Pediatric Cervical Spine: Odontoid Anomalies & Surgery
Key Takeaway
Congenital anomalies of the pediatric cervical spine, particularly os odontoideum, present significant risks of atlantoaxial instability and compressive myelopathy. This comprehensive guide details the embryology, vascular anatomy, and radiographic evaluation of odontoid anomalies. It provides step-by-step surgical techniques for atlantoaxial and occipitocervical fusion, emphasizing biomechanical principles, preoperative traction, and precise graft placement to ensure optimal neurological outcomes in pediatric patients.
Pediatric Cervical Spine: Anomalies of the Odontoid
Although congenital anomalies of the pediatric cervical spine—specifically those involving the odontoid process (dens)—are relatively rare, they represent a critical diagnostic and therapeutic challenge for the orthopedic surgeon. These anomalies can precipitate profound atlantoaxial instability, leading to catastrophic neurological consequences, including compressive myelopathy, vertebral artery compression, or sudden death from minor trauma.
Anomalies of the odontoid are frequently detected as incidental findings following minor cervical trauma or when insidious neurological symptoms prompt advanced imaging. A comprehensive understanding of the embryology, vascular anatomy, and biomechanics of the craniovertebral junction is mandatory for any surgeon managing these complex pediatric deformities.
Classification of Odontoid Anomalies
Congenital anomalies of the odontoid are broadly categorized into three distinct morphological groups:
- Aplasia (Agenesis): The complete absence of the odontoid process. This is exceedingly rare and results in profound C1-C2 instability.
- Hypoplasia: Partial development of the odontoid. The osseous structure varies from a diminutive, peg-like projection to a slightly undersized dens.
- Os Odontoideum: The most clinically significant anomaly. The odontoid presents as an independent, oval or round ossicle with a smooth, sclerotic cortical border. It is separated from the body of the axis (C2) by a transverse gap, leaving the apical segment devoid of structural support.
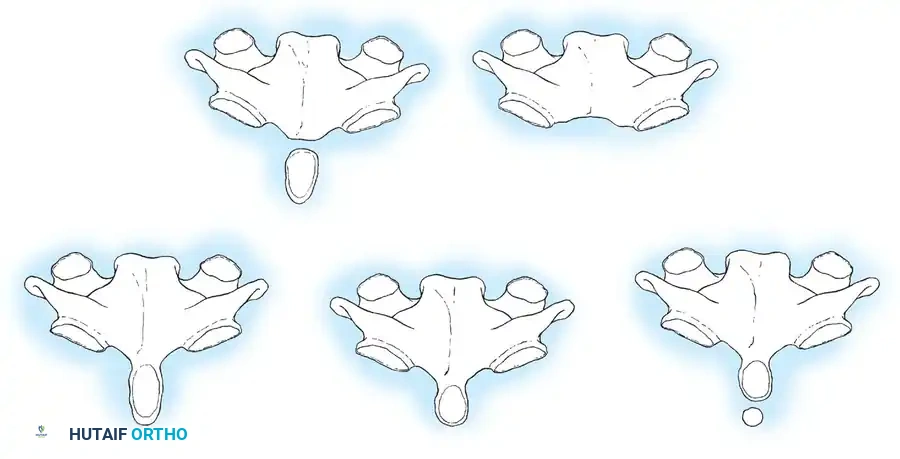
Fig. 37-1 Types of odontoid anomalies. A, Normal odontoid. B, Hypoplastic odontoid. C, Ossiculum terminale. D, Os odontoideum. E, Aplasia of odontoid.
The ossicle in os odontoideum is of variable size. It is typically located in the anatomical position of the normal odontoid (orthotopic), though it may occasionally be displaced superiorly near the occiput in the region of the foramen magnum (dystopic).
Clinical Pearl: Odontoid anomalies exhibit a higher prevalence in patients with specific syndromic conditions, including Down syndrome, Klippel-Feil syndrome, Morquio syndrome, and spondyloepiphyseal dysplasia. A high index of suspicion must be maintained when evaluating these populations.
Embryology and Vascular Anatomy
Knowledge of the embryological development and vascular supply of the odontoid is essential to understanding the etiology of these anomalies.
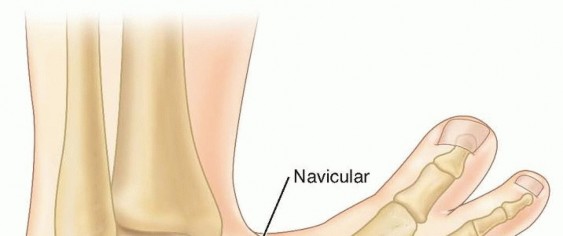
The odontoid process is derived from the mesenchyme of the first cervical vertebra (atlas). During normal embryogenesis, it separates from the atlas and fuses with the body of the axis. A vestigial disc space between C1 and C2 forms a synchondrosis within the body of the axis. The apex (tip) of the odontoid is derived from the most caudal occipital sclerotome, known as the proatlas. This separate ossification center, the ossiculum terminale, appears at approximately 3 years of age and typically fuses by age 12. Anomalies isolated to this terminal portion rarely cause clinical instability.

