Comprehensive Postoperative Management and Rehabilitation in Hand Surgery
Key Takeaway
Optimal postoperative care in hand surgery requires a delicate balance between tissue protection and early functional rehabilitation. This comprehensive guide details evidence-based protocols for dressing application, edema control, and splinting. It emphasizes the critical role of multidisciplinary hand therapy, strict elevation, and strategic wound surveillance to prevent complications, minimize scar contracture, and maximize functional outcomes in the upper extremity.
INTRODUCTION TO POSTOPERATIVE HAND CARE
The success of any surgical intervention in the upper extremity is inextricably linked to the quality of the postoperative management. Care after surgery must be orchestrated intelligently and meticulously so that traumatized tissues are allowed to heal without disruption, while the biomechanical functions of the affected part are restored as rapidly and safely as possible. The hand is an unforgiving anatomical structure; even minor deviations in postoperative protocols can result in catastrophic stiffness, debilitating edema, or irreversible joint contractures.
Postoperative care does not begin in the recovery room; it begins in the operating theater with the application of the surgical dressing. This comprehensive guide delineates the textbook-level, evidence-based protocols for postoperative management, encompassing dressing application, edema control, immobilization biomechanics, wound surveillance, and the integration of multidisciplinary hand therapy.
PRINCIPLES OF THE SURGICAL DRESSING
The surgical dressing in hand surgery is not merely a passive covering; it is an active therapeutic device designed to control edema, absorb exudate, immobilize specific joints, and protect the healing wound from mechanical shear and bacterial contamination. The routine dressing is applied in a highly structured, multi-layered fashion.
The Primary Contact Layer
A closely woven, non-adherent patch of gauze (such as Xeroform or Adaptic) is placed directly over each incision.
Clinical Pearl: The primary function of the non-adherent layer is to prevent granulation tissue from growing through the dressing material. If standard dry gauze is used, capillary loops will interweave with the fabric, causing severe pain, disruption of the delicate healing epithelium, and micro-hemorrhage upon removal. Furthermore, petrolatum-based or emulsion-impregnated gauze prevents the wound from becoming macerated by allowing exudate to pass through to the secondary layer while maintaining a physiologically moist wound environment.
The Intermediate Conforming Layer
After the hand has been positioned properly—typically in the "position of safe immobilization" (intrinsic-plus position)—the intermediate layer is applied. Cotton sponges or synthetic (Acrilan) sponges that have been moistened in sterile saline or a glycerin solution are placed carefully around the digits and the hand.
The use of moistened sponges is a critical biomechanical technique. Moist sponges conform to the complex, three-dimensional contours of the hand much more accurately than dry sponges. By conforming perfectly to the web spaces and the palmar arches, they distribute compressive pressure evenly across the integument, adhering to Pascal’s principle of fluid pressure. This prevents focal areas of ischemia that can lead to pressure necrosis. Additionally, the capillary action of the moistened sponges promotes the rapid absorption of blood and serous exudate, drawing it away from the incision site.
The Outer Compressive and Splinting Layer
Once the conforming layer is in place, a roll of cotton or synthetic sheet wadding (cast padding) is wrapped circumferentially around the hand and forearm to provide a uniform layer of soft tissue protection.
Finally, an appropriate splint—constructed of either plaster of Paris or modern fiberglass—is applied. The splint is secured and held in precise position with a roll of 2-inch or 3-inch conforming gauze bandage.
TOURNIQUET MANAGEMENT AND HEMOSTASIS
The transition from the intraoperative to the postoperative phase is marked by the deflation of the pneumatic tourniquet. The management of the extremity during this exact moment dictates the degree of postoperative edema and hematoma formation.
Surgical Warning: Immediately before the tourniquet is removed, the hand must be elevated and kept constantly elevated. Releasing the tourniquet while the hand is in a dependent position invites a massive, rapid influx of arterial blood against a closed venous system, leading to catastrophic venous engorgement, reactive hyperemia, and immediate hematoma formation within the surgical dead spaces.
BIOMECHANICS OF IMMOBILIZATION AND PEDIATRIC CONSIDERATIONS
The Position of Safe Immobilization
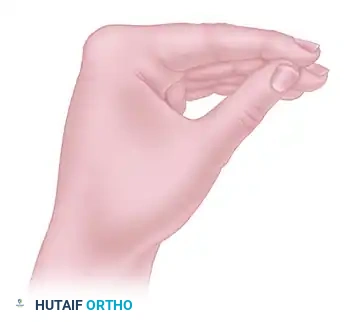
Unless specifically contraindicated by the nature of the repair (e.g., flexor tendon repairs requiring specific dynamic splinting protocols), the hand should be immobilized in the intrinsic-plus position (James position). This involves:
* Wrist: 20 to 30 degrees of extension.
* Metacarpophalangeal (MCP) Joints: 70 to 90 degrees of flexion.
* Interphalangeal (IP) Joints: Full extension.
This position maintains the collateral ligaments of the MCP joints at their maximal length (preventing extension contractures) and the volar plates of the IP joints at their maximal length (preventing flexion contractures).
