Jobe Four-Limb Reconstruction of the Thumb UCL
Key Takeaway
The Jobe four-limb reconstruction is a robust surgical technique designed to address chronic ulnar collateral ligament (UCL) instability of the thumb metacarpophalangeal joint. By utilizing a free tendon autograft, typically the palmaris longus, routed through precisely placed osseous tunnels in the proximal phalanx and metacarpal head, this procedure restores both the proper and accessory collateral ligaments. It provides superior biomechanical stability, allowing for early rehabilitation and optimal functional recovery in high-demand patients.
INTRODUCTION TO THUMB UCL INSTABILITY AND RECONSTRUCTION
Chronic instability of the ulnar collateral ligament (UCL) of the thumb metacarpophalangeal (MCP) joint—often referred to as chronic Gamekeeper’s thumb or the sequelae of an untreated Stener lesion—presents a significant functional deficit. The UCL is the primary restraint to valgus stress at the MCP joint, and its incompetence leads to profound weakness in pinch grip, pain, and progressive articular degeneration.
When direct anatomical repair is no longer feasible due to tissue retraction, attenuation, or poor tissue quality, ligamentous reconstruction becomes the gold standard. The Jobe Four-Limb Reconstruction is an internationally recognized, biomechanically superior technique that utilizes a free tendon autograft (most commonly the palmaris longus) to anatomically recreate both the proper and accessory components of the UCL. By routing the graft through precisely drilled osseous tunnels in the metacarpal head and the base of the proximal phalanx, the surgeon restores the multi-planar stability required for high-demand hand function.
CLINICAL ANATOMY AND BIOMECHANICS
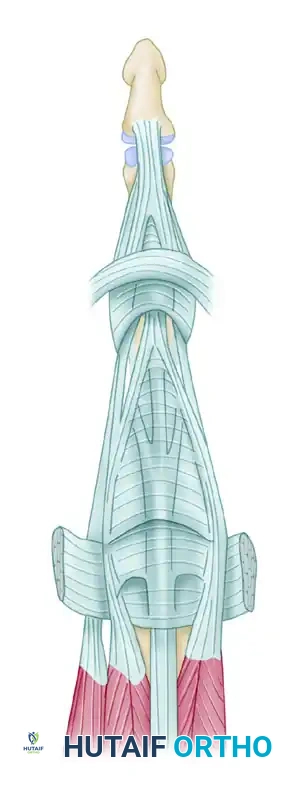
A profound understanding of the thumb MCP joint anatomy is mandatory for successful reconstruction. The UCL complex consists of two distinct functional bands:
* Proper Ulnar Collateral Ligament (pUCL): Originates from the dorsal third of the metacarpal head and inserts onto the volar aspect of the proximal phalanx base. It is the primary restraint to valgus stress when the MCP joint is in flexion.
* Accessory Ulnar Collateral Ligament (aUCL): Originates volar to the pUCL and inserts onto the volar plate and sesamoid. It is the primary restraint to valgus stress when the MCP joint is in extension.
The Jobe four-limb reconstruction is uniquely designed to address both bands. By utilizing two phalangeal insertion points and routing the graft in a figure-of-eight or parallel limb configuration, the construct mimics the isometric tensioning of the native ligament complex across the entire arc of motion.
💡 Clinical Pearl: The Stener Lesion
In acute injuries, the adductor pollicis aponeurosis can interpose between the torn UCL and its phalangeal insertion, creating a Stener lesion. This prevents anatomical healing and guarantees chronic instability if not surgically addressed. In chronic cases, the scarred remnants of the UCL are often found retracted proximal to the adductor aponeurosis.
PREOPERATIVE EVALUATION AND DIFFERENTIAL DIAGNOSIS
Thorough clinical examination involves valgus stress testing of the thumb MCP joint in both full extension (testing the aUCL and volar plate) and 30 degrees of flexion (testing the pUCL). An opening of greater than 30 degrees, or a side-to-side difference of more than 15 degrees compared to the contralateral uninjured thumb, indicates complete rupture.
