Operative Spine Surgery: Applied Anatomy, Biomechanics, and Surgical Approaches
Key Takeaway
Mastering spinal surgery requires a profound understanding of vertebral biomechanics, pedicle morphometry, and regional neurovascular anatomy. This comprehensive guide details essential anterior and posterior surgical approaches across the cervical, thoracic, and lumbar spine. It provides orthopedic surgeons and neurosurgeons with evidence-based techniques, step-by-step procedural insights, and critical strategies for avoiding catastrophic complications such as recurrent laryngeal nerve palsy, vascular injury, and spinal cord ischemia.
Introduction to Spinal Anatomy and Surgical Principles
The evolution of operative orthopaedics and spine surgery is deeply rooted in a rigorous understanding of spinal anatomy, biomechanics, and the meticulous execution of surgical approaches. The spine functions as a dynamic, viscoelastic arch, protecting the neural elements while facilitating complex multi-planar motion. Surgical intervention—whether for trauma, degenerative disease, deformity, or oncologic resection—demands an uncompromising command of regional neurovascular anatomy, pedicle morphometry, and the physiologic limits of spinal cord blood flow.
This masterclass synthesizes foundational biomechanical principles and advanced surgical approaches to the cervical, thoracic, and lumbosacral spine. Designed for orthopedic residents, spine fellows, and practicing consultants, this guide details the indications, positioning, step-by-step surgical techniques, and complication avoidance strategies essential for modern spinal surgery.
Applied Surgical Anatomy and Biomechanics
Pedicle Morphometry and Instrumentation Biomechanics
The vertebral pedicle serves as the primary conduit for rigid spinal fixation. Transpedicular fixation relies on the precise understanding of age-related and regional variations in pedicle dimensions.
- Cervical Spine (C3-C7): Lower cervical pedicles exhibit significant morphometric variability. The pedicle diameter is typically narrowest at C3 and gradually widens toward C7. The medial angulation of cervical pedicles ranges from 30 to 45 degrees, necessitating precise preoperative computed tomography (CT) templating to avoid lateral mass breach and vertebral artery injury.
- Thoracic Spine (T1-T12): The thoracic pedicles are highly complex. The narrowest pedicles are consistently found between T4 and T6, often measuring less than 5 mm in transverse diameter. The medial angulation decreases from T1 to T12.
- Lumbar Spine (L1-L5): Lumbar pedicles are robust, with the transverse diameter increasing progressively from L1 to L5. The medial angulation also increases caudally, reaching up to 30 degrees at L5.
- Sacrum (S1): The S1 pedicle is massive but requires careful trajectory planning to avoid anterior cortical breach, which endangers the common iliac vessels and the L5 nerve root.
CLINICAL PEARL:
The pullout strength of a pedicle screw is directly proportional to the outer diameter of the screw, the thread depth, and the bone mineral density of the pedicle and vertebral body. Maximizing screw diameter without breaching the pedicle cortex is the cornerstone of biomechanically sound fixation.
Spinal Cord Blood Flow and Ischemia
The vascular supply to the spinal cord is segmental and highly vulnerable during anterior and posterior exposures. The critical vascular zone, often referred to as the "watershed area," is located in the mid-thoracic spine (T4-T9).
- Artery of Adamkiewicz: Typically arises between T8 and L1 on the left side. Injury to this vessel during anterior thoracolumbar approaches can result in catastrophic anterior spinal artery syndrome (paraplegia with loss of pain and temperature sensation, but preserved proprioception).
- Viscoelastic Relaxation: Prolonged spinal cord compression alters local blood flow. Decompression must be executed meticulously, as rapid reperfusion can occasionally lead to reperfusion injury or edema.
Anterior Surgical Approaches to the Spine
Anterior approaches provide direct access to the vertebral bodies and intervertebral discs, allowing for comprehensive decompression of the anterior neural elements and placement of interbody structural grafts.
Transoral Approach to the Upper Cervical Spine (C1-C2)
Indications: Anterior midline compressive pathology at the craniocervical junction, including basilar invagination, rheumatoid pannus, chordomas, and odontoid fractures non-amenable to posterior fixation.
Positioning: The patient is placed supine with the head secured in a Mayfield radiolucent skull clamp. The neck is slightly extended to maximize the distance between the mandible and the upper cervical spine.