Fig. 37-2 Anteroposterior open-mouth odontoid view showing V-shaped dens bicornis and ossiculum terminale.
The arterial blood supply to the odontoid is highly specialized and derived from both the vertebral and carotid arteries.
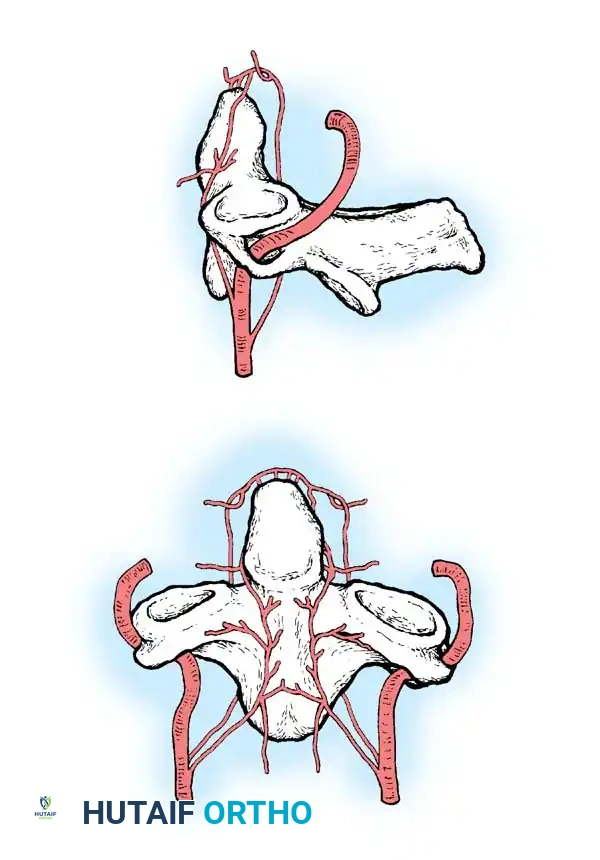
Fig. 37-3 Blood supply to odontoid: posterior and anterior ascending arteries and apical arcade.
The vertebral artery gives off anterior and posterior ascending arteries that originate at the level of C3. These vessels ascend anterior and posterior to the odontoid, anastomosing superiorly to form an apical arcade. Furthermore, the most rostral portion of the extracranial internal carotid artery provides "cleft perforators" that supply the superior pole of the odontoid.
Surgical Warning: This peculiar vascular arrangement is a biomechanical vulnerability. The synchondrosis prevents direct vascularization of the odontoid from the C2 body, and the surrounding synovial joint cavity of the atlantoaxial articulation prevents vascular ingrowth from C1. This watershed vascularity heavily predisposes the odontoid to nonunion and osteonecrosis following trauma.
Etiology: Congenital vs. Acquired
The etiology of os odontoideum remains a subject of academic debate, with evidence supporting both congenital and acquired (post-traumatic) origins.
- Congenital Theory: Proposes a failure of fusion of the apex (ossiculum terminale) or a failure of fusion of the odontoid to the axis. However, this theory fails to explain why the gap in os odontoideum typically occurs at the level of the superior articulating facets of C2, rather than below the facets where the neurocentral synchondrosis is anatomically located.
- Acquired Theory: Extensive literature suggests that an unrecognized fracture at the base of the odontoid in early childhood is the most common cause. The distraction force exerted by the intact alar ligaments pulls the fractured tip away from its base, while the tenuous blood supply leads to osteonecrosis and subsequent nonunion. Acquired os odontoideum has also been well-documented following halo-pelvic traction, where excessive distraction forces compromise the apical arcade.
Clinical Presentation and Diagnosis
The clinical presentation of os odontoideum is highly variable. Patients may be entirely asymptomatic, presenting only after an incidental radiographic finding, or they may present with frank compressive myelopathy.
Common Symptoms:
* Mechanical neck pain and suboccipital headache (due to local irritation of the C1-C2 articulation).
* Torticollis.
* Neurological deficits ranging from transient paresis following minor trauma to progressive, complete myelopathy.
* Upper motor neuron signs (hyperreflexia, clonus, Babinski sign), weakness, loss of balance, and proprioceptive/sphincter disturbances.
* Vertebral Artery Compression: Cervical and brainstem ischemia can manifest as seizures, syncope, vertigo, and visual disturbances (Wallenberg-like syndrome).
Diagnostic Pearl: The lack of cranial nerve involvement is a critical localizing sign. It helps differentiate os odontoideum from other occipitovertebral anomalies (e.g., basilar invagination), as the spinal cord impingement in os odontoideum occurs strictly below the foramen magnum.
Radiographic Evaluation
Routine cervical spine radiography, including an open-mouth odontoid view, is the first line of investigation.

Fig. 37-4 Lateral radiograph (A) and open-mouth odontoid radiograph (B) showing os odontoideum.
- Aplasia: Appears as a slight depression between the superior articulating facets on the open-mouth view.
