar fractures, open knee lacerations, and severe ligamentous disruption. Rupture of the posterior cruciate ligament (PCL) can be particularly difficult to diagnose acutely due to guarding and the impossibility of performing a reliable initial knee examination while the hip remains dislocated.
Surgical Warning: Hip dislocations are absolute orthopaedic emergencies. The dislocation must be reduced as expeditiously as possible to restore perfusion to the femoral head via the retinacular vessels. Closed reduction of the hip takes strict precedence over the definitive treatment of almost all other skeletal injuries.
Late complications of these injuries are devastating and include osteonecrosis (avascular necrosis) of the femoral head and rapidly progressive posttraumatic osteoarthritis.
Biomechanics and Mechanism of Injury
Posterior dislocations are by far the most common type of hip dislocation. Patients typically present with a clinically obvious deformity: a shortened, internally rotated, and adducted lower extremity held in slight flexion. However, this classic posture can be altered if the femoral head becomes impaled on a fractured posterior acetabular wall.
The injury typically results from a massive longitudinally directed force applied through the femoral shaft to a flexed hip. This is the hallmark of an automobile head-on collision where the patient’s knee strikes the dashboard.
* Pure Dislocation: If the hip is in a state of adduction at the time of impact, the femoral head is driven directly out of the posterior capsule, resulting in a pure dislocation.
* Fracture-Dislocation: If the hip is in a neutral position or slight abduction, the femoral head is driven into the posterior rim of the acetabulum, leading to a dislocation associated with a fracture of the posterior acetabular wall or the femoral head itself.
Classification Systems
Traditionally, this injury complex has been categorized based on the direction of the dislocation (posterior, anterior, obturator, or central). True central fracture-dislocations are exceedingly rare, occasionally seen in patients with severe metabolic bone disease where the femoral head breaches the medial wall of the acetabulum without disrupting the anterior or posterior columns. More commonly, what appears as a central fracture-dislocation is actually a transverse or both-column acetabular fracture, best described by the Letournel and Judet classification.
Thompson and Epstein Classification
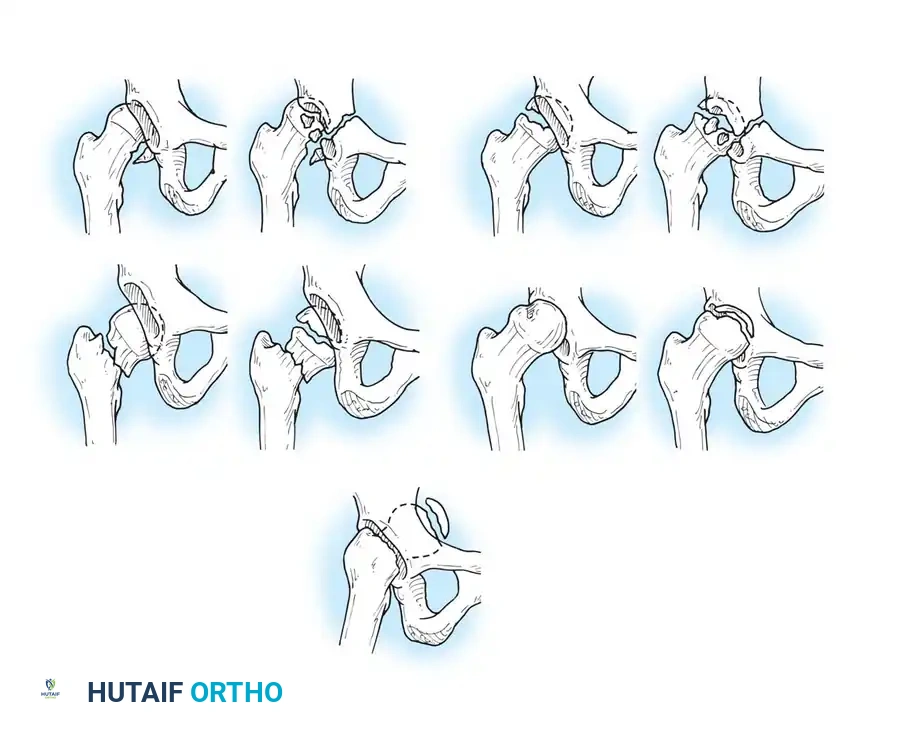
For posterior dislocations, the Thompson and Epstein classification remains a foundational framework, dividing these injuries into five distinct types:
- Type I: Dislocation with or without a minor fracture.
