Mastering Benign Bone Tumors: Osteoblastoma, Chondromyxoid Fibroma, and Langerhans Cell Histiocytosis

Key Takeaway
Osteoblastoma is a rare, bone-forming neoplasm predominantly affecting the posterior elements of the spine in young adults. It presents with localized pain and potential neurological deficits. Management requires meticulous extended curettage or marginal resection, often necessitating complex spinal reconstruction. Langerhans cell histiocytosis, presenting frequently as vertebra plana or lytic lesions, is generally managed conservatively or with intralesional corticosteroid injection, reserving surgical decompression for progressive neurological compromise.
INTRODUCTION TO BENIGN AND TUMOR-LIKE BONE LESIONS
The diagnosis and management of benign bone tumors and tumor-like conditions require a rigorous, multidisciplinary approach. While these lesions lack metastatic potential, their local behavior can range from entirely quiescent to highly aggressive, leading to severe structural compromise, neurological deficits, and profound morbidity. This comprehensive masterclass details the pathophysiology, radiographic evaluation, and advanced surgical management of three distinct entities: Osteoblastoma, Chondromyxoid Fibroma, and Langerhans Cell Histiocytosis.
OSTEOBLASTOMA
Epidemiology and Clinical Presentation
Osteoblastoma is a rare, primary bone-forming neoplasm, accounting for less than 1% of all bone tumors. It predominantly affects adolescents and young adults, with peak incidence occurring between 10 and 30 years of age. There is a distinct male predominance, with a male-to-female ratio of approximately 3:1.
While osteoblastoma can arise in any bone, it exhibits a strong predilection for the axial skeleton. Approximately 40% to 50% of all lesions are located in the spine, almost exclusively originating in the posterior elements (spinous process, lamina, pedicles, and articular facets).
Clinically, the hallmark symptom is insidious, progressive pain. Unlike the pain of osteoid osteoma, which is classically nocturnal and dramatically relieved by nonsteroidal anti-inflammatory drugs (NSAIDs), the pain of osteoblastoma is often less responsive to salicylates and more constant.
Clinical Pearl: In the spine, osteoblastoma frequently induces a painful, rigid scoliosis. The lesion is typically located on the concave side of the scoliotic curve. In the lumbar spine, radiculopathy secondary to nerve root compression is common, whereas thoracic lesions are more likely to present with insidious spinal cord compression and myelopathy.
Radiographic and Histological Evaluation
Because osteoblastomas are slow-growing, symptoms may precede radiographic diagnosis by 1 to 2 years. The classic radiographic appearance is a well-circumscribed, expansile, bone-forming lesion in the posterior elements of the spine.

Anteroposterior and lateral radiographs of the cervical spine in a 10-year-old boy presenting with a 1-month history of severe neck pain, demonstrating a distinct lesion of the C3 spinous process.
Advanced imaging, particularly Computed Tomography (CT), is mandatory for preoperative planning. CT exquisitely delineates the osseous margins, the extent of cortical destruction, and the presence of matrix mineralization.

