Dynamic Distraction External Fixation for PIP Joint Fracture-Dislocations
Key Takeaway
Dynamic distraction external fixation is a highly effective surgical technique for managing unstable fracture-dislocations of the proximal interphalangeal (PIP) joint. By utilizing a precise construct of Kirschner wires and elastic traction, this method restores joint congruity through ligamentotaxis while permitting immediate active range of motion. This guide details the biomechanical principles, step-by-step surgical application, and postoperative rehabilitation protocols essential for optimizing functional outcomes in complex digital trauma.
INTRODUCTION TO PIP JOINT FRACTURE-DISLOCATIONS
Fracture-dislocations of the proximal interphalangeal (PIP) joint represent one of the most challenging intra-articular injuries in hand surgery. The PIP joint is a highly constrained, ginglymus (hinge) joint that relies on a complex interplay of osseous congruity, the volar plate, and collateral ligaments for stability. When axial load and hyperextension forces exceed the structural integrity of the joint, the result is typically a dorsal fracture-dislocation involving the volar base of the middle phalanx.
If the fracture involves more than 30% to 40% of the articular surface, the collateral ligaments remain attached to the fractured volar fragment, rendering the remaining dorsal portion of the middle phalanx highly unstable and prone to dorsal subluxation. Traditional immobilization often leads to devastating stiffness, while extensive open reduction and internal fixation (ORIF) can result in severe scarring and loss of motion.
To circumvent these complications, Dynamic Distraction External Fixation was developed. Pioneered by Agee (Force-Couple Splint) and later refined by Ruland et al., this technique utilizes the principles of ligamentotaxis and a mechanical force-couple to maintain concentric joint reduction while allowing immediate, active range of motion.
BIOMECHANICAL PRINCIPLES
The success of dynamic distraction external fixation relies on two primary biomechanical concepts: Ligamentotaxis and the Force-Couple Mechanism.
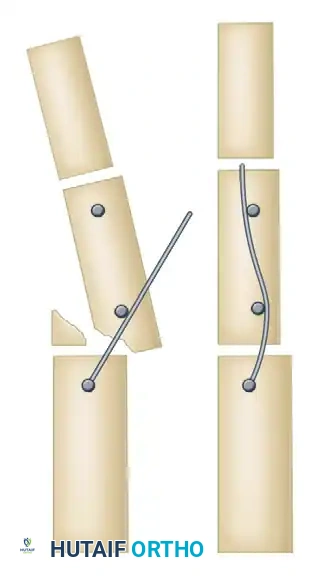
Ligamentotaxis
By applying longitudinal traction across the PIP joint, tension is imparted to the intact soft tissue envelope (specifically the collateral ligaments and the extensor mechanism). This tension acts to realign the fracture fragments and maintain the joint space, preventing the articular surfaces from grinding against one another during flexion and extension.
The Force-Couple Mechanism
In a standard dorsal fracture-dislocation, the middle phalanx tends to subluxate dorsally. The dynamic fixator counteracts this by creating a force couple:
1. A dorsally directed force is applied to the head of the proximal phalanx.
2. A palmarly (volarly) directed force is applied to the base of the middle phalanx.
This dynamic interplay forces the middle phalanx into a reduced, concentric position within the condyles of the proximal phalanx, maintaining this relationship throughout the entire arc of motion.
Surgical Pearl: The dynamic fixator does not rigidly hold the fracture fragments together; rather, it holds the joint in a reduced state. The fracture heals secondarily while the joint cartilage is nourished through continuous active motion.
INDICATIONS AND CONTRAINDICATIONS
Indications
- Unstable dorsal fracture-dislocations of the PIP joint (typically involving >30% of the volar articular base).
- Comminuted PIP joint pilon fractures (with construct modifications).
- Chronic fracture-dislocations (often requiring limited open reduction prior to frame application).
- Patients compliant enough to participate in early active motion protocols.
Contraindications
- Purely volar dislocations with dorsal articular fractures (requires a reversed force-couple construct).
- Severe soft tissue compromise or active infection at the pin insertion sites.
- Lack of intact collateral ligaments (though rare in these specific fracture patterns, their absence negates the ligamentotaxis effect).
- Non-compliant patients unable to manage pin care or perform required exercises.
PREOPERATIVE PLANNING AND SETUP
Operating Room Setup
- Anesthesia: Regional block (e.g., wrist block or digital block) is preferred to allow intraoperative patient participation. The patient must be awake to actively flex and extend the digit to confirm concentric reduction.