Radiographic Assessment and the Bennett Fracture Differential
Standard posteroanterior, lateral, and Robert's view radiographs are essential to evaluate for joint subluxation, osteoarthritis, or avulsion fractures.
It is critical to differentiate chronic UCL insufficiency from other base-of-thumb pathologies that present with weakness and pain. For instance, intra-articular fractures of the thumb metacarpal base must be ruled out. As noted in classic trauma principles, one must carefully assess for metacarpal displacement in a Bennett fracture, which is driven proximally and radially by the deforming force of the abductor pollicis longus (APL).
In addition to routine anteroposterior and lateral views, a radiograph should be made with 30 degrees of pronation to give a better view of the articular surface for accurate diagnosis of a Bennett fracture. While acute Bennett fractures often can be reduced by longitudinal traction and percutaneous pinning (subsequently protected by a cast), fractures that are not recognized early and heal in a displaced position may benefit from corrective osteotomy of the malunion or resection arthroplasty. Ensuring the MCP joint symptoms are not referred from an undiagnosed carpometacarpal (CMC) joint issue is a vital step in preoperative planning.
SURGICAL TECHNIQUE: JOBE FOUR-LIMB RECONSTRUCTION
1. Patient Positioning and Anesthesia
The procedure is performed under regional anesthesia (supraclavicular or axillary brachial plexus block) or general anesthesia. The patient is positioned supine with the operative arm extended on a radiolucent hand table. A well-padded pneumatic tourniquet is applied to the proximal arm and inflated to 250 mm Hg after exsanguination with an Esmarch bandage.
2. Graft Harvest
The palmaris longus tendon is the graft of choice due to its accessibility and minimal donor site morbidity.
* Confirm the presence of the palmaris longus preoperatively.
* Harvest the tendon using a minimally invasive tendon stripper through a small transverse incision at the distal wrist crease.
* If the palmaris longus is absent, alternatives include a slip of the abductor pollicis longus (APL), the plantaris tendon, or a toe extensor.
* Prepare the graft on the back table by clearing it of paratenon and placing running locking sutures (e.g., 4-0 nonabsorbable) at both ends to facilitate passage.
3. Surgical Approach and Exposure
- Make a lazy-S or gently curved longitudinal incision over the ulnar aspect of the thumb MCP joint.
- Nerve Protection: Carefully dissect through the subcutaneous tissues. Identify and meticulously retract the terminal branches of the superficial radial nerve (SRN) and the dorsal sensory branch of the ulnar nerve. Neuropraxia of these nerves is a common and highly distressing postoperative complication.
- Identify the adductor aponeurosis. Incise it longitudinally parallel to the extensor pollicis longus (EPL) tendon to expose the underlying joint capsule.
- Separate the capsular tissue and completely excise the old, scarred ulnar collateral ligament from its origin on the metacarpal head and its insertion on the proximal phalanx.
4. Preparation of the Osseous Tunnels
Accurate placement of the bone tunnels is the most critical step in ensuring joint isometry and preventing graft laxity or restriction of motion.
Phalangeal Tunnels:
* Identify the planned sites of the two pairs of holes according to normal anatomical positions for metacarpophalangeal joint anatomy.
* The distal holes correspond to the proper and accessory ulnar collateral ligament phalangeal attachments.
* Make these two phalangeal holes 2.75 mm in diameter.
* Crucial Step: Leave a solid cortical bone bridge of 3 to 4 mm between them to prevent iatrogenic fracture during tensioning.
* Carefully channel these two holes together within the cancellous bone using a small curved curette or a specialized passing instrument, creating a U-shaped tunnel.
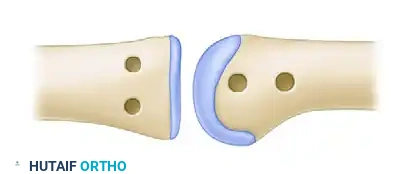
Figure 67-27A: Position of metacarpal and phalangeal holes for passage of the tendon graft.