- Os Odontoideum: A distinct space is visible between the C2 body and the free ossicle. The ossicle is typically half the size of a normal dens, with smooth, sclerotic borders. This must be differentiated from an acute Type II odontoid fracture, which presents with a thin, irregular, non-sclerotic radiolucent line.
Dynamic Imaging and Instability Criteria:
Lateral flexion and extension radiographs are mandatory to document instability. In children, the free ossicle is fixed to the anterior arch of C1 and moves in unison with it. Therefore, measuring the relationship between C1 and the ossicle is futile.
Instead, instability is measured by projecting a line superiorly from the posterior body of the axis and measuring the distance to the posterior border of the anterior arch of the atlas.
* Significant Instability: > 3 mm in adults; > 4 to 5 mm in children.
* Space Available for the Cord (SAC): Measured from the posterior aspect of the odontoid/axis to the nearest posterior structure (posterior arch of C1). A SAC of < 13 mm is highly predictive of neurological injury.
Watanabe et al. defined specific radiographic parameters correlating with neurological symptoms:
1. Sagittal Plane Rotation Angle: > 20 degrees.
2. Instability Index: > 40%.
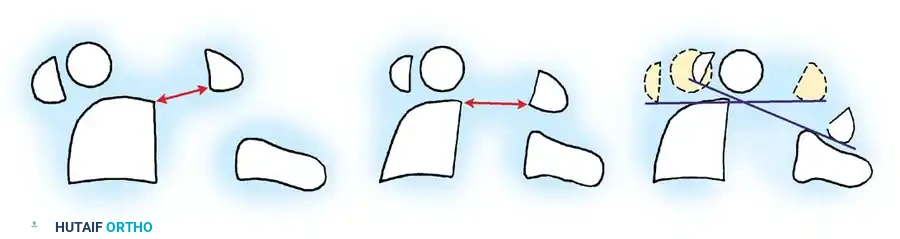
Fig. 37-5 Radiographic parameters. Minimal (A) and maximal (B) distance from posterior border of body of C2 to posterior atlantal arch. C, Change of atlantoaxial angle between flexion and extension position. a, sagittal plane rotation.
Advanced Imaging:
MRI is indispensable for evaluating the spinal cord for myelomalacia and identifying reactive retrodental soft-tissue masses (pannus) that occur with chronic instability. This reactive tissue can significantly decrease the SAC and cause compressive myelopathy even in the absence of severe dynamic subluxation.
Surgical Management
The primary objective of surgical intervention is to stabilize the abnormal atlantoaxial joint, preventing catastrophic subluxation that could lead to permanent spinal cord injury.
Indications for Operative Stabilization
Prophylactic stabilization of asymptomatic patients with < 5 mm of instability remains controversial. However, given the unpredictable nature of pediatric trauma, the risks of nonoperative management must be carefully weighed against surgical morbidity.
Box 37-1: Indications for Operative Stabilization of Os Odontoideum
* Neurological involvement (even if transient).
* Instability of > 5 mm posteriorly or anteriorly.
* Progressive instability documented on serial radiographs.
* Persistent neck complaints (pain, torticollis) associated with instability, refractory to conservative treatment.
Preoperative Preparation
In patients presenting with neurological deficits or severe subluxation, preoperative skeletal traction (e.g., Gardner-Wells tongs or halo ring) is highly recommended. Traction achieves gradual reduction, relieves spinal cord irritation, and allows for potential recovery of neurological function prior to surgical fusion. Achieving and maintaining anatomical reduction is the most critical prerequisite for a successful C1-C2 fusion.
Posterior Atlantoaxial Fusion Techniques
Before proceeding with a C1-C2 posterior fusion, the structural integrity of the posterior arch of C1 must be verified via CT scan. Incomplete development of the C1 posterior ring occurs with increased frequency in patients with os odontoideum and precludes standard wiring techniques.
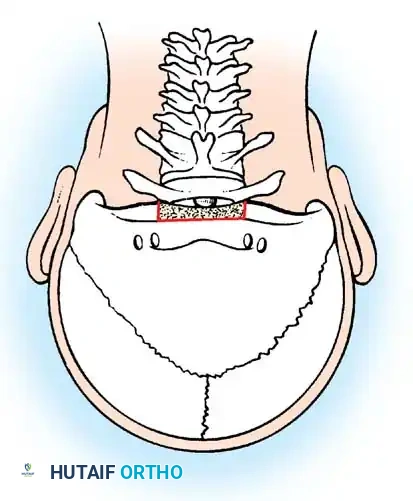
The Gallie Technique
The Gallie technique utilizes a single structural bone graft placed over the posterior arches of C1 and C2, secured with a single sublaminar wire passed beneath the arch of C1 and looped around the spinous process of C2.

Posterior wiring diagram demonstrating the passage of the wire.
- Advantage: Requires only one sublaminar wire passage (beneath C1), minimizing the risk of iatrogenic cord injury.