Surgical Steps:
1. Preparation: A specialized transoral retractor (e.g., Crockard) is inserted to depress the tongue and elevate the soft palate.
2. Incision: A midline vertical incision is made through the posterior pharyngeal wall, extending from the lower clivus to the C2-C3 disc space.
3. Dissection: The longus colli muscles are elevated subperiosteally and retracted laterally.
4. Exposure: The anterior arch of C1 and the odontoid process of C2 are exposed. High-speed burrs are utilized for odontoidectomy or tumor resection.
SURGICAL WARNING:
Lateral dissection beyond 15 mm from the midline at the C1-C2 level places the vertebral arteries at imminent risk. The vertebral artery groove on the axis exhibits significant anatomic variation; preoperative CT angiography is mandatory.
Anterior Approach to the Subaxial Cervical Spine (Smith-Robinson)
Indications: Cervical radiculopathy, myelopathy, cervical disc herniation, spondylosis, and anterior cervical trauma.
Positioning: Supine with a gel roll placed vertically between the scapulae to induce mild cervical extension, opening the anterior disc spaces.
Surgical Steps:
1. Incision: A transverse incision is made within a natural skin crease (for 1-2 level pathology) or a longitudinal incision along the anterior border of the sternocleidomastoid (SCM) for multi-level disease. Left-sided approaches are historically preferred to reduce the risk of recurrent laryngeal nerve (RLN) injury, as the left RLN has a more constant, protected course within the tracheoesophageal groove.
2. Superficial Dissection: The platysma is divided in line with the incision. The superficial cervical fascia is incised anterior to the SCM.
3. Deep Dissection: The blunt dissection plane is developed between the carotid sheath (laterally) and the visceral axis (trachea and esophagus, medially).
4. Exposure: The prevertebral fascia is incised longitudinally over the midline. The longus colli muscles are elevated bilaterally to accommodate self-retaining retractors.
PITFALL:
Stretch-induced nerve injury to the recurrent laryngeal nerve is a primary cause of postoperative vocal cord paralysis. To minimize this, periodically release retractor tension during prolonged procedures and ensure the endotracheal tube cuff is temporarily deflated and reinflated after retractor placement to prevent compression of the RLN against the thyroid cartilage.
Anterior Retroperitoneal Approach to the Lumbar Spine (ALIF)
Indications: Lumbar degenerative disc disease, spondylolisthesis, pseudoarthrosis, and anterior column reconstruction.
Positioning: Supine with the lumbar spine positioned over the table break to allow for intraoperative lordosis recreation.
Surgical Steps:
1. Incision: A transverse or vertical paramedian incision is made.
2. Fascial Incision: The anterior rectus sheath is incised, and the rectus abdominis muscle is mobilized laterally.
3. Retroperitoneal Dissection: The posterior rectus sheath and transversalis fascia are carefully incised to enter the retroperitoneal space. The peritoneal sac is swept medially.
4. Vascular Mobilization: At L4-L5, the great vessels (aorta and inferior vena cava) bifurcate. The left common iliac vein must be mobilized to the right.
5. Exposure: The L5-S1 disc space is typically accessed below the bifurcation, within the "vascular window."
SURGICAL WARNING:
The iliolumbar vein is a critical tethering structure that drains into the left common iliac vein. During an L4-L5 exposure, the iliolumbar vein must be identified, ligated, and divided. Failure to do so will result in avulsion of the vein from the common iliac vein, leading to catastrophic, difficult-to-control hemorrhage. Furthermore, meticulous use of bipolar electrocautery over the L5-S1 disc space is required to prevent injury to the superior hypogastric plexus, which causes retrograde ejaculation in males.
Posterior and Posterolateral Surgical Approaches
Posterior approaches are the workhorse of spine surgery, providing access to the posterior tension band, facet joints, pedicles, and the posterior aspect of the spinal canal.
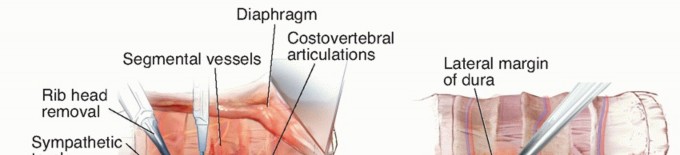
Lateral Extracavitary and Retropleural Approaches (Thoracolumbar)
Indications: Thoracolumbar fractures, osteomyelitis/discitis, and lateral thoracic disc herniations requiring anterior decompression without entering the pleural cavity.