Pediatric Splinting Challenges
Splints and bandages on pediatric patients present a unique challenge, as they tend to slip distally due to the conical shape of the child's forearm and the child's inherent non-compliance and high activity level.
To control this effectively, the surgeon should apply a long arm splint or a long arm cast. Furthermore, enclosing the entire extremity in a tube of stockinette that is secured proximally prevents the child from pulling the dressing off or introducing foreign bodies into the cast.
EDEMA CONTROL: THE CORNERSTONE OF RECOVERY
Edema is the primary enemy of hand function. Protein-rich fluid that accumulates in the interstitial spaces of the hand rapidly organizes into a fibrinous glue, which subsequently matures into dense scar tissue, binding the gliding planes of tendons and tethering joint capsules.
Strict Elevation Protocols
Elevation of the operative extremity should be maintained rigorously for at least 48 hours postoperatively. Effective elevation requires the hand to be positioned above the level of the heart. This can be achieved through several modalities:
1. Pillow Support: Positioning the hand on a firm pillow resting on the patient's chest while supine.
2. Overhead Suspension: Utilizing light overhead suspension that elevates the hand and forearm vertically while the elbow rests comfortably on the bed.
3. Sponge Blocks: Using a preformed, commercially available rubber sponge block designed specifically to cradle the arm at the correct angle of elevation.
Bed Rest vs. Ambulatory Slings
Bed rest for 3 days or longer is strongly recommended after major reconstructive surgery on the hand. General body activity increases cardiac output and peripheral blood flow, which paradoxically increases edema in the dependent hand.
Merely supporting the hand in a standard arm sling while the patient is ambulatory is highly ineffective for edema control. In a standard sling, the hand often rests at or below the level of the heart, allowing gravity to promote venous pooling and interstitial fluid accumulation.
WOUND SURVEILLANCE AND SCAR MANAGEMENT
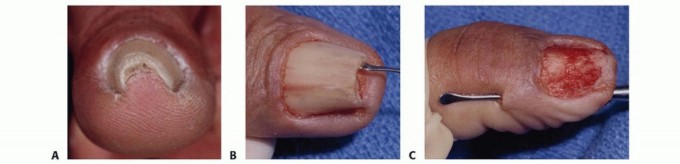
Inspection and Suture Removal
Even when no complications are suspected, it is a safe and highly recommended practice to inspect the wound at approximately 7 days postoperatively. This "window" inspection prevents unpleasant surprises and allows for the timely, aggressive management of unexpected superficial infections, hematomas, or marginal skin necrosis.
Sutures of non-absorbable nylon or stainless steel may not require removal until the splint is definitively discarded, which is usually at 3 or 4 weeks depending on the procedure. Complete redressing during the intermediate period may be unnecessary unless a hematoma or infection is clinically suspected (e.g., throbbing pain, systemic fever, malodor). In these instances, the dressing must be opened immediately under sterile conditions, the wound inspected, and the splint reapplied.
Surgical Planning for Scar Optimization
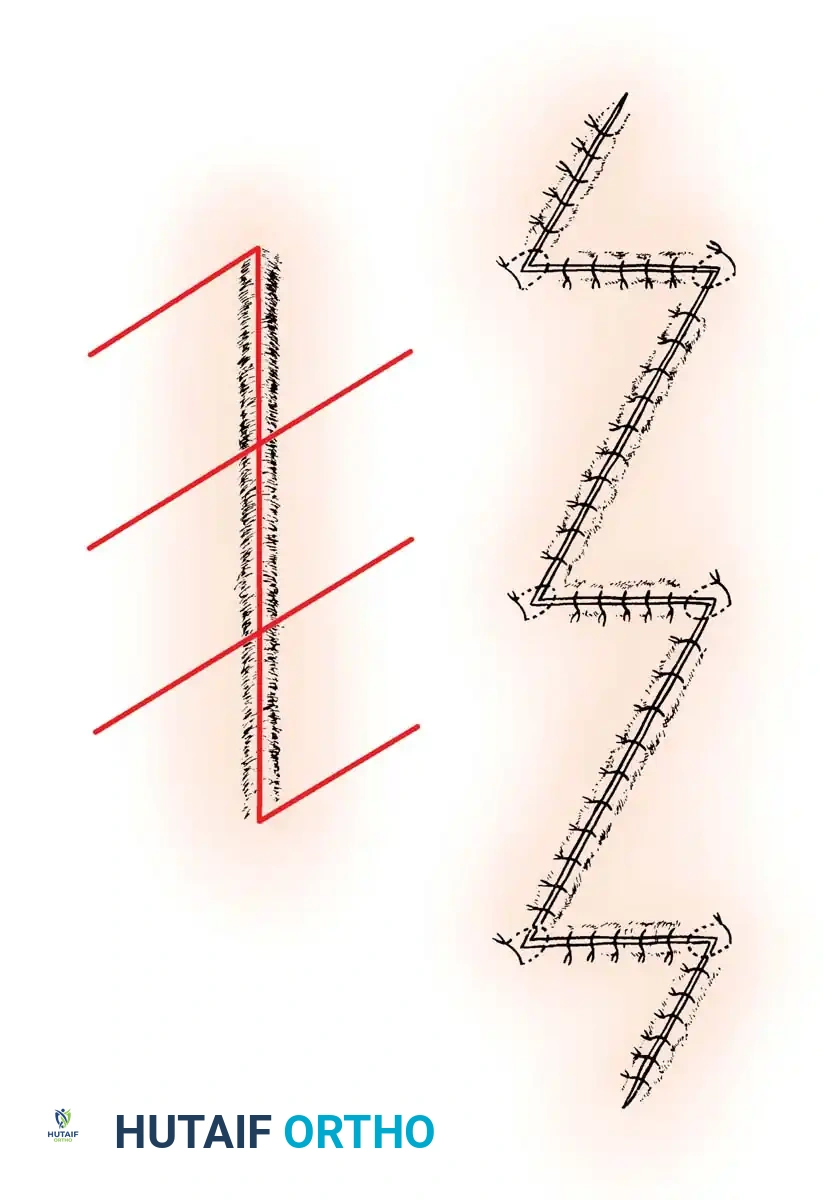
The prevention of debilitating scar contractures begins with intelligent surgical incision planning and extends into postoperative scar management. Linear scars that cross flexion creases perpendicularly are prone to severe longitudinal hypertrophy and contracture, which can severely limit joint extension.