- Disadvantage: Biomechanically inferior in controlling rotational forces. Furthermore, tightening the wire can cause the unstable C1 vertebra to translate posteriorly, potentially fusing the spine in a subluxated position.
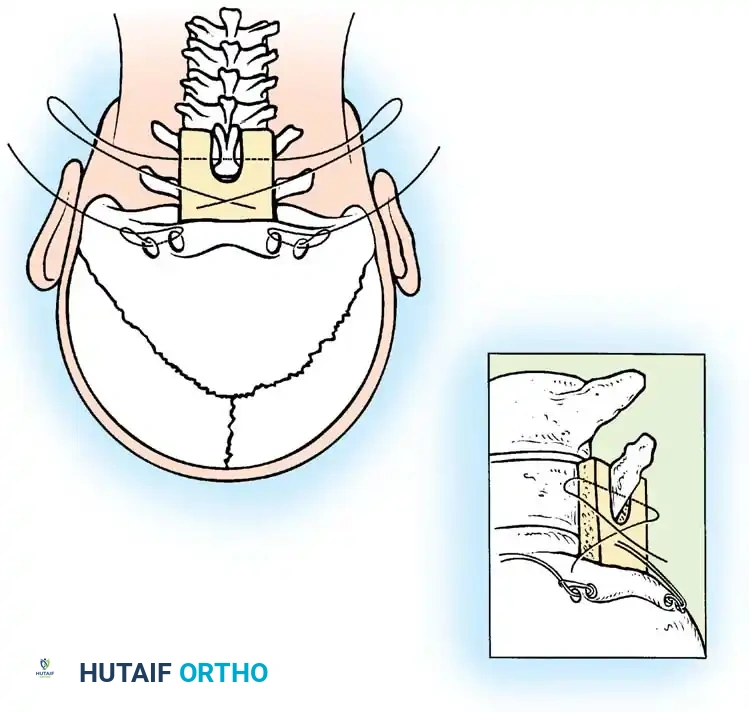
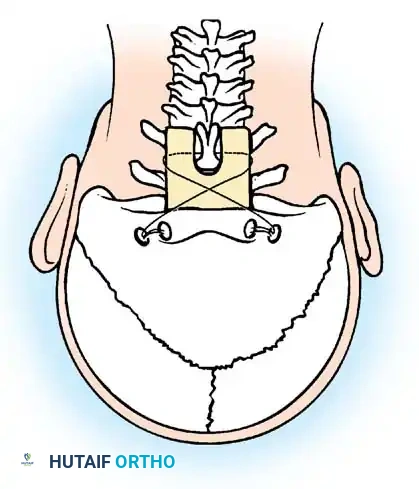
The Brooks-Jenkins Technique
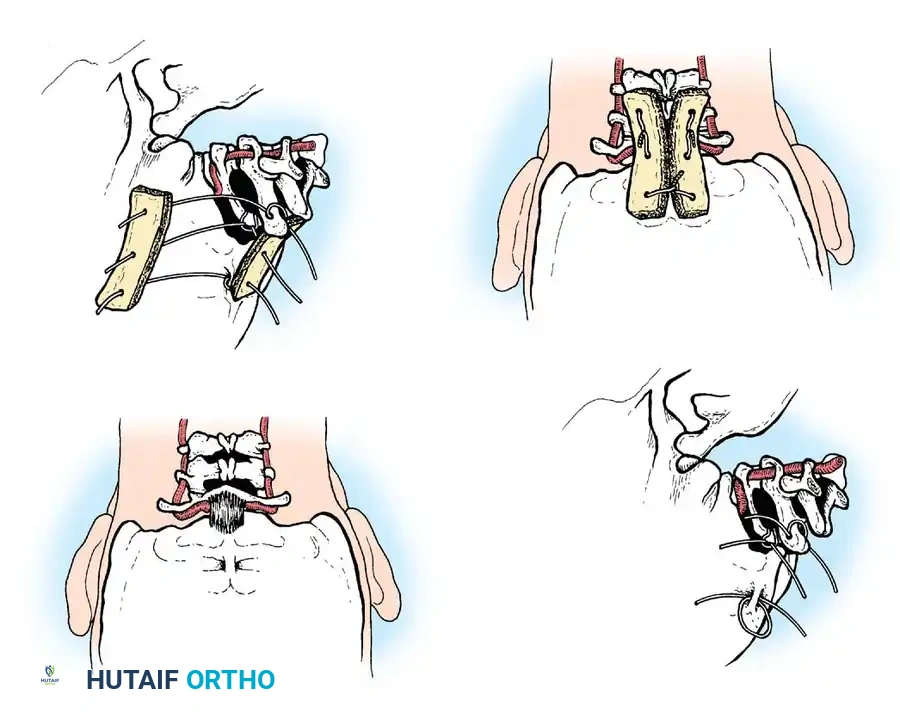
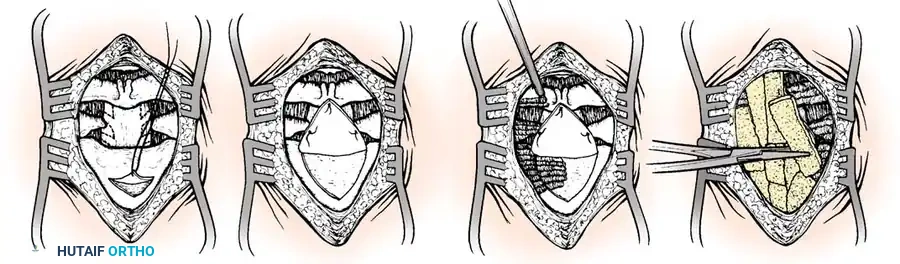
The Brooks-Jenkins technique provides superior biomechanical stability by utilizing two separate wedge-shaped bone grafts wedged between the lamina of C1 and C2, secured by bilateral sublaminar wires passed beneath both C1 and C2.