Axial and sagittal CT scans clearly defining the expansile, mineralized matrix of the osteoblastoma within the posterior elements, allowing for precise surgical planning.
Outside the spine, the radiographic appearance is highly variable and often non-specific. Lesions may be diaphyseal or metaphyseal, intramedullary or cortical, and can appear radiolucent, sclerotic, or mixed. The classic presentation of a calcified central nidus surrounded by a radiolucent halo and reactive sclerosis is occasionally seen.
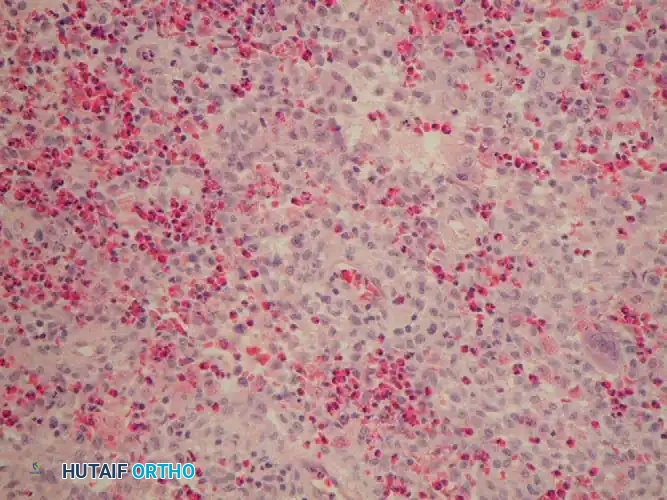
A 4-year-old boy with a 1-year history of right leg pain and antalgic gait. The right tibia was 2 cm longer than the left. Radiographs and CT reveal a lesion in the distal metaphysis causing bowing of the fibula, indicative of a chronic, benign process. The typical microscopic appearance confirms osteoblastoma.
Differential Diagnosis: The primary differential includes osteoid osteoma, aneurysmal bone cyst (ABC), and osteosarcoma. The distinction between osteoblastoma and osteoid osteoma is primarily based on size; by convention, a nidus greater than 1.5 cm is classified as an osteoblastoma.
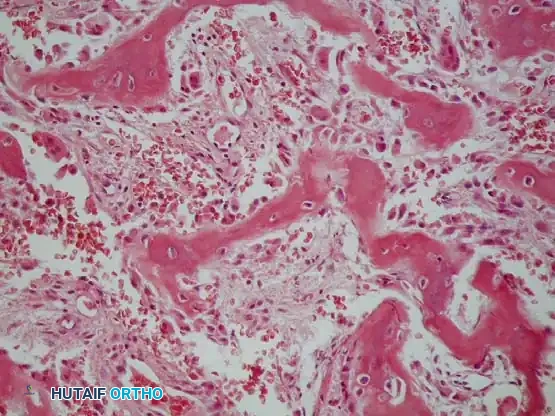
Histopathology: Microscopically, osteoblastoma is nearly identical to osteoid osteoma. It is characterized by a highly vascularized, fibrovascular stroma producing abundant osteoid and primitive woven bone.
Surgical Warning: The critical histological feature differentiating osteoblastoma from low-grade osteosarcoma is that the bony trabeculae in osteoblastoma are lined by a single, orderly layer of benign osteoblasts. Features favoring malignancy include permeation into surrounding host bone and sheets of atypical osteoblasts without intervening bone production.
Surgical Management of Osteoblastoma
The treatment of choice for osteoblastoma is extended intralesional curettage or marginal resection. Due to the tumor's vascularity, preoperative embolization should be strongly considered for large spinal or pelvic lesions to minimize intraoperative blood loss.
Step-by-Step Surgical Technique: Spinal Resection
- Positioning and Exposure: The patient is positioned prone on a radiolucent Jackson table. A standard midline posterior approach is utilized. Subperiosteal dissection must be performed meticulously to avoid penetrating the highly vascular tumor capsule.
- Tumor Isolation: Using fluoroscopy or intraoperative navigation, the exact levels are identified. The tumor is exposed, often revealing a thinned, expanded cortical shell.
- Resection: For posterior element lesions, an en bloc marginal resection (e.g., laminectomy/spinous process excision) is preferred over piecemeal curettage to minimize recurrence. A high-speed burr is used to disconnect the posterior elements from the pedicles.
- Neural Decompression: The ligamentum flavum is carefully resected, and the dura and exiting nerve roots are fully decompressed.
- Spinal Reconstruction: Because resection of the posterior elements and facets creates iatrogenic instability, instrumented posterolateral fusion is typically required. Lateral mass screws (cervical) or pedicle screws (thoracolumbar) are placed, and the defect is grafted with autograft or allograft.