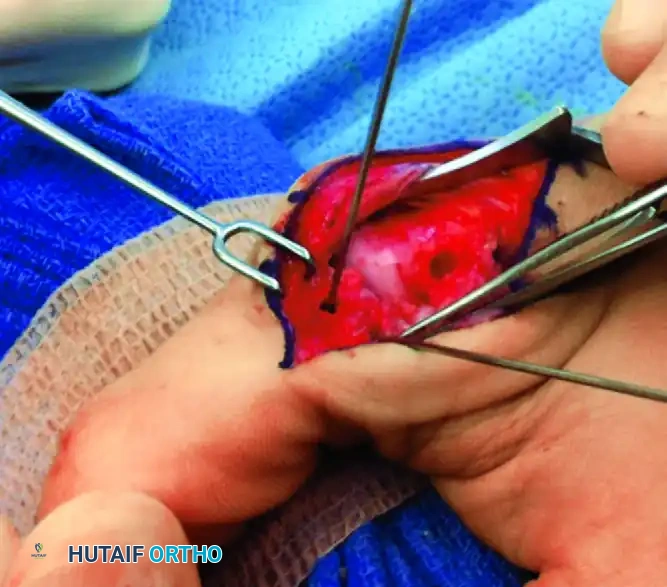
Figure 67-27B: Detailed view of the phalangeal bone bridge and metacarpal tunnel placement.
Metacarpal Tunnels:
* Make two 3-mm holes in the metacarpal head.
* Place the most distal hole precisely in the anatomical ulnar collateral ligament fossa (the isometric point).
* Place the second hole approximately 5 mm more proximally along the ulnar neck of the metacarpal.
* Communicate these two holes internally using a curette, strictly protecting the intervening bone bridge.
⚠️ Surgical Warning: Bone Bridge Integrity
The integrity of the 3 to 4 mm bone bridges on both the phalanx and the metacarpal is paramount. Aggressive reaming or the use of oversized drill bits can lead to cortical blowout. If a blowout occurs, the surgeon must immediately pivot to an alternative fixation method, such as suture anchors or a biotenodesis screw.
5. Graft Passage
- Pass the prepared tendon graft (palmaris longus or equivalent) through the U-shaped phalangeal tunnel. Ensure the graft slides smoothly without catching on cancellous bone spicules.
- Take the two free limbs of the graft and pass them together through the distal hole in the ulnar collateral ligament fossa of the metacarpal head.
- Subsequently, route both limbs out through the more proximal metacarpal hole.
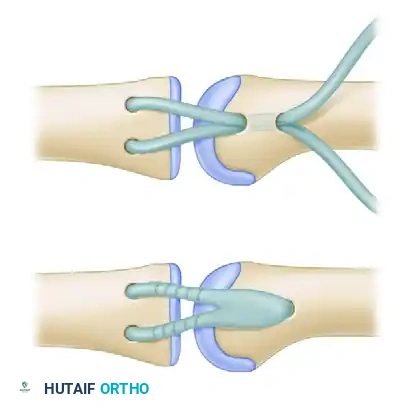
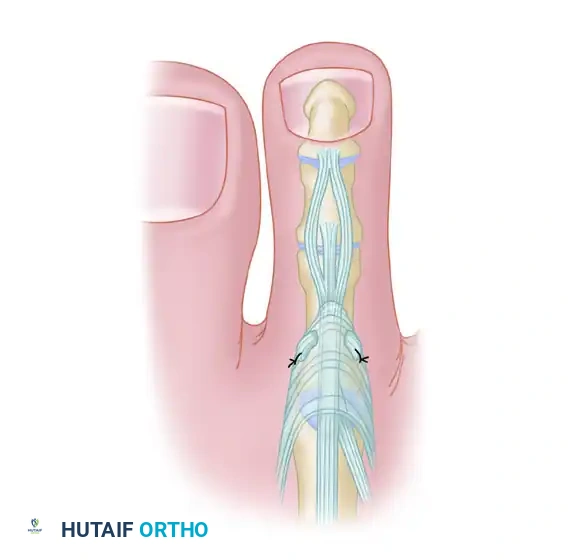
Figure 67-27C: Passage of the graft through the phalangeal and metacarpal osseous tunnels.