- Imaging: Mini C-arm fluoroscopy is mandatory.
- Equipment:
- 0.045-inch (1.14 mm) Kirschner wires (smooth and threaded options).
- Wire cutters and heavy needle holders/wire benders.
- Dental rubber bands (orthodontic elastics).
- Needle for joint line identification.
SURGICAL TECHNIQUE: STEP-BY-STEP GUIDE
The following technique synthesizes the foundational Agee Force-Couple principles with the highly adaptable Ruland Dynamic Distraction modification.
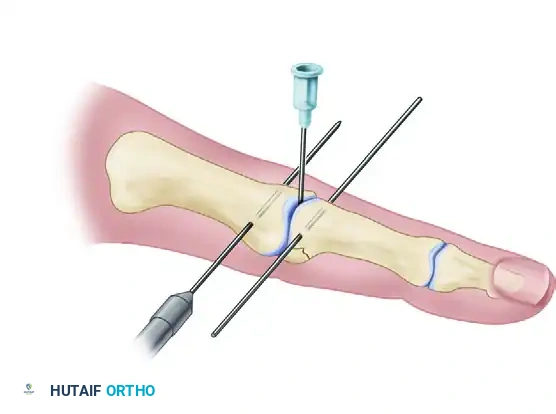
Step 1: Closed Reduction and Joint Identification
Under fluoroscopic guidance, attempt a closed reduction of the PIP joint. Apply longitudinal traction and volar pressure to the middle phalanx.
If closed reduction is impossible due to interposed soft tissue or impacted osteochondral fragments, a limited mid-axial or volar open incision may be necessary to disimpact the fragments and achieve a concentric reduction. Once reduced, identify the exact rotational axis of the PIP joint. A hypodermic needle can be used as a radiographic marker to identify the joint line accurately.
Step 2: Placement of the Proximal Axis Pin (Wire #1)
The first 0.045-inch K-wire is the most critical. It must be placed exactly through the center of the rotational axis of the proximal phalangeal head.
1. Identify the true lateral center of the condyles under fluoroscopy.
2. Drive the K-wire transversely from lateral to medial.
3. Ensure the wire is perfectly perpendicular to the longitudinal axis of the digit in the coronal plane.
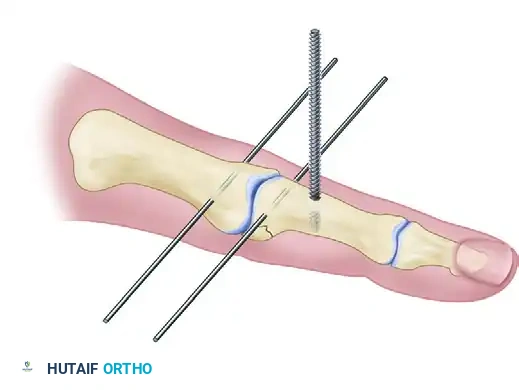
Once inserted, bend the ends of this wire 90 degrees distally, running parallel along the longitudinal axis of the digit. Rotate this entire construct dorsally to move it out of the way for the placement of the subsequent pins.
Step 3: Placement of the Distal Pin (Wire #2)
The second 0.045-inch K-wire is placed in the middle phalanx.
1. Target the distal metadiaphyseal junction of the middle phalanx.
2. The wire must be placed parallel to the distal interphalangeal (DIP) joint and parallel to the first wire.
3. Drive the wire transversely through the bone.
Surgical Warning: Ensure this distal wire does not tether the extensor lateral bands. Place it strictly mid-axial to avoid restricting DIP joint motion.
Step 4: Placement of the Fulcrum Pin (Wire #3)
Note: This step is specific to the Ruland modification for dorsal fracture-dislocations. See the "Pilon Fracture Modification" section below if dealing with a pilon variant.
The third wire acts as the mechanical fulcrum.