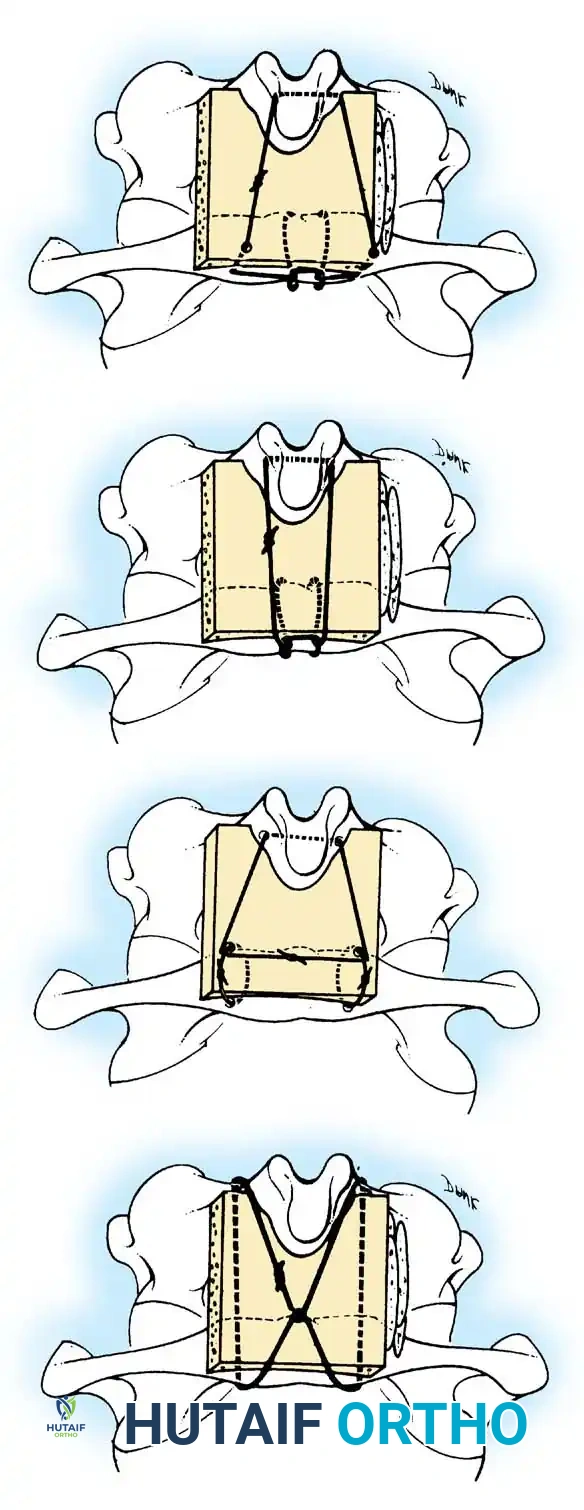
Sublaminar wire passage technique.
Preparation and shaping of the structural bone graft.
Placement of the bilateral bone grafts in the Brooks-Jenkins technique.
- Advantage: Excellent resistance to rotational movement, lateral bending, and extension. High fusion rates.
- Disadvantage: Requires the passage of sublaminar wires beneath both C1 and C2, increasing the risk of dural tear or spinal cord contusion, especially in a canal already compromised by instability.