Postoperative anteroposterior and lateral radiographs following marginal resection of the C3 osteoblastoma, demonstrating complete tumor removal and restoration of cervical alignment.
Adjuvant Therapies and Prognosis
The role of radiation therapy in osteoblastoma is highly controversial. Most orthopaedic oncologists strongly advise against radiation due to the documented risk of sarcomatous degeneration. Radiation is strictly reserved for symptomatic, anatomically inoperable lesions where surgical morbidity would be catastrophic.
Patients must be followed with serial radiographs of the primary site and chest CTs, as rare cases of "aggressive osteoblastoma" have been reported to metastasize or undergo malignant transformation.
CHONDROMYXOID FIBROMA: SURGICAL PRINCIPLES
Though distinct from osteoblastoma, Chondromyxoid Fibroma (CMF) is another rare benign bone tumor that requires meticulous surgical management. It typically presents in the second and third decades of life, most commonly in the metaphyseal regions of long bones, particularly the proximal tibia.
Clinical and Radiographic Presentation
Patients generally present with chronic, localized pain. Radiographically, CMF appears as an eccentric, sharply circumscribed, osteolytic lesion in the metaphysis. It often has a lobulated appearance with a sclerotic margin and may cause endosteal scalloping or cortical expansion.


Anteroposterior and lateral radiographs of a 36-year-old man with a 1-year history of right knee pain, demonstrating a chondromyxoid fibroma in its classic location—the proximal tibial metaphysis.
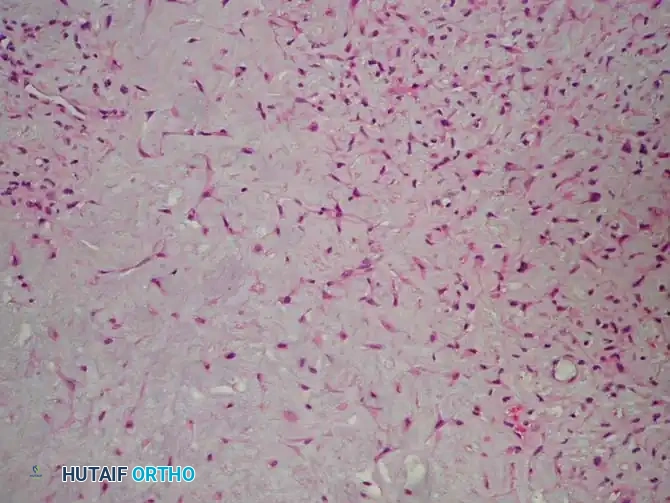
Typical microscopic appearance of chondromyxoid fibroma, showing a lobular architecture with chondroid, myxoid, and fibrous zones.
Operative Technique: Extended Curettage and Adjuvant Therapy
The standard of care for CMF is extended intralesional curettage. Simple curettage carries an unacceptably high recurrence rate (up to 25%); therefore, the use of local adjuvants is mandatory.

Anteroposterior and lateral radiographs of the right wrist in a 14-year-old boy showing a benign-appearing, expansile lesion in the distal radial metaphysis.
- Cortical Windowing: A generous cortical window is created over the lesion to allow complete visualization of the tumor cavity.
- Gross Curettage: The macroscopic tumor is removed using progressively smaller curettes, ensuring all lobulations and recesses are cleared.
- High-Speed Burring: A high-speed burr is used to aggressively remove an additional 1-2 mm of reactive bone from the cavity walls, breaking the microscopic tumor extensions.
- Chemical/Thermal Adjuvants: The cavity is treated with an adjuvant to induce necrosis of any remaining microscopic cells. Argon beam coagulation is highly effective, providing uniform thermal necrosis with minimal depth of penetration, thereby protecting adjacent articular cartilage.
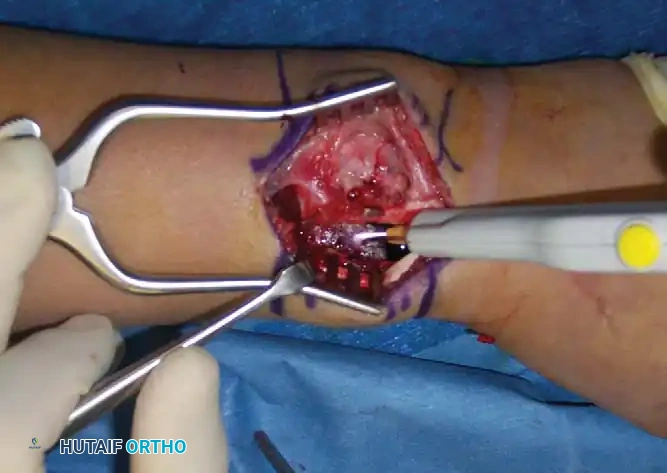
Intraoperative photograph demonstrating the tumor cavity after removal with curettes and a power burr, followed by treatment with argon beam coagulation to ensure marginal sterilization.
- Defect Reconstruction: The resulting void must be filled to restore structural integrity. Calcium phosphate bone graft substitutes, autograft, or allograft can be utilized depending on the defect size and mechanical demands.