1. Place this wire in the middle third of the middle phalanx, distal to the fracture site.
2. It must be positioned along the axis created by the first two wires.

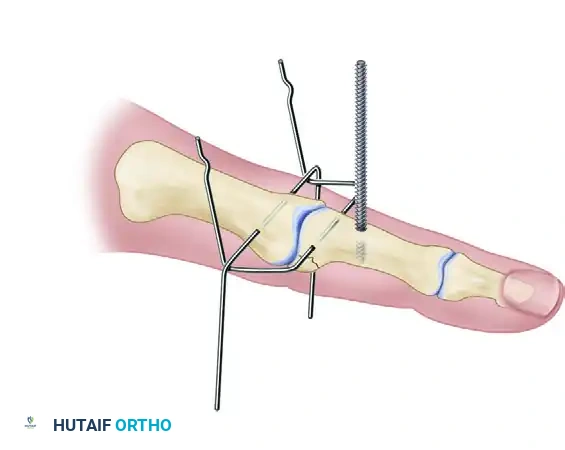
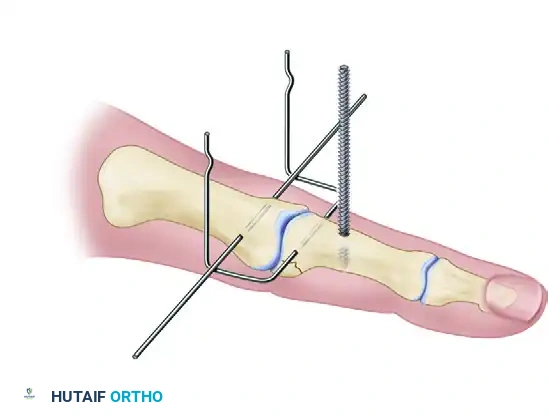
Step 5: Frame Assembly and Bending (Agee vs. Ruland Constructs)
At this stage, the surgeon must fashion the frame. The historical Agee technique utilizes a threaded central wire and complex 90-degree bends to create a rigid force-couple splint.
The Agee Force-Couple Bending Sequence:
If utilizing the Agee method, a threaded K-wire is inserted dorsal to palmar in the middle phalanx.
The distal wire is then bent 90 degrees on each side.

A second 90-degree bend is made in the distal wire, and a hook is fashioned into the end of the wire.
The proximal wire is then bent 90 degrees palmarward on each side to engage the construct.
This results in the completed Agee splint, allowing almost full range of active motion.
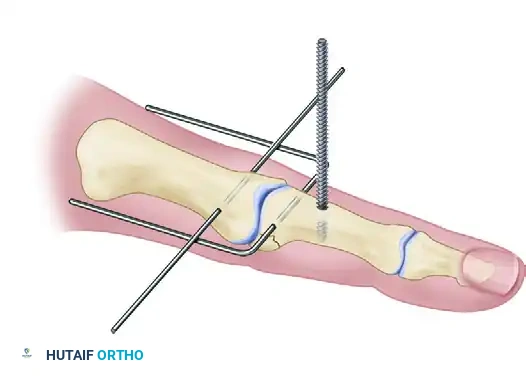
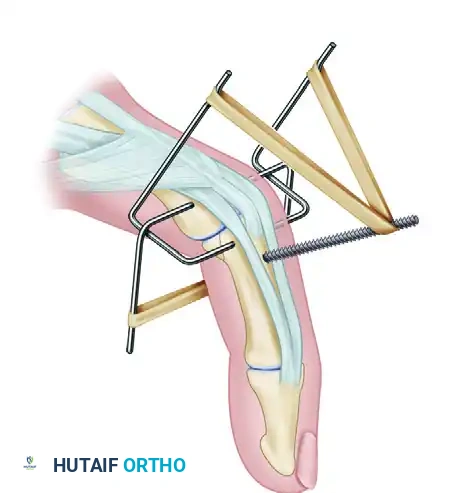
The Ruland Dynamic Distraction Assembly:
The modern Ruland technique simplifies the bending process and utilizes elastic traction.
1. Rotate the first wire (proximal axis pin) over the third wire (the fulcrum) and under the second wire (distal pin).
2. This specific over-under weaving provides the critical biomechanical force: a dorsally directed force on the proximal phalangeal head and a palmarly directed force on the middle phalangeal base.
- Fashion the free ends of the first wire into upward-facing hooks.
- Fashion the free ends of the second wire into downward-facing hooks.
- Cut any excess wire to prevent soft tissue irritation or catching on clothing.
Step 6: Application of Dynamic Traction
Apply dental rubber bands between the hooks of the first and second wires.
* Usually, two rubber bands (one on each side) are sufficient to provide adequate in-line traction across the PIP joint.
* The elastic bands generate continuous distraction, engaging ligamentotaxis to pull the fracture fragments into alignment.

Step 7: Intraoperative Dynamic Testing
This is a critical quality-control step. With the regional block active, instruct the patient to actively flex and extend the finger.