- Type II: Dislocation with a large single fracture of the posterior acetabular rim.
- Type III: Dislocation with comminution of the posterior acetabular rim, with or without a major fragment.
- Type IV: Dislocation with fracture of the acetabular floor.
- Type V: Dislocation with fracture of the femoral head.
Diagrammatic representation of various hip fracture-dislocation patterns highlighting the relationship between the femoral head and acetabular rim.
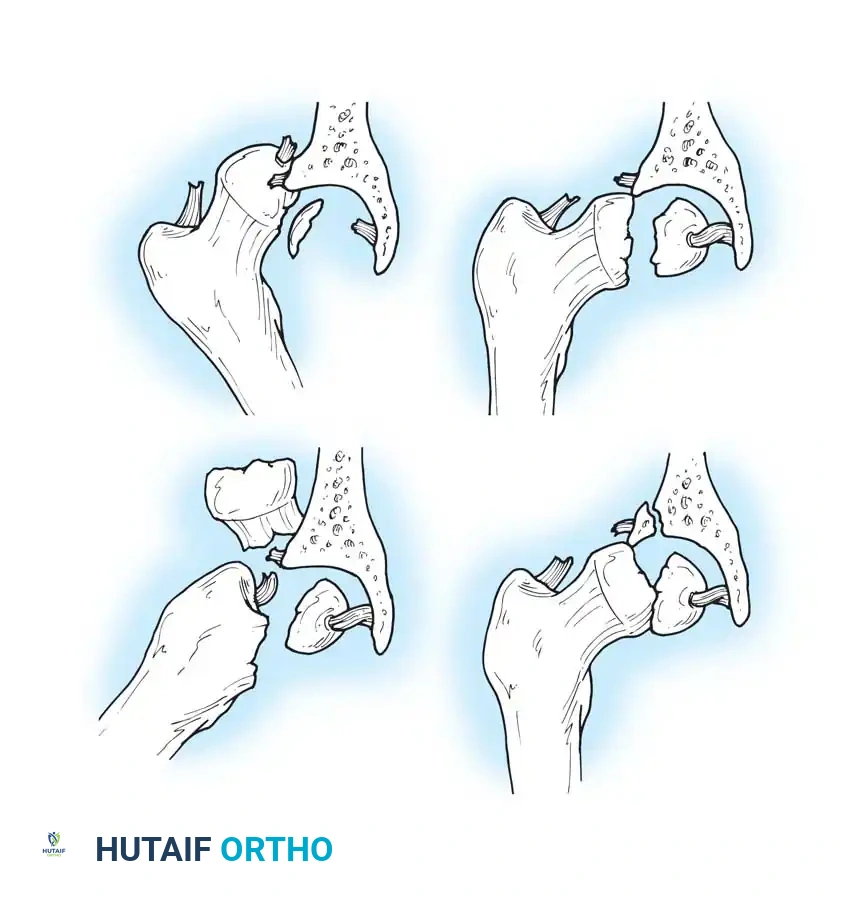
Further classification of femoral head fractures associated with posterior hip dislocations, emphasizing the location of the fracture relative to the fovea capitis.
While this classification system was formulated before the widespread advent of Computed Tomography (CT), it remains conceptually vital. Historically, Thompson and Epstein recommended routine open reduction for all fracture-dislocations to clear retained fragments. Today, high-resolution CT allows for precise preoperative identification of retained osteocartilaginous fragments, guiding the decision between closed management and operative intervention.