Positioning: Prone or lateral decubitus.
Surgical Steps:
1. Incision: A curvilinear or "hockey-stick" incision is made over the targeted levels.
2. Muscle Dissection: The paraspinal musculature is elevated and retracted medially.
3. Rib Resection: The proximal 3 to 5 cm of the rib corresponding to the level of pathology is subperiosteally dissected and resected.
4. Pleural Mobilization: The parietal pleura is bluntly dissected away from the lateral aspect of the vertebral body.
5. Exposure: The pedicle is removed to expose the lateral dura, allowing for a corpectomy and anterior decompression from a posterior trajectory.
CLINICAL PEARL:
The retropleural approach significantly reduces pulmonary morbidity compared to a formal thoracotomy. However, the surgeon must be prepared to manage an inadvertent pleural tear with primary repair or the placement of a chest tube.
The Paraspinal Sacrospinalis-Splitting Approach (Wiltse)
Indications: Far lateral lumbar disc herniations, placement of pedicle screws, and minimally invasive transforaminal lumbar interbody fusion (TLIF).
Biomechanics: Traditional midline posterior approaches require extensive subperiosteal stripping of the multifidus and longissimus muscles, leading to denervation, ischemic necrosis, and postoperative "fusion disease" (chronic axial back pain). The Wiltse approach utilizes a natural intermuscular cleavage plane, preserving the neurovascular supply to the paraspinal musculature.
Surgical Steps:
1. Incision: A midline or bilateral paramedian incision is made.
2. Fascial Incision: The lumbodorsal fascia is incised 3 to 4 cm lateral to the midline.
3. Intermuscular Plane: Blunt dissection is used to separate the multifidus muscle (medially) from the longissimus muscle (laterally).
4. Exposure: This plane leads directly to the facet joint, the pars interarticularis, and the transverse process—the exact anatomic landmarks required for pedicle screw starting points.
Postoperative Protocols and Complication Management
The success of complex spinal surgery extends beyond the operating room. Rigorous postoperative protocols are essential for optimizing fusion rates and mitigating complications.
Neurologic Monitoring and Recovery
- Spinal Cord Ischemia: If intraoperative neuromonitoring (SSEP/MEP) signals are lost, immediate steps must be taken: increase mean arterial pressure (MAP > 85-90 mmHg), reverse any induced deformity correction, ensure adequate oxygenation, and administer warm irrigation.
- C5 Palsy: A known complication following extensive cervical decompression (anterior or posterior). It is believed to be caused by nerve root tethering or reperfusion injury. Most cases are managed conservatively with physical therapy, and the majority recover within 6 to 12 months.
Vascular and Visceral Complications
- Chylothorax: An unusual but severe complication of anterior thoracic approaches, resulting from injury to the thoracic duct. Management includes closed tube thoracostomy, a medium-chain triglyceride (MCT) diet, or total parenteral nutrition (TPN). Refractory cases require surgical ligation or percutaneous embolization.
- Urogenital Complications: As noted, anterior lumbar approaches carry a risk of retrograde ejaculation. Preoperative counseling is mandatory for male patients undergoing ALIF at L5-S1.
Rehabilitation and Mobilization
- Early Mobilization: Unless contraindicated by dural tears or unstable constructs, patients should be mobilized on postoperative day one to prevent deep vein thrombosis (DVT), pulmonary embolism (PE), and atelectasis.
- Orthotic Management: The use of postoperative orthoses (e.g., rigid cervical collars, TLSO braces) depends on bone quality, construct rigidity, and patient compliance. Modern rigid pedicle screw fixation has significantly reduced the reliance on postoperative bracing.
Conclusion
The mastery of operative orthopaedics in the spine is an ongoing pursuit of anatomic precision and biomechanical optimization. Whether navigating the precarious vertebral artery groove in the upper cervical spine, managing the delicate vascular window of the anterior lumbar spine, or executing a muscle-sparing Wiltse approach, the surgeon's success is predicated on a profound respect for the complex, three-dimensional anatomy of the human spine. By adhering to strictly evidence-based techniques and maintaining vigilance against neurovascular complications, spine surgeons can consistently achieve superior clinical outcomes in the face of challenging spinal pathology.
You Might Also Like