The sterilized cavity is meticulously packed with a calcium phosphate bone graft substitute to provide immediate structural support and a scaffold for osteointegration.

Postoperative anteroposterior and lateral radiographs demonstrating complete filling of the defect and restoration of the distal radial anatomy.
LANGERHANS CELL HISTIOCYTOSIS (LCH)
Disease Spectrum and Classification
Langerhans Cell Histiocytosis (formerly Histiocytosis X) encompasses a spectrum of idiopathic disorders characterized by the clonal proliferation of Langerhans cells. The disease can affect virtually any organ system and is historically divided into three clinical syndromes:
1. Eosinophilic Granuloma: The localized form, restricted to isolated bone lesions. This is the most common presentation encountered by orthopaedic surgeons.
2. Hand-Schüller-Christian Disease: A chronic, disseminated form classically presenting with the triad of skull lesions, exophthalmos, and diabetes insipidus.
3. Letterer-Siwe Disease: An acute, disseminated, and frequently fatal multisystem disease occurring in infants under 3 years of age, characterized by hepatosplenomegaly, lymphadenopathy, and severe bone marrow involvement.
Clinical Presentation and Radiographic Findings
Eosinophilic granuloma typically affects children and young adults between 5 and 20 years of age. Patients present with localized, progressive pain, swelling, and occasionally systemic symptoms such as low-grade fever and elevated inflammatory markers.
Pitfall: The clinical and radiographic presentation of LCH in long bones can perfectly mimic acute osteomyelitis or Ewing sarcoma. A high index of suspicion and a low threshold for biopsy are required.
Radiographically, LCH is the great imitator.
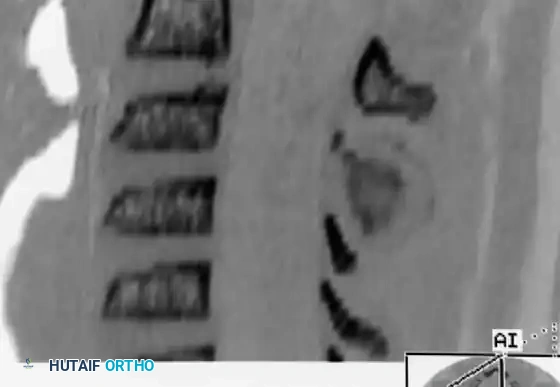
* Spine: LCH is the most common cause of vertebra plana (severe, uniform flattening of the vertebral body) in children. The intervertebral disc spaces are classically preserved, differentiating it from infectious spondylodiscitis.

Eosinophilic granuloma of the vertebral body. Severe compression of the body produces the classic radiographic changes of vertebra plana. The adjacent disc spaces remain intact.
- Flat Bones (Skull, Pelvis): Lesions appear as well-circumscribed, "punched-out" lytic defects. In the skull, uneven destruction of the inner and outer tables creates a characteristic "hole-within-a-hole" appearance.
- Long Bones: Diaphyseal lesions often exhibit an aggressive, permeative pattern of bone destruction with robust, lamellated periosteal
Associated Surgical & Radiographic Imaging

You Might Also Like