Principles of Initial Management
Regardless of the specific type of dislocation, several immutable guidelines govern the management of hip dislocations:
- Severity Dictates Outcome: Long-term functional results are directly proportional to the severity of the initial cartilaginous and bony trauma.
- Time is Cartilage: Reduction (whether open or closed) must be performed emergently, ideally within 6 hours, and absolutely within 12 hours to minimize the risk of osteonecrosis.
- Limit Attempts: Only one or two meticulous attempts at closed reduction should be made under adequate sedation and muscle relaxation. Repeated forceful attempts cause catastrophic iatrogenic damage to the femoral head cartilage and remaining vascular supply. If closed reduction fails, emergent open reduction is mandatory.
Neurological Evaluation
Before any reduction attempt, the patient must be carefully examined for sciatic nerve injury. A complete or partial sciatic nerve palsy occurs in approximately 10% to 15% of patients with posterior dislocations. The peroneal division is most frequently affected due to its lateral and superficial position within the sciatic nerve bundle. The mechanism of injury may involve direct trauma from the dislocating femoral head, laceration by sharp bone fragments, or ischemia from sustained compression. Sciatic nerve function must be meticulously documented both before and immediately after reduction.
Closed Reduction Techniques
Most Type I posterior dislocations can be treated by closed reduction in the emergency department. This requires deep intravenous sedation, profound muscle relaxation, and continuous hemodynamic monitoring.
The Allis Maneuver
The Allis maneuver is the most commonly utilized technique due to its safety and efficacy in the supine patient.
- The patient is positioned supine. An assistant firmly stabilizes the pelvis by applying downward pressure on both anterior superior iliac spines.
- The surgeon applies steady, inline longitudinal traction in the direction of the deformity.
- While maintaining traction, the surgeon slowly flexes the patient's hip and knee to 90 degrees.
- Gentle internal and external rotation of the hip is applied to clear the posterior acetabular lip until a palpable "clunk" indicates concentric reduction.
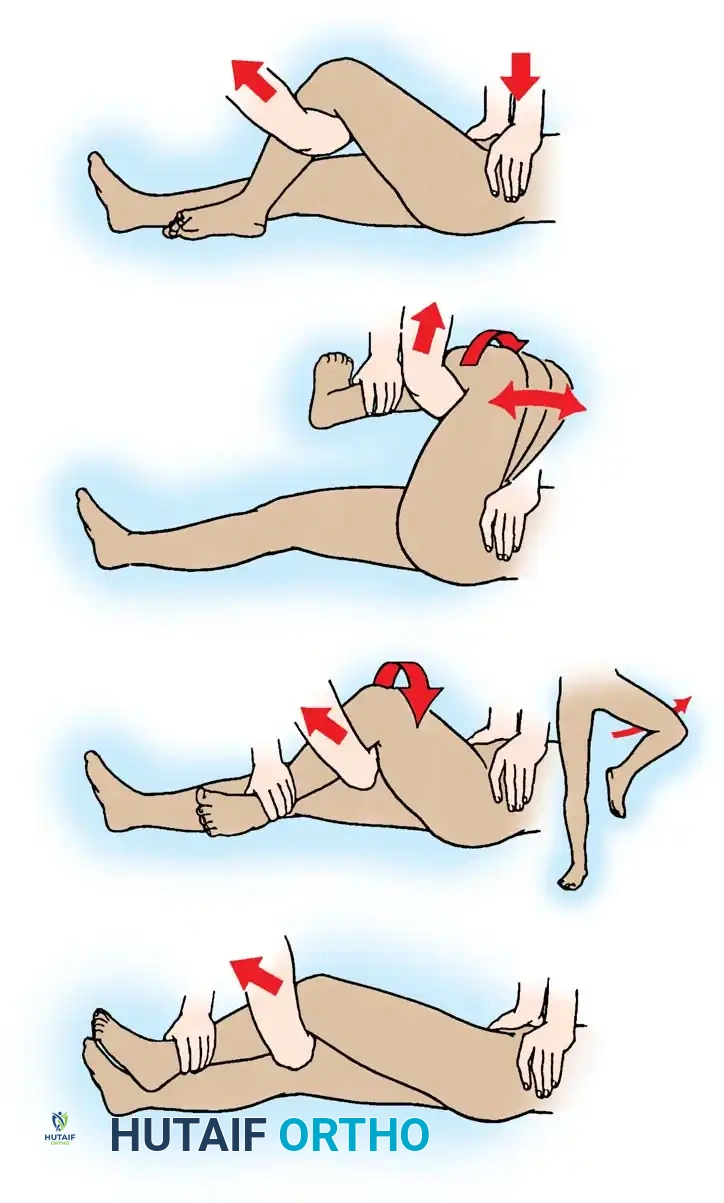
Fig. 52-48 (Part 1) Allis reduction maneuver for posterior dislocation of the hip. Initial inline traction and flexion.