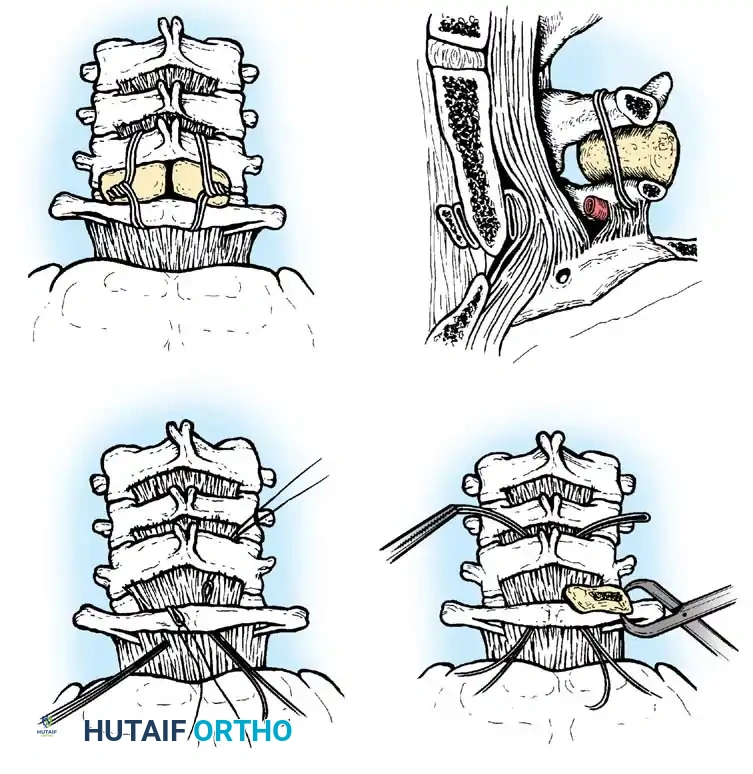
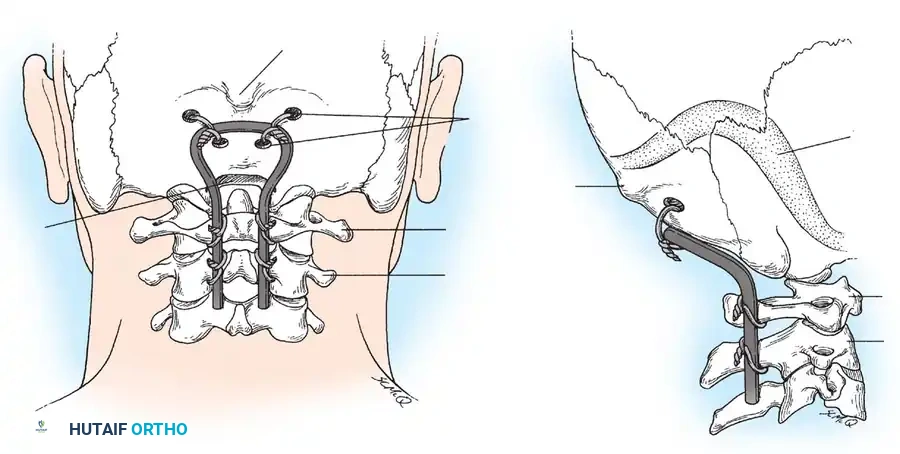
Occipitocervical Fusion
When the posterior arch of C1 is assimilated, hypoplastic, absent, or fractured, isolated C1-C2 fusion is impossible. In these scenarios, the fusion construct must be extended proximally to the occiput (Occipitocervical Fusion).
Historically, this was achieved using contoured rods or loops secured with sublaminar and cranial wiring, supplemented with autologous iliac crest bone graft.
Occipitocervical wiring technique.
Contoured loop for occipitocervical stabilization.
Occipitocervical construct utilizing contoured rods.
Detail of occipitocervical construct fixation.
Modern techniques favor rigid internal fixation using occipital plates and cervical pedicle or lateral mass screws. Regardless of the instrumentation used, meticulous decortication and the application of robust autologous bone graft are paramount for achieving arthrodesis.
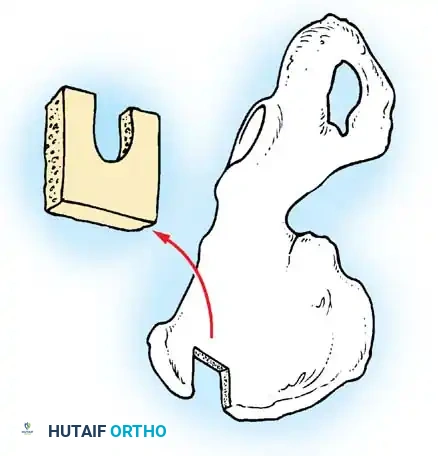
Harvesting and shaping of the occipitocervical bone graft.
Placement of the structural bone graft spanning the occiput to the cervical spine.