* Observe the joint under live fluoroscopy during the entire arc of motion.
* The joint must remain concentrically reduced from full extension to full flexion.
* If the joint hinges, subluxates dorsally, or if the joint space is asymmetric, the traction is insufficient. Apply a third rubber band to increase the distraction force.
* Conversely, if the joint is over-distracted (joint space significantly wider than adjacent normal digits), reduce the tension by using weaker bands or removing one band.

Modification for Pilon Fractures
Critical Pitfall: If a PIP joint pilon fracture (comminution of both the dorsal and volar base of the middle phalanx) is present, do not use the fulcrum wire (Wire #3).
In pilon fractures, the volar cortex is not intact. Applying a palmarly directed force via the fulcrum will cause apex dorsal angulation and collapse of the fracture site. In these cases, the third wire is omitted from the force-couple and is merely used for frame control and pure longitudinal distraction.
POSTOPERATIVE CARE AND REHABILITATION
The primary advantage of dynamic distraction external fixation is the ability to initiate immediate motion. A strict, supervised rehabilitation protocol is paramount to success.
Phase 1: Immediate Postoperative (Days 1-7)
- Edema Control: Elevation and compressive wrapping of the hand (leaving the affected digit free for motion).
- Active ROM: Immediate, supervised active range of motion exercises are initiated. The patient is instructed to perform full flexion and extension of the PIP joint 10-15 times every hour while awake.
- Pin Care: Daily cleaning of the pin sites with chlorhexidine or half-strength hydrogen peroxide. Application of sterile gauze to prevent crusting. Use of oral antibiotics (e.g., first-generation cephalosporin) is recommended if pin sites show early signs of erythema or concern.
Phase 2: Maintenance and Monitoring (Weeks 1-6)
- Radiographic Surveillance: Weekly radiographs (PA and true lateral) are mandatory for the first 3 weeks to evaluate the maintenance of concentric reduction and joint space.
- Traction Adjustment: If the joint space exceeds that of the adjacent normal fingers on follow-up radiographs, the rubber bands must be reduced in number or strength to prevent over-distraction, which can lead to delayed union or nonunion.
- Therapy: Continue aggressive active ROM. Passive ROM is generally avoided to prevent excessive stress on the healing fracture and pin-bone interface.
Phase 3: Frame Removal (Week 6)
- At approximately 6 weeks, or when there are clear radiographic signs of fracture union and clinical stability, the external fixator is removed in the clinic.
- Following removal, buddy taping to an adjacent digit is utilized for an additional 2 to 4 weeks during strenuous activities.
- Strengthening exercises and, if necessary, gentle passive stretching are initiated to maximize final functional recovery.
COMPLICATIONS AND MANAGEMENT
While highly effective, dynamic distraction external fixation carries specific risks that the surgeon must anticipate and manage.
- Pin Tract Infection: The most common complication. Prevented by meticulous surgical technique (avoiding thermal necrosis during drilling) and rigorous postoperative pin care. Minor infections are treated with oral antibiotics; deep infections require immediate pin removal.
- Loss of Reduction: Usually occurs due to inadequate initial elastic traction, pin loosening, or failure to place the proximal pin exactly in the axis of rotation. Requires immediate frame adjustment or revision.
- Over-Distraction: Leads to delayed union, nonunion, or intrinsic minus posturing. Monitored via weekly radiographs and managed by decreasing rubber band tension.
- Joint Stiffness: Despite early motion, some loss of terminal extension (typically 10-15 degrees) is common and should be discussed with the patient preoperatively. Severe stiffness usually results from patient non-compliance with the active motion protocol.
- Pin Migration/Cut-out: Occurs in severely osteoporotic bone or if pins are placed too close to the fracture site. May necessitate conversion to internal fixation or a static spanning fixator if the joint cannot be maintained.
CONCLUSION
Dynamic distraction external fixation remains a cornerstone technique in the armamentarium of the hand and orthopedic surgeon for managing complex PIP joint fracture-dislocations. By respecting the anatomical axis of rotation, harnessing the power of ligamentotaxis, and enforcing strict postoperative active motion, surgeons can restore joint congruity and achieve excellent functional outcomes in injuries that historically carried a poor prognosis. Mastery of both the Agee force-couple principles and the Ruland construct modifications ensures adaptability to various fracture patterns encountered in clinical practice.
You Might Also Like