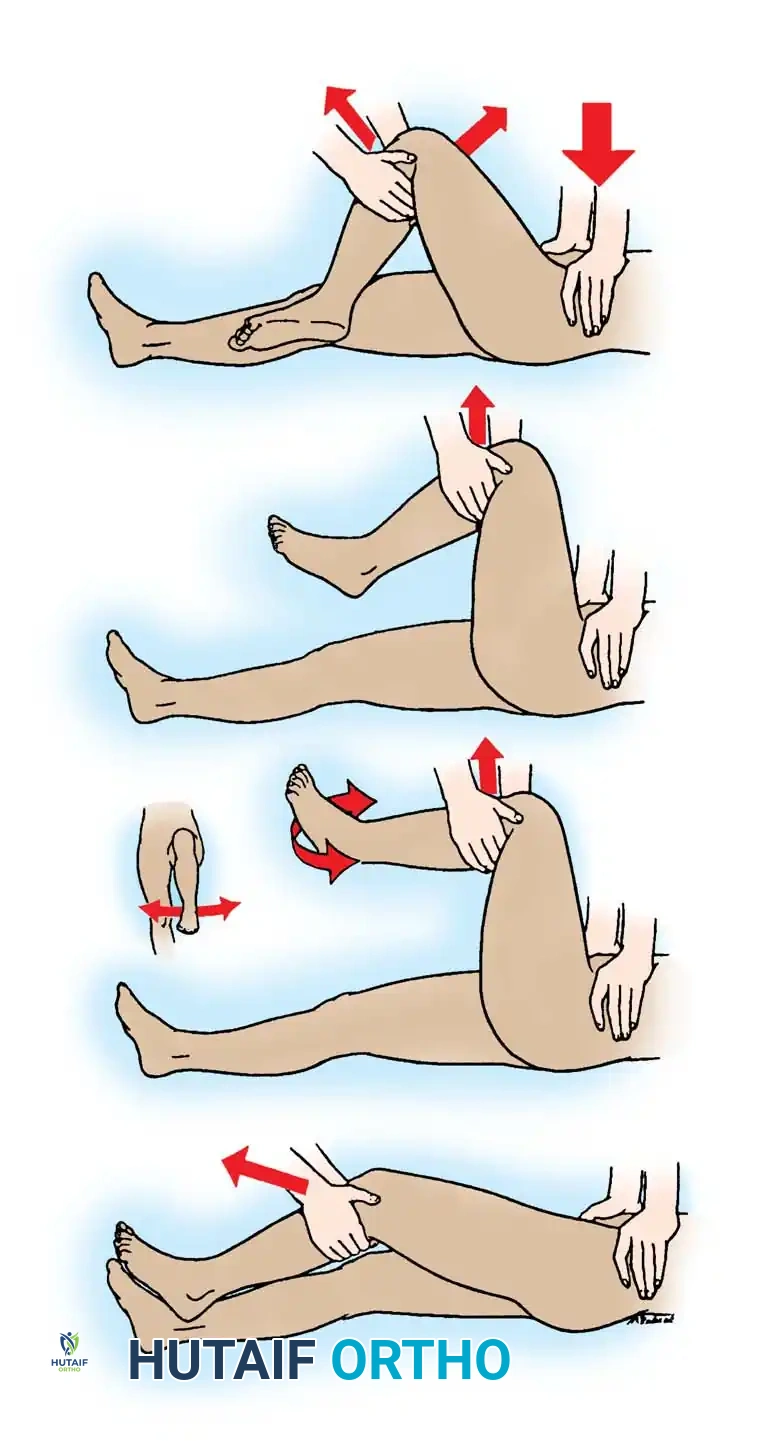
Fig. 52-48 (Part 2) Allis reduction maneuver. Application of rotational forces to lever the femoral head into the acetabulum.