When a surgeon is faced with a scar that is too long to be released by a single Z-plasty, or when planning an extensive exposure that crosses multiple flexion zones, multiple Z-plasties are indicated.
As illustrated above, multiple Z-plasties effectively break up the linear tension of a long scar, redistributing the contractile forces laterally and lengthening the overall scar line. This technique is invaluable in postoperative rehabilitation, as it allows for earlier and more aggressive range of motion without the risk of wound dehiscence or the development of a restrictive bowstring scar.
REHABILITATION AND MULTIDISCIPLINARY HAND THERAPY
Active use of the hand is unequivocally the most effective way to reestablish motion after surgery. The transition from immobilization to active rehabilitation must be guided by the biological timeline of tissue healing.
Proximal Joint Management
A common pitfall in hand surgery is the neglect of the proximal joints. Fingers that are not explicitly splinted for protection should be exercised actively and frequently.
Furthermore, the shoulder is highly susceptible to becoming stiff (adhesive capsulitis), especially in older patients. To prevent this, the shoulder should be abducted and elevated toward the head through a full range of motion several times daily.
Clinical Pearl: Compliance with proximal joint exercises is notoriously poor. Patients should be instructed to perform their shoulder abduction and elevation exercises at a specific, recurring daily event—such as at each mealtime—to build a reliable habit.
The Role of the Hand Therapist
The development of the specialized field of hand therapy has been of immeasurable importance in assisting patients in their recovery. Physical therapy and occupational therapy techniques, protocols, and modalities are essential in educating the patient to reintegrate the hand and upper extremity into vocational, recreational, and other activities of daily living (ADLs).
Two points are especially critical in the postoperative care paradigm:
1. The Multidisciplinary Team: The patient, the hand therapist, and the surgeon must function as a well-integrated team. They must plan and organize the patient’s course of treatment collaboratively, with regular, scheduled opportunities to evaluate functional progress. In most clinical settings, the surgeon must take the lead in planning, prescribing the specific biomechanical limitations, and monitoring the overall therapy program.
2. Pain as a Guide: The patient should never be required to carry out movements of the hand that are markedly painful. While mild discomfort and stretching sensations are expected, sharp or severe pain is a biological warning sign. The exact cause of the pain should be sought immediately (e.g., tendon subluxation, hardware failure, infection, or complex regional pain syndrome). If necessary, the part should be re-splinted until the pathology is resolved.
Contraindications in Therapy
Certain modalities and techniques are strictly contraindicated during the postoperative phase:
* Dependent Heat: Applying excessive heat to the hand while it is held in a dependent position is strictly contraindicated. Heat causes profound vasodilation; combined with gravity, this will result in massive, rapid edema formation.
* Forced Passive Manipulation: Forced passive manipulation of stiff joints by the patient, the therapist, or the surgeon is absolutely contraindicated. Aggressive passive stretching tears the delicate, healing collagen fibers, inducing micro-hemorrhage and a renewed inflammatory cascade. This inevitably results in increased fibrosis, thicker scar tissue, and ultimately, a stiffer joint. Motion must be regained through active and active-assisted modalities, allowing the patient's own pain threshold to dictate the limits of the stretch.
Return to Work and Psychological Well-being
Often, the most effective occupational therapy is the patient’s usual work. If biomechanically safe and possible, patients should be offered the opportunity to return to work as an integrated part of their treatment protocol, even if on a limited, light-duty, or modified basis.
The return to the activities of daily living and the vocational environment provides continuous, functional active range of motion. Furthermore, it has a profoundly beneficial psychological effect, preventing the depression and loss of identity that frequently accompany prolonged disability, thereby driving better overall clinical outcomes.
You Might Also Like