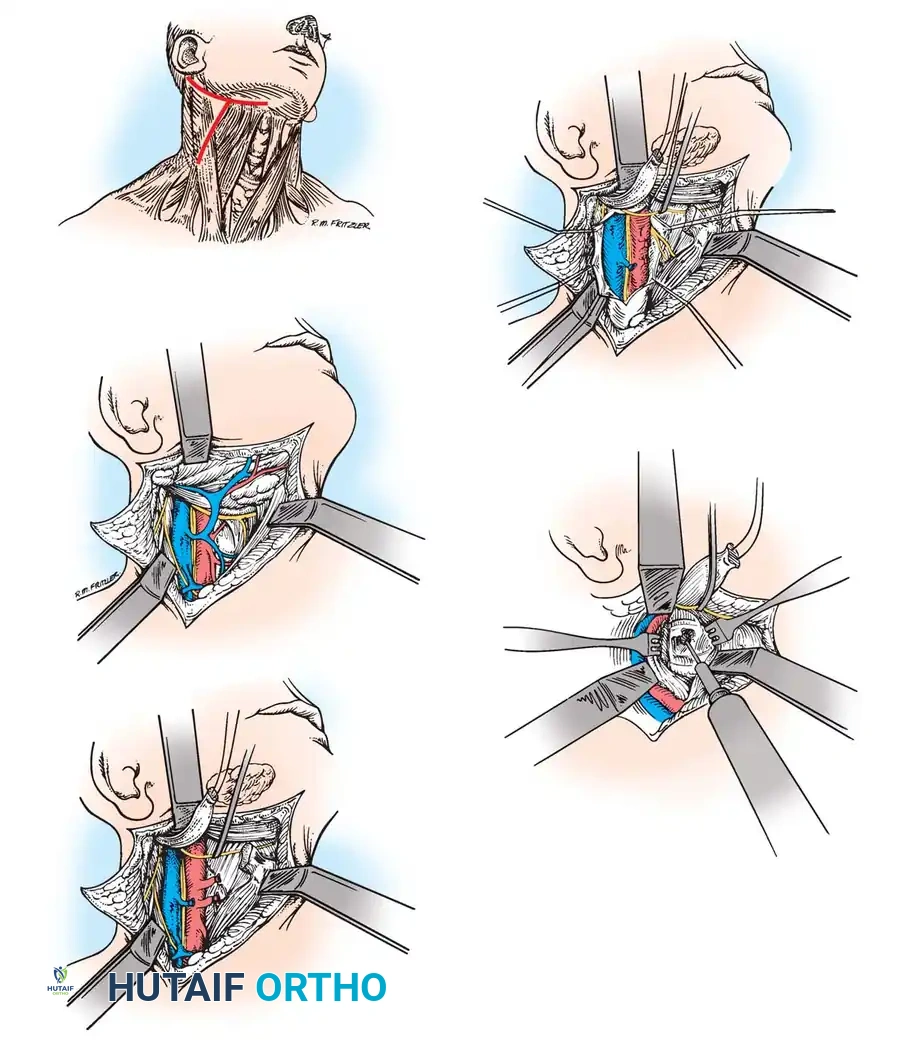
Anterior and Transoral Approaches
In rare instances, patients present with irreducible anterior spinal cord compression. This is typically caused by a fixed, posteriorly displaced os odontoideum or severe retrodental pannus that does not reduce with preoperative traction. In these cases, posterior fusion in situ is contraindicated as it would lock the spine in a stenotic state.
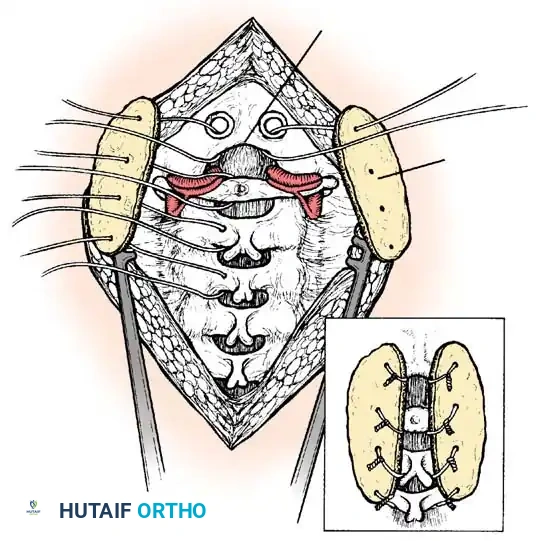
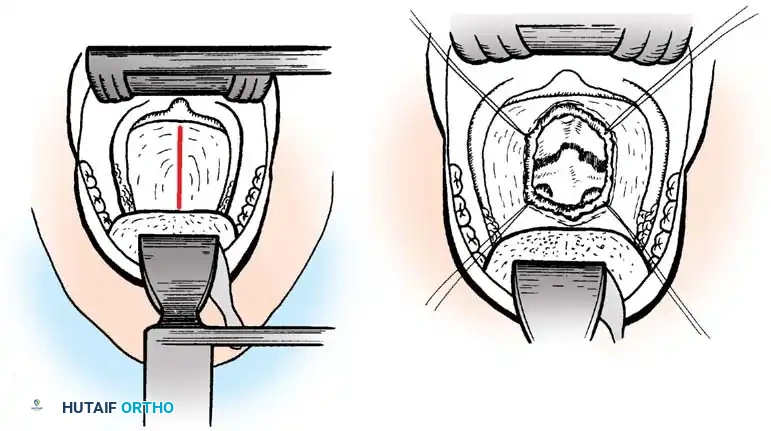
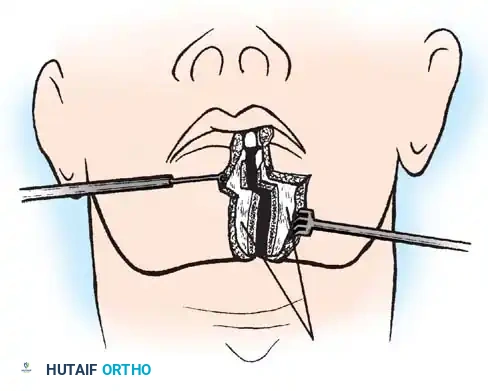
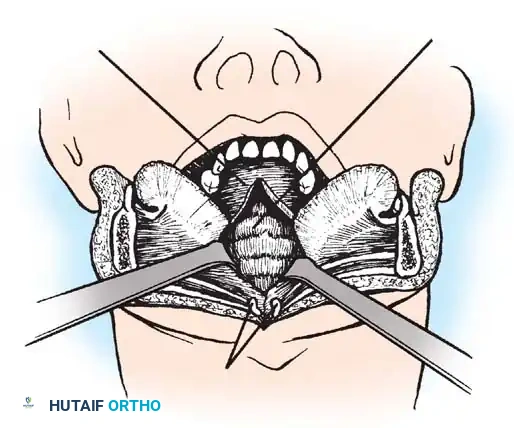