The Gravity Method of Stimson
The Stimson method is highly effective and minimally traumatic but requires the patient to be prone, which is often contraindicated in polytrauma patients with spine or thoracic injuries.
- The patient is placed prone on a stretcher with the affected lower extremity hanging off the edge.
- An assistant stabilizes the pelvis.
- The hip and knee are flexed to 90 degrees. The surgeon grasps the proximal calf and applies a steady, downward longitudinal force.
- Gentle rotation aids in guiding the head back into the acetabulum.
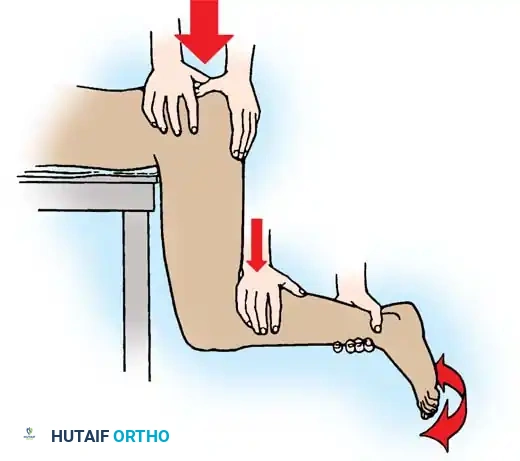
Fig. 52-47 Stimson maneuver for reduction of hip dislocation. The gravity-assisted downward force minimizes iatrogenic cartilage damage.
The Bigelow Maneuver
The Bigelow maneuver utilizes the intact iliofemoral ligament as a fulcrum. It is more complex and carries a slightly higher risk of iatrogenic femoral neck fracture if performed forcefully.
- With the patient supine and pelvis stabilized, the surgeon grasps the ankle and places their opposite forearm beneath the flexed knee.
- Longitudinal traction is applied, followed by flexion of the hip to 90 degrees in an adducted, internally rotated position.
- The femoral head is levered into the acetabulum through a sweeping motion of abduction, external rotation, and extension.
Fig. 52-49 Bigelow reduction maneuver for posterior dislocation of the hip, demonstrating the sweeping arc of reduction.
The East Baltimore Lift
This technique is excellent for minimizing surgeon fatigue and back strain, utilizing the combined strength of two providers.
- The patient is supine. The surgeon and an assistant stand on opposite sides of the affected limb.
- The patient’s hip and knee are flexed to 90 degrees.
- Both providers place their arms under the patient's proximal calf, resting their hands on each other's shoulders.
- By simultaneously standing up from a squatted position, they apply powerful, controlled upward traction while a second assistant stabilizes the pelvis.

Fig. 52-50 East Baltimore Lift. A highly effective, ergonomically safe method for reduction of posterior hip dislocations.