6. Tensioning and Fixation
The surgeon must now assess joint reduction and establish the correct tension on the two free limbs. The MCP joint should be held in approximately 20 to 30 degrees of flexion with a mild ulnar deviation force applied to close the joint space anatomically.
Option A: Suture Fixation over Bone Bridge
* Once the correct tension has been established, fold the limbs distally back onto themselves.
* Use robust nonabsorbable sutures (e.g., 3-0 or 4-0 braided polyester or ultra-high-molecular-weight polyethylene) to secure the construct.
* The graft can be secured either over a button, a catheter tip, or sutured directly to the adjacent periosteum and itself to create a reinforced, four-limb construct.
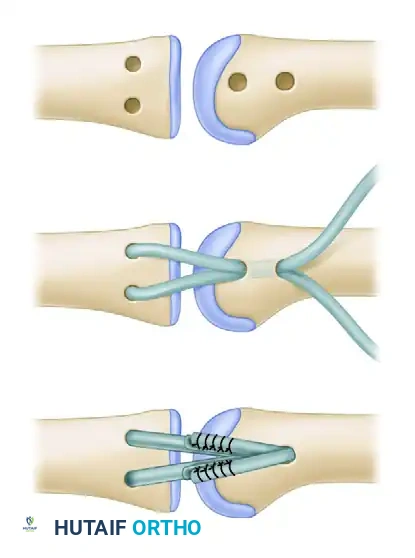
Figure 67-27D: Final position of the graft folded back and prepared for suturing.
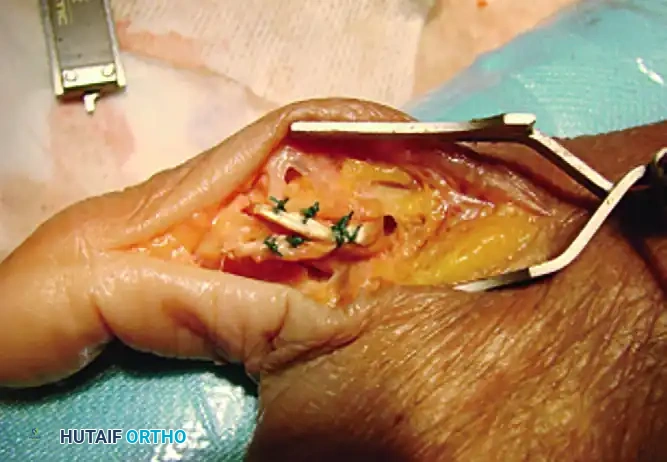
Figure 67-27E: Final position of the graft fixed securely with nonabsorbable sutures.
Option B: Biotenodesis Screw Fixation
Modern advancements allow for the use of a biotenodesis screw, which provides excellent pull-out strength and allows for a more streamlined metacarpal preparation.
* For screw fixation, make only one hole in the UCL fossa and continue it transversely across the metacarpal head to the radial cortex.
* Grasp the two limbs of the free graft and pass them into the hole in the metacarpal head that has been specifically reamed to match the diameter of the appropriate tenodesis screw (typically 3.0 mm or 4.0 mm).
* Adjust tension on the free suture ends exiting the radial side.
* Once appropriate joint reduction and tension are achieved, advance the tenodesis screw into the metacarpal head, locking the graft limbs against the cortical wall.
* Excise the redundant tendon ends and/or sutures emerging from the radial side of the metacarpal head.