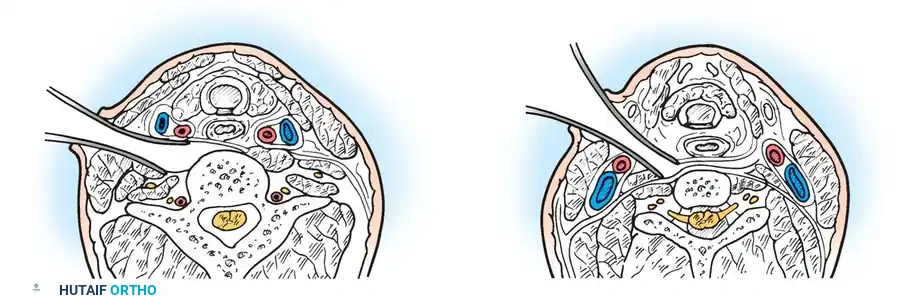
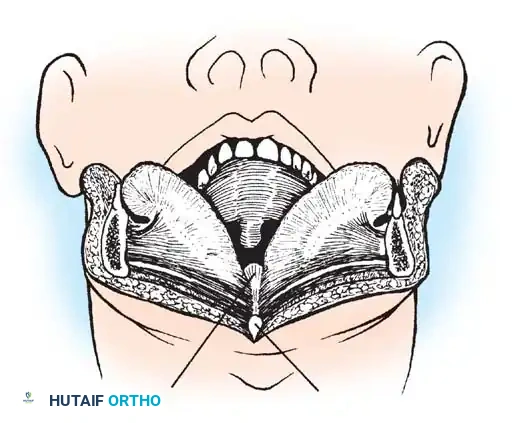
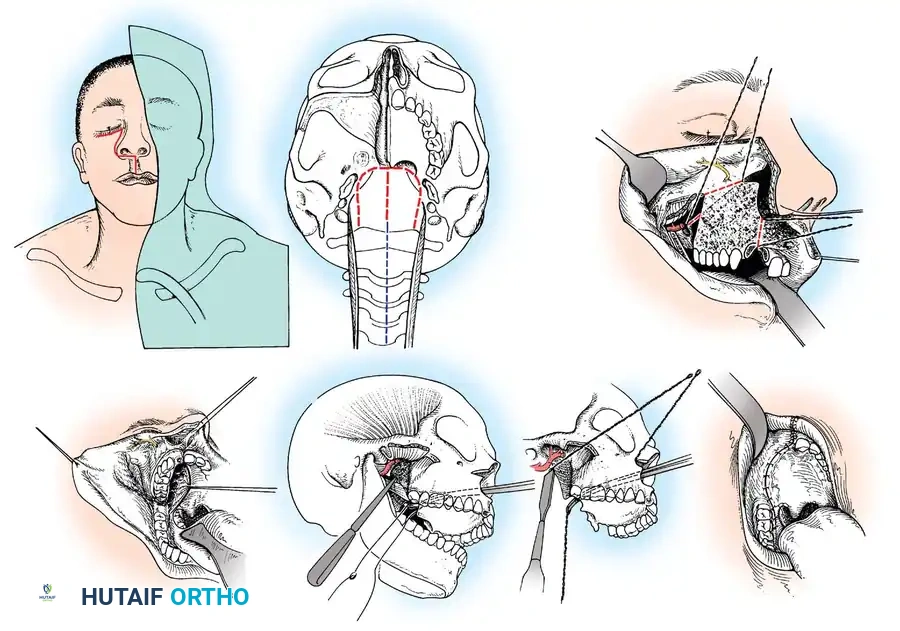
An anterior decompressive approach—specifically the Transoral-Transpharyngeal Approach—is required to resect the anterior arch of C1 and the compressive odontoid/ossicle, followed by a staged posterior stabilization.
Transoral Approach Steps:
1. Positioning and Retraction: The patient is positioned supine. A specialized transoral retractor (e.g
Associated Surgical & Radiographic Imaging
📚 Medical References
You Might Also Like