Post-Reduction Evaluation and Imaging
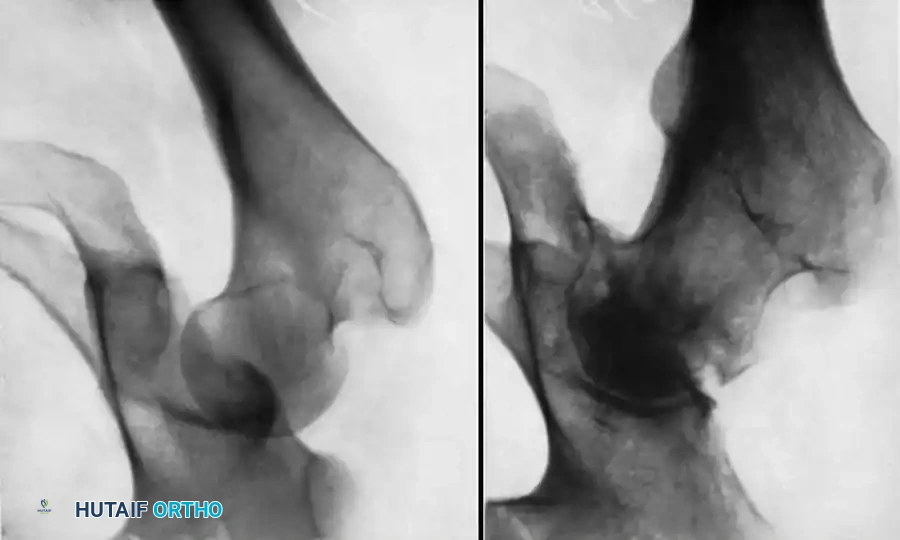
Immediately following closed reduction, a repeat anteroposterior (AP) pelvic radiograph is mandatory to confirm concentric reduction.
Clinical Pearl: Nonconcentric reduction is a subtle but critical finding. It is radiographically identified by a persistent widening of the medial joint space—specifically, the distance between the radiographic teardrop and the femoral head—when compared to the contralateral normal hip.
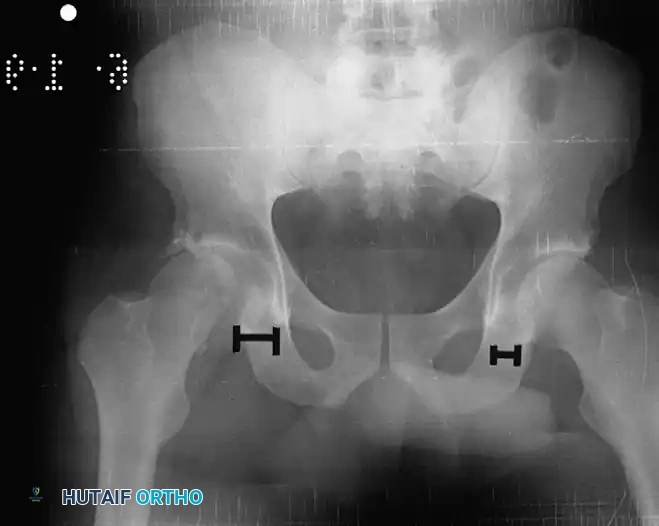
Fig. 52-45 Widening of the medial joint space after closed reduction indicates a nonconcentric reduction, highly suspicious for entrapped osteocartilaginous fragments or labrum.
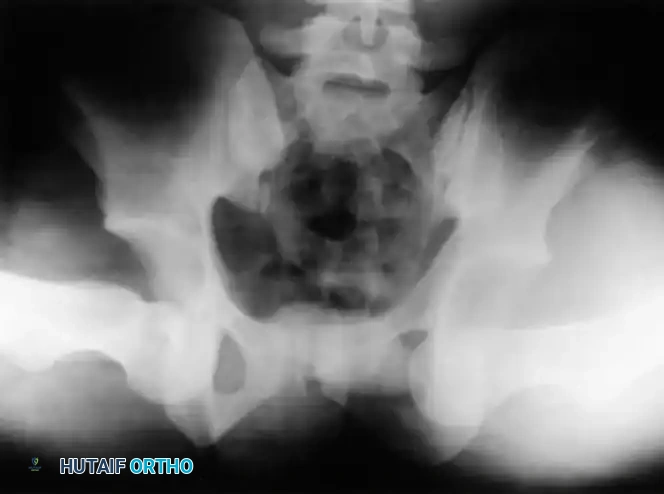
If the reduction is concentric, the patient must undergo a high-resolution CT scan of the pelvis with thin (2-3 mm) axial, coronal, and sagittal reformats. CT is vastly superior to plain radiography for identifying intra-articular fragments, subtle acetabular wall fractures, and femoral head impaction injuries.