Figure 67-28: Fixation of the graft utilizing a biotenodesis screw in the metacarpal head.
7. Joint Transfixation and Closure
- If there is any question regarding graft engagement, bone quality, or patient compliance, protect the construct with a 0.045-inch Kirschner wire.
- Carefully drive the Kirschner wire across the MCP joint, transfixing it in 20 degrees of flexion. Redirect the wire if it encounters the intra-osseous graft.
- Repair the adductor aponeurosis and close the triangular oblique extensor expansion flap using absorbable sutures (e.g., 4-0 Vicryl).
- Deflate the tourniquet, achieve meticulous hemostasis, and close the skin in a routine fashion with nonabsorbable monofilament sutures.
POSTOPERATIVE CARE AND REHABILITATION
The success of the Jobe four-limb reconstruction relies heavily on a disciplined, phased rehabilitation protocol. The reconstructed ligament requires adequate time for osseous integration within the tunnels before dynamic stress is applied.
Phase I: Immobilization (Weeks 0 to 4-5)
* Immediately postoperatively, the thumb is immobilized in a rigid thumb spica cast or a custom thermoplastic splint.
* The interphalangeal (IP) joint may be left free to prevent extensor mechanism adhesions, provided the MCP joint is rigidly stabilized.
* The reconstruction is strictly protected for 4 to 5 weeks.
Phase II: Pin Removal and Early Motion (Weeks 5 to 8)
* At the 4 to 5-week mark, the transarticular Kirschner wire (if utilized) is removed in the clinic.
* The rigid cast is transitioned to a removable custom thumb spica splint, which is worn at all times except during therapy sessions.
* Supervised hand therapy is initiated. Active range of motion (AROM) and active-assisted range of motion (AAROM) exercises for the MCP and IP joints begin.
* Caution: Passive stretching and valgus stress must be strictly avoided during this phase.
Phase III: Strengthening (Weeks 8 to 12)
* Splint wear is gradually discontinued for light activities of daily living.
* Progressive strengthening exercises, including gentle pinch and grip strengthening, are introduced.
* Dynamic splinting may be considered if MCP joint flexion is lagging, though stiffness is generally preferred over recurrent instability.
Phase IV: Return to Activity (Months 3 to 6)
* Unrestricted use of the hand is typically permitted by 12 weeks postoperatively.
* Heavy manual laborers or athletes involved in contact sports may require a protective taping or a soft functional orthosis during high-risk activities for up to 6 months.
COMPLICATIONS AND PITFALLS
While highly successful, the Jobe four-limb reconstruction carries specific risks that the orthopedic surgeon must anticipate:
- Superficial Radial Nerve (SRN) Injury: The most common complication. Neuroma formation or complex regional pain syndrome (CRPS) can result from aggressive retraction. Meticulous soft tissue handling is non-negotiable.
- Cortical Blowout: Fracture of the 3-4 mm bone bridge during drilling or tensioning compromises the entire construct. If this occurs, the surgeon must convert to suture anchor fixation.
- MCP Joint Stiffness: A slight loss of terminal flexion is common and generally well-tolerated. It is a preferable outcome compared to recurrent valgus instability. Early IP joint motion helps mitigate extensor tendon adhesions.
- Graft Laxity: Often caused by non-isometric tunnel placement (specifically, placing the metacarpal tunnel too far dorsally or proximally). This results in a graft that stretches out over time, leading to failure of the reconstruction.
CONCLUSION
The Jobe four-limb reconstruction remains a cornerstone technique in operative orthopaedics for the management of chronic thumb MCP joint instability. By respecting the intricate biomechanics of the proper and accessory collateral ligaments, and executing precise osseous tunnel placement, surgeons can reliably restore pinch strength, alleviate pain, and halt the progression of post-traumatic arthritis in the thumb. Mastery of this technique, alongside rigorous postoperative rehabilitation, ensures excellent long-term functional outcomes for patients.
You Might Also Like