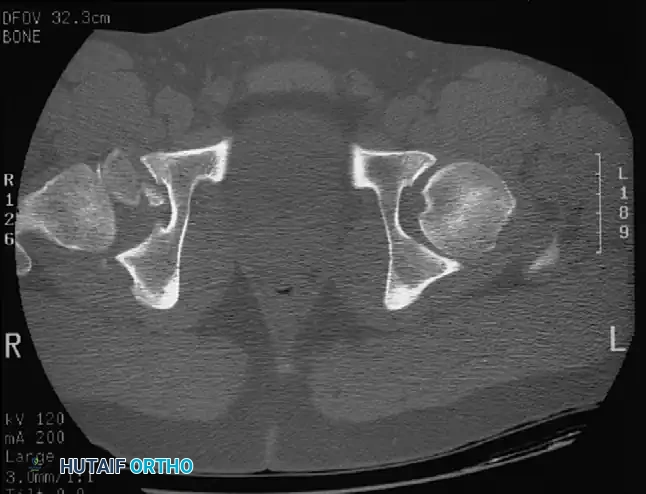
Fig. 52-46 Axial CT scan clearly demonstrating a retained osteochondral fragment interposed between the femoral head and the acetabular dome. Operative excision is strictly indicated.
CT scan of the pelvis providing detailed visualization of the posterior wall comminution and the relationship of the femoral head to the acetabular columns.
Indications for Open Reduction
Operative intervention is indicated under the following circumstances:
1. Irreducible Dislocation: Failure of 1-2 closed attempts. Obstructions may include buttonholing of the femoral head through the posterior capsule, interposition of the piriformis or obturator internus muscles, or a torn acetabular labrum blocking the joint space.
2. Nonconcentric Reduction: Evidence of retained intra-articular osteochondral fragments on post-reduction plain films or CT.
3. Unstable Acetabular Fractures: Posterior wall fractures that result in dynamic hip instability (typically involving >20-30% of the posterior wall).
4. Displaced Femoral Head Fractures: Pipkin fractures requiring internal fixation or excision.
5. Progressive Sciatic Nerve Deficit: Occurring after a closed reduction attempt, suggesting nerve entrapment within the joint.
Preoperative and postoperative radiographs demonstrating a complex fracture-dislocation successfully managed with open reduction and internal fixation.
Surgical Approaches and Fixation Strategies
The Posterior Approach (Kocher-Langenbeck)
The Kocher-Langenbeck approach is the workhorse for posterior fracture-dislocations. It provides excellent visualization of the posterior column, posterior wall, and the posterior aspect of the femoral head.
Step-by-Step Surgical Technique:
1. Positioning: The patient is placed in the lateral decubitus or prone position on a radiolucent table.
2. Incision: A curved incision is made centered over the greater trochanter, extending proximally toward the posterior superior iliac spine and distally along the femoral shaft.
3. Superficial Dissection: The iliotibial band is split distally, and the gluteus maximus is split bluntly in line with its fibers proximally.
4. Nerve Protection: The sciatic nerve is systematically identified and protected. It must be handled with extreme care to prevent iatrogenic traction injury.
5. Deep Dissection: The short external rotators (piriformis, superior gemellus, obturator internus, inferior gemellus) are tagged and tenotomized near their femoral insertion. They are reflected posteriorly to cushion the sciatic nerve.
* Crucial Step: The quadratus femoris must be preserved if possible, or only partially released, to protect the ascending branch of the medial circumflex femoral artery (MCFA), which provides the primary blood supply to the femoral head.
6. Arthrotomy and Debridement: The posterior capsule is incised (or the traumatic rent is extended). The joint is distracted, and all intra-articular debris is irrigated and removed.
7. Fixation: Acetabular wall fragments are anatomically reduced and fixed with interfragmentary lag screws and a posterior buttress plate. Femoral head fractures can be fixed with countersunk headless compression screws.

Postoperative radiograph showing anatomic restoration of the posterior acetabular wall utilizing a contoured reconstruction plate and lag screws.
Axial CT and corresponding radiograph demonstrating precise plate placement along the posterior column to buttress the posterior wall fracture.
Management of Concomitant Femoral Fractures
In high-energy trauma, hip dislocations may present alongside ipsilateral femoral neck or shaft fractures. These complex scenarios require meticulous preoperative planning. The hip dislocation must be reduced first. If closed reduction is impossible due to a disconnected femoral shaft, open reduction of the hip is performed, followed by definitive fixation of the femur.

Radiographic sequence showing an ipsilateral femoral neck and shaft fracture. The neck fracture must be stabilized prior to or concurrently with intramedullary nailing of the shaft to prevent catastrophic displacement.

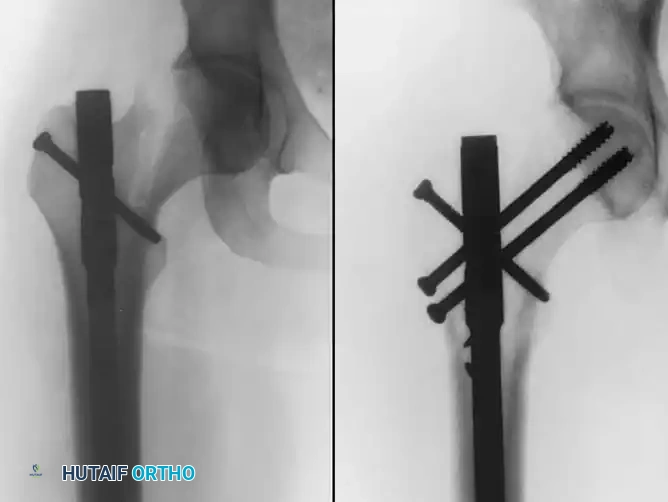
Fixation of a complex proximal femur fracture associated with hip trauma, utilizing a cephalomedullary nail combined with supplementary anterior neck screws for rotational control.
Postoperative Protocol and Rehabilitation
Postoperative management is tailored to the stability of the reduction and the presence of associated fractures.
- Immobilization: For pure dislocations (Type I) that are stable post-reduction, the patient is placed in an abduction pillow or a knee immobilizer to prevent hip flexion and adduction. Buck traction may be used temporarily to overcome muscle spasm.
- Weight-Bearing:
- Pure Dislocations: Touch-down weight-bearing (TDWB) for 2 to 4 weeks, progressing to full weight-bearing as pain allows.
- Fracture-Dislocations: Strict TDWB for 6 to 8 weeks to allow for bony union of the acetabulum or femoral head, followed by a graduated return to weight-bearing.
- Range of Motion: Passive and active-assisted range of motion exercises are initiated early to nourish the articular cartilage and prevent capsular contracture. Extremes of flexion (>90 degrees), adduction, and internal rotation are strictly avoided for 6 weeks.
- DVT Prophylaxis: Given the high-energy nature of the trauma and subsequent immobility, chemical thromboprophylaxis (e.g., LMWH) is mandatory unless contraindicated.
Complications
- Osteonecrosis (Avascular Necrosis): The most feared complication, occurring in 2% to 10% of pure dislocations and up to 40% of severe fracture-dislocations. The risk is directly correlated with the duration the hip remains dislocated.
- Posttraumatic Osteoarthritis: Results from initial chondral damage, retained intra-articular fragments, or subtle articular incongruity. It may necessitate total hip arthroplasty in the future.
- Sciatic Nerve Palsy: While 60% to 70% of patients experience partial or complete recovery of nerve function, permanent foot drop or sensory deficits can occur, requiring an ankle-foot orthosis (AFO).
- Heterotopic Ossification (HO): Common after extensive surgical approaches to the acetabulum. Prophylaxis with Indomethacin or single-fraction localized radiation therapy may be indicated in high-risk patients.
===```
You Might